Atrial flutter resident survival guide: Difference between revisions
| Line 110: | Line 110: | ||
{{familytree | | | |`|-|-|-|v|-|-|-|'| | | | | | | | }} | {{familytree | | | |`|-|-|-|v|-|-|-|'| | | | | | | | }} | ||
{{familytree | | | | | | | D01 | | | | | | | | | | |D01=<div style="float: left; text-align: left;padding:1em "> ❑ Assess need for therapy to prevent recurrence </div> |D02=}} | {{familytree | | | | | | | D01 | | | | | | | | | | |D01=<div style="float: left; text-align: left;padding:1em "> ❑ Assess need for therapy to prevent recurrence </div> |D02=}} | ||
{{familytree | |,|-|-|- | {{familytree | |,|-|-|v|-|-|^|-|-|v|-|-|.| | | | | | | | | | | | | | | }} | ||
{{familytree | H01 | {{familytree | H01 | H02 | H03 | H04 | H05 | | | | | | | | | |H01=<table class="wikitable"> | ||
<tr><td>▸ '''''First episode and well-tolerated atrial flutter'''''</td><td>▸ '''''Cardioversion alone ([[ACC AHA guidelines classification scheme|class I, level of evidence B]])''''' <br> or <br> ▸ '''''Catheter ablation ([[ACC AHA guidelines classification scheme|class IIa, level of evidence B]])'''''</td></tr></table>|H02=<table class="wikitable"><tr><td>▸ '''''Recurrent and well-tolerated atrial flutter'''''</td><td>▸ '''''Catheter ablation([[ACC AHA guidelines classification scheme|class I, level of evidence B]])'''''<br> or <br>▸ '''''Dofetilide ([[ACC AHA guidelines classification scheme|class IIa, level of evidence C]])'''''<br> or <br>▸ '''''Amiodarone ([[ACC AHA guidelines classification scheme|class IIb, level of evidence C]]) <br>or<br> Sotalol <br>or<br> Flecainide <br>or<br> Quinidine <br>or<br> Propafenone <br>or<br> Procainamide <br>or<br> Disopyramide''''' </td></tr></table> |H03=<table class="wikitable"><tr><td>▸ '''''Poorly tolerated atrial flutter'''''</td><td> ▸ '''''Catheter ablation ([[ACC AHA guidelines classification scheme|class I, level of evidence B]])'''''</td></tr></table> |H04=<table class="wikitable"><tr><td>▸ '''''Atrial flutter appearing after use of class Ic agents or amiodarone for treatment of AF'''''</td><td>▸ '''''Catheter ablation ([[ACC AHA guidelines classification scheme|class I, level of evidence B]])''''' <br> or <br>▸ '''''Stop current drug and use another ([[ACC AHA guidelines classification scheme|class IIa, level of evidence C]])'''''</td></tr></table> |H05=<table class="wikitable"><tr><td>▸ '''''Symptomatic non–CTI-dependent flutter after failed antiarrhythmic drug therapy'''''</td><td>'''''Catheter ablation ([[ACC AHA guidelines classification scheme|class IIa, level of evidence B]])'''''</td></tr></table> }} | <tr><td>▸ '''''First episode and well-tolerated atrial flutter'''''</td><td>▸ '''''Cardioversion alone ([[ACC AHA guidelines classification scheme|class I, level of evidence B]])''''' <br> or <br> ▸ '''''Catheter ablation ([[ACC AHA guidelines classification scheme|class IIa, level of evidence B]])'''''</td></tr></table>|H02=<table class="wikitable"><tr><td>▸ '''''Recurrent and well-tolerated atrial flutter'''''</td><td>▸ '''''Catheter ablation([[ACC AHA guidelines classification scheme|class I, level of evidence B]])'''''<br> or <br>▸ '''''Dofetilide ([[ACC AHA guidelines classification scheme|class IIa, level of evidence C]])'''''<br> or <br>▸ '''''Amiodarone ([[ACC AHA guidelines classification scheme|class IIb, level of evidence C]]) <br>or<br> Sotalol <br>or<br> Flecainide <br>or<br> Quinidine <br>or<br> Propafenone <br>or<br> Procainamide <br>or<br> Disopyramide''''' </td></tr></table> |H03=<table class="wikitable"><tr><td>▸ '''''Poorly tolerated atrial flutter'''''</td><td> ▸ '''''Catheter ablation ([[ACC AHA guidelines classification scheme|class I, level of evidence B]])'''''</td></tr></table> |H04=<table class="wikitable"><tr><td>▸ '''''Atrial flutter appearing after use of class Ic agents or amiodarone for treatment of AF'''''</td><td>▸ '''''Catheter ablation ([[ACC AHA guidelines classification scheme|class I, level of evidence B]])''''' <br> or <br>▸ '''''Stop current drug and use another ([[ACC AHA guidelines classification scheme|class IIa, level of evidence C]])'''''</td></tr></table> |H05=<table class="wikitable"><tr><td>▸ '''''Symptomatic non–CTI-dependent flutter after failed antiarrhythmic drug therapy'''''</td><td>'''''Catheter ablation ([[ACC AHA guidelines classification scheme|class IIa, level of evidence B]])'''''</td></tr></table> }} | ||
Revision as of 15:43, 12 March 2014
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hilda Mahmoudi M.D., M.P.H.[2]; Priyamvada Singh, M.D. [3]
Definition
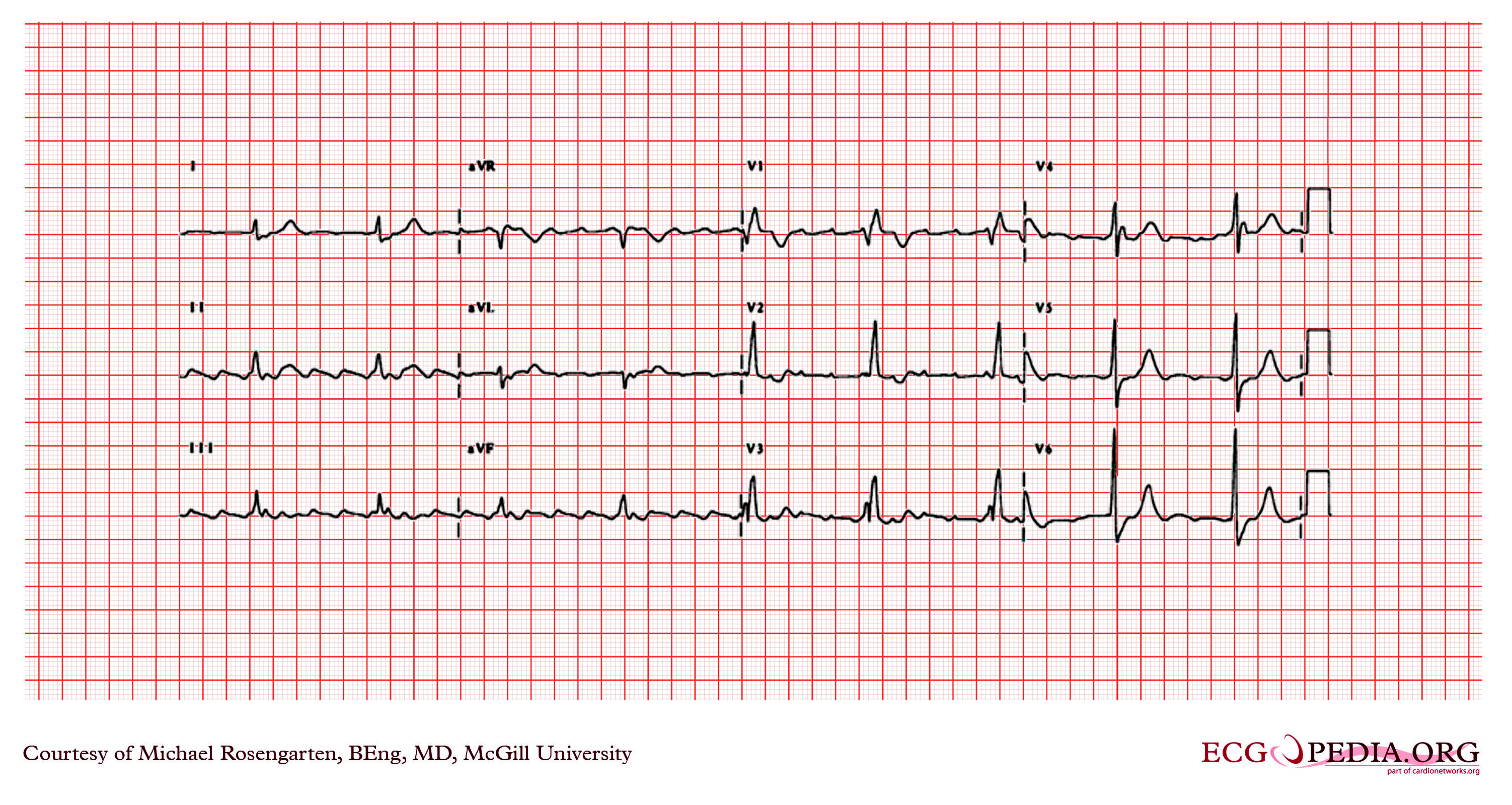
Atrial flutter is a reenterant arrhythmia, with atrial rates between 240 and 340/min, with a regular ventricular response and a saw tooth pattern on EKG.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated. Atrial flutter can be a life-threatening condition and must be treated as such irrespective of the causes.
Common Causes
- Acute coronary syndromes
- Cardiomyopathy
- Carbon monoxide poisoning
- Congenital heart disease
- Hypertensive heart disease
- Hyperthyroidism
- Mitral valve disease[1] [2]
- Pulmonary embolism
- Myocardial infarction
Management
Diagnostic Approach
Shown below is an algorithm summarizing the initial approach to atrial fibrillation.
Characterize the symptoms:
Characterize the timing of the symptoms:
❑ Duration
| |||||||||||||||||||||||||||||||||||
Identify possible triggers:
| |||||||||||||||||||||||||||||||||||
❑ Examine the patient ❑ Order an ECG ♦ Atrial flutter rhythm
| |||||||||||||||||||||||||||||||||||
❑ Order a transthoracic echocardiogram | |||||||||||||||||||||||||||||||||||
Therapeutic Approach
Shown below is an algorithm summarizing the therapeutic approach to atrial flutter.[3]
| Atrial flutter | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Unstable | Stable | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
❑ Look for the presence of any of these: ❑ If present, attempt direct DC cardioversion and then rate control measures as shown in the table below:
| ❑ Administer anticoagulation therapy based on the risk of stroke, if total duration of flutter > 48 hours ❑ Administer rate control therapy as shown in table below:
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
❑ Attempt conversion as shown in table below:
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
❑ Assess need for therapy to prevent recurrence | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||
Acute management of atrial flutter
| ||||||||||||
| ||||||||||||
Long term management of atrial flutter
| |||||||||||||||
Heart Rate Control
Shown below is a table summarizing the list of recommended agents for control of heart rate and their dosages.[4]
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Pharmacological cardioversion
| ||||||||||||
Antiarrhythmic Therapy
| |||
Anticoagulation Therapy
Shown below are tables depicting the assessment of risk of stroke and the appropriate anticoagulation therapy among patients with Atrial flutter.[4]
| ||||||||
| ||||||||
Do's
Don'ts
References
- ↑ Gutierrez SD, Earing MG, Singh AK, Tweddell JS, Bartz PJ (2012). "Atrial Tachyarrhythmias and the Cox-maze Procedure in Congenital Heart Disease". Congenit Heart Dis. doi:10.1111/chd.12031. PMID 23280242. Unknown parameter
|month=ignored (help) - ↑ Granada, J.; Uribe, W.; Chyou, PH.; Maassen, K.; Vierkant, R.; Smith, PN.; Hayes, J.; Eaker, E.; Vidaillet, H. (2000). "Incidence and predictors of atrial flutter in the general population". J Am Coll Cardiol. 36 (7): 2242–6. PMID 11127467. Unknown parameter
|month=ignored (help) - ↑ "ACC/AHA/ESC Guidelines for the Management of Patients With Supraventricular Arrhythmias—Executive Summary". Retrieved 15 August 2013.
- ↑ 4.0 4.1 Fuster, V.; Rydén, LE.; Cannom, DS.; Crijns, HJ.; Curtis, AB.; Ellenbogen, KA.; Halperin, JL.; Kay, GN.; Le Huezey, JY. (2011). "2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines". Circulation. 123 (10): e269–367. doi:10.1161/CIR.0b013e318214876d. PMID 21382897. Unknown parameter
|month=ignored (help)