Atrial flutter electrocardiogram
|
Atrial flutter Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Atrial flutter electrocardiogram On the Web |
|
American Roentgen Ray Society Images of Atrial flutter electrocardiogram |
|
Risk calculators and risk factors for Atrial flutter electrocardiogram |
Please help WikiDoc by adding content here. It's easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Electrocardiographic Findings
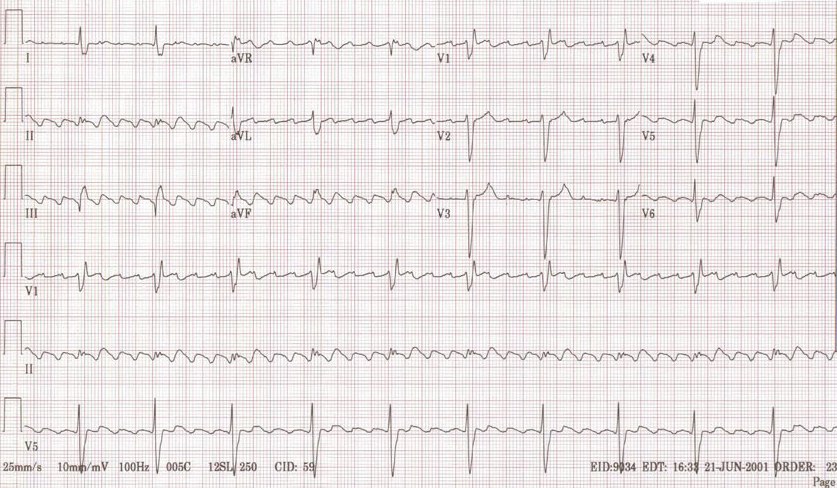
- There are rapid regular undulations (F waves) that cause a sawtooth appearance.
- Best seen in 2,3,F and V1.
- Usually inverted in the inferior leads.
- No isoelectric baselines between the F waves.
- Atrial rate is 250 to 350 Beats Per Minute (BPM).
- Can be faster in infants and children.
- Massive dilation of the atria can lead to a rate < 200 BPM.
- Quinidine can reduce the atrial rate.
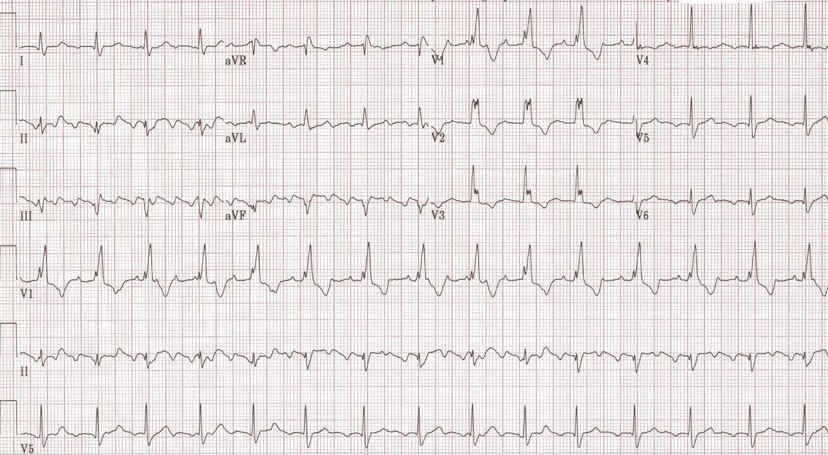
- There is a variable ventricular rate depending on the AV conduction.
- The Most common response is 2:1
- 3:1 is uncommon
- 4:1 suggests the existence of an AV conduction defect
- May be associated with complete AV block in which case the RR intervals are regular and the F waves have no constant relationship to the QRS. The ventricular response is usually slow.
- 1:1 conduction may be precipitated by excitement, exercise, induction of anesthesia or any increase in sympathetic tone. It may occur in WPW where the impulses are conducted antegrade through the bypass tract. All these are an emergency.
- During treatment with quinidine the atrial rate may slow sufficiently to permit 1:1 conduction.
- Vagal maneuvers increase the degree of AV block.
- QRS either normal or aberrant depending on preexisting IVCD or aberrant ventricular conduction.
Examples
-
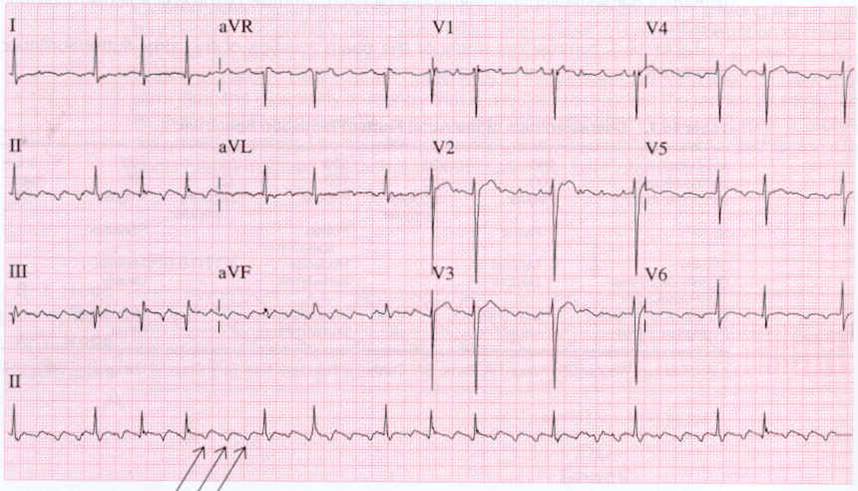
Atrial flutter
-
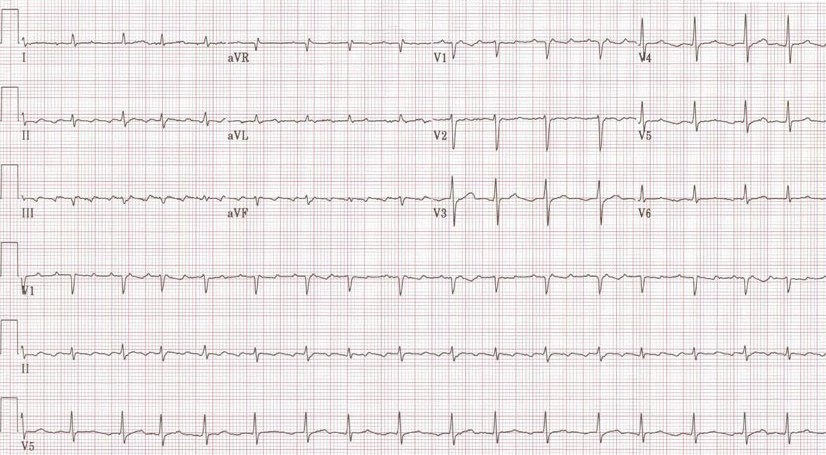
Atrial flutter with variable conduction
-
A very rare condition 1:1 Atrial flutter
-
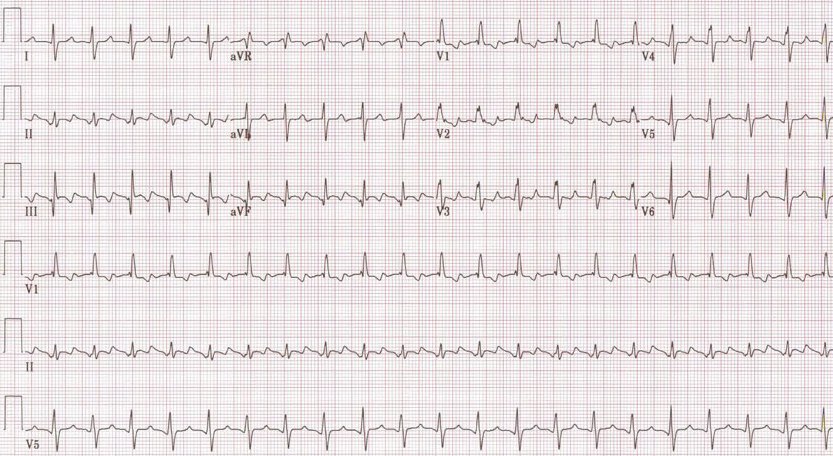
2:1 Atrial flutter
-
3:1 Atrial flutter
-
4:1 Atrial flutter
-
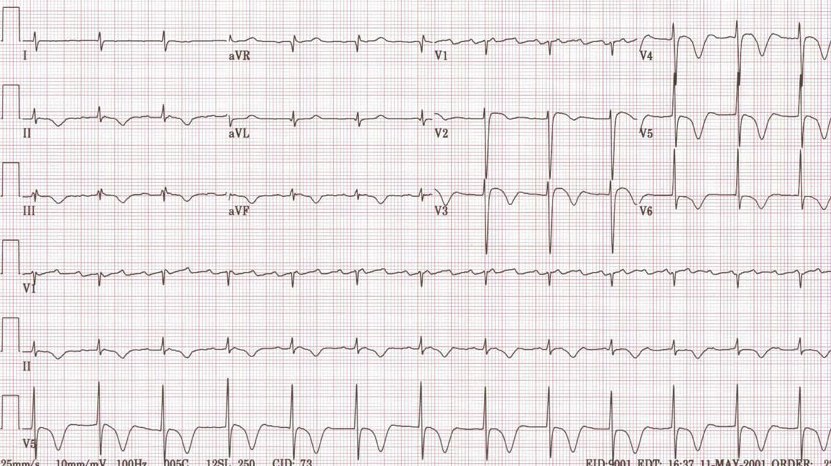
Atrial flutter with RBBB
-

Typical atrial flutter pattern







{kind=link}