Atrioventricular block
| Atrioventricular block | |
 | |
|---|---|
| ICD-10 | I44.0-I44.3 |
| ICD-9 | 426.0-426.1 |
| MeSH | D006327 |
|
Atrioventricular block Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Atrioventricular block On the Web |
|
American Roentgen Ray Society Images of Atrioventricular block |
|
Risk calculators and risk factors for Atrioventricular block |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: AV block
Overview
Historical Perspective
Classification
Pathophysiology
Causes
Differentiating Atrioventricular block from other Diseases
Epidemiology and Demographics
Risk Factors
Screening
Natural History, Complications and Prognosis
Treatment
- Remove extrinsic causes
- Treat reversible intrinsic causes
Pharmacotherapy
Acute Pharmacotherapies
- Pharmacologic interventions (Atropine, Isoproterenol, Theophylline)
Surgery and Device Based Therapy
- Temporary Pacing
- Permant Pacing
Indications for Surgery and Device Based Therapy
Indications for Permanent Pacemaker in Acquired Atrioventricular Block in Adults (AHA, 1998)
- Class I
- Third-degree AV block plus:
- Symptoms related to bradycardia
- Arrhythmia or other condition requiring nodal blockers
- Asystole > 3 seconds (while awake), ventricular rate <40
- Neuromeuscular disease
- Second Degree AV block plus:
- Symptomatic Bradycardia
- Third-degree AV block plus:
- Class II
- Asymptomatic Third-degree AV Block with HR >40
- Asymptomatic Type II, second-degreee AV Block
- Asymptomatic Type I, second-degree AV Block (with wide complex)
- Class III
- Asymptomatic Type I, second-degree AV block (with narrow complex)
ACC / AHA Guidelines- Recommendations for Acquired Atrioventricular Block in Adults (DO NOT EDIT) [1]
| “ |
Class I1. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with bradycardia with symptoms (including heart failure) or ventricular arrhythmias presumed to be due to AV block. (Level of Evidence: C) 2. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with arrhythmias and other medical conditions that require drug therapy that results in symptomatic bradycardia. (Level of Evidence: C) 3. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level in awake, symptom-free patients in sinus rhythm, with documented periods of asystole greater than or equal to 3.0 seconds86 or any escape rate less than 40 bpm, or with an escape rhythm that is below the AV node. (Level of Evidence: C) 4. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level in awake, symptom-free patients with AF and bradycardia with 1 or more pauses of at least 5 seconds or longer. (Level of Evidence: C) 5. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level after catheter ablation of the AV junction. (Level of Evidence: C) 6. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with postoperative AV block that is not expected to resolve after cardiac surgery. (Level of Evidence: C) 7. Permanent pacemaker implantation is indicated for third-degree and advanced second-degree AV block at any anatomic level associated with neuromuscular diseases with AV block, such as myotonic muscular dystrophy, Kearns-Sayre syndrome, Erb dystrophy (limb-girdle muscular dystrophy), and peroneal muscular atrophy, with or without symptoms. (Level of Evidence: B) 8. Permanent pacemaker implantation is indicated for second-degree AV block with associated symptomatic bradycardia regardless of type or site of block. (Level of Evidence: B) 9. Permanent pacemaker implantation is indicated for asymptomatic persistent third-degree AV block at any anatomic site with average awake ventricular rates of 40 bpm or faster if cardiomegaly or LV dysfunction is present or if the site of block is below the AV node. (Level of Evidence: B) 10. Permanent pacemaker implantation is indicated for second- or third-degree AV block during exercise in the absence of myocardial ischemia. (Level of Evidence: C) Class IIa1. Permanent pacemaker implantation is reasonable for persistent third-degree AV block with an escape rate greater than 40 bpm in asymptomatic adult patients without cardiomegaly. (Level of Evidence: C) 2. Permanent pacemaker implantation is reasonable for asymptomatic second-degree AV block at intra- or infra-His levels found at electrophysiological study. (Level of Evidence: B) 3. Permanent pacemaker implantation is reasonable for first- or second-degree AV block with symptoms similar to those of pacemaker syndrome or hemodynamic compromise. (Level of Evidence: B) 4. Permanent pacemaker implantation is reasonable for asymptomatic type II second-degree AV block with a narrow QRS. When type II second-degree AV block occurs with a wide QRS, including isolated right bundle-branch block, pacing becomes a Class I recommendation. (See Section 2.1.3, “Chronic Bifascicular Block.”) (Level of Evidence: B) Class IIb1. Permanent pacemaker implantation may be considered for neuromuscular diseases such as myotonic muscular dystrophy, Erb dystrophy (limb-girdle muscular dystrophy), and peroneal muscular atrophy with any degree of AV block (including first-degree AV block), with or without symptoms, because there may be unpredictable progression of AV conduction disease. (Level of Evidence: B) 2. Permanent pacemaker implantation may be considered for AV block in the setting of drug use and/or drug toxicity when the block is expected to recur even after the drug is withdrawn. (Level of Evidence: B) Class III1. Permanent pacemaker implantation is not indicated for asymptomatic first-degree AV block. (Level of Evidence: B) (See Section 2.1.3, “Chronic Bifascicular Block.”) 2. Permanent pacemaker implantation is not indicated for asymptomatic type I second-degree AV block at the supra-His (AV node) level or that which is not known to be intra- or infra-Hisian. (Level of Evidence: C) 3. Permanent pacemaker implantation is not indicated for AV block that is expected to resolve and is unlikely to recur (e.g., drug toxicity, Lyme disease, or transient increases in vagal tone or during hypoxia in sleep apnea syndrome in the absence of symptoms). (Level of Evidence: B) |
” |
Examples
-
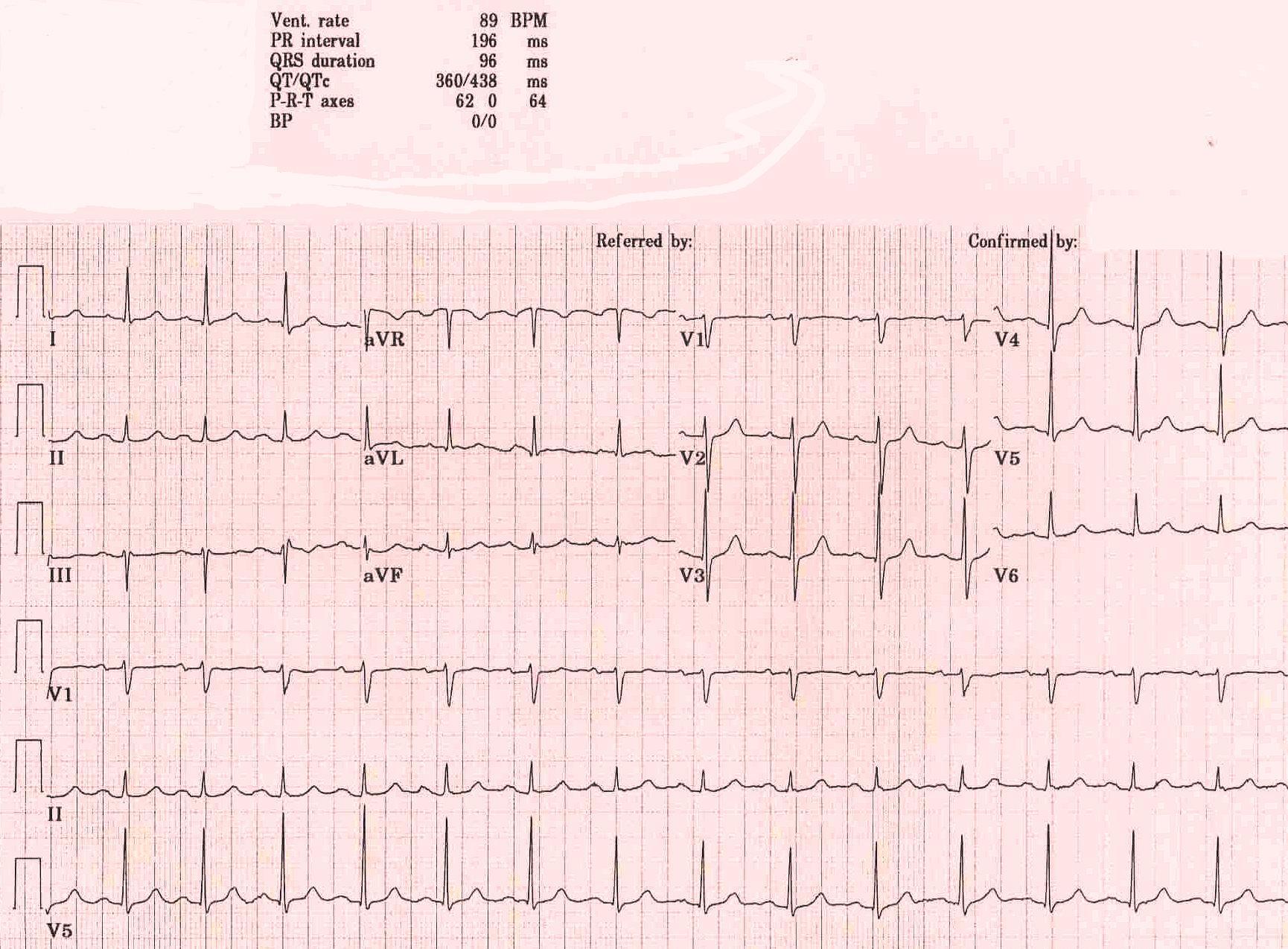
First degree AV block is a misnomer in that every P wave is conducted to the ventricles, however, with a PR interval exceeding 200 msec. Prolonged PR conduction, a more appropriate classification for this conduction disturbance, may be the result of conduction delay within the atrium, AV node, bundle of His or bundle branches. Prolongation of the PR interval most often indicates AV nodal conduction delay.
-
Two-to-one AV block can represent benign block within the AV node or disease of the His-Purkinje system. Certain electrocardiographic features and maneuvers can help in distinguishing where the location of block exists. A long PR interval with a narrow QRS suggests an intranodal block. A short PR interval with intraventricular conduction delay or bundle branch block suggests disease below the node. Responses to atropine, exercise and carotid sinus massage can be helpful in diagnosis. Atropine will improve AV nodal conduction but will worsen block within diseased His-Purkinje fibers. Exercise has a similar effect, improving conduction in cases where block exists only in the node, but worsening when block is subnodal. Alternatively, Carotid Sinus Massage will slow conduction when block occurs in the AV node, but will improve conduction in diseased His-Purkinje tissue by allowing for refractoriness to recover


Sources
- The ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities [1]
References
- ↑ 1.0 1.1 Epstein AE, DiMarco JP, Ellenbogen KA, Estes NAM III, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices). Circulation. 2008; 117: 2820–2840. PMID 18483207