Thymoma overview
|
Thymoma Microchapters |
|
Diagnosis |
|---|
|
Case Studies |
|
Thymoma overview On the Web |
|
American Roentgen Ray Society Images of Thymoma overview |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Amr Marawan, M.D. [2]
Overview
Thymoma is one of the organs contained in the anterior mediastinum, located behind the sternum in front of the great vessels that involutes during puberty, but continues to take part in lymphocytes maturation throughout adulthood. Thymic malignancies count for less than 0.13/100,000/year.
They can be divided into two major groups: thymoma and thymic carcinoma. Prognosis and proper management are essentially determined by pathologic classification. Surgery is the only curative treatment, but they can be sensitive to chemotherapy and radiotherapy especially in unresectable disease.
Thymoma is the most common tumor of the anterior mediastinum, consisting of any type of thymic epithelial cell as well as lymphocytes that are usually abundant and probably not neoplastic. Thymoma usually is benign, and frequently encapsulated uncommon tumor, best known for its association with the neuromuscular disorder myasthenia gravis. Thymoma is found in 15% of patients with myasthenia gravis. Once diagnosed, thymomas may be removed surgically. When occasionally malignant, then it is invasive: metastasis is extremely rare. In the rare case of a malignant tumor, chemotherapy may be used.
Malignant lymphomas that involve the thymus, e.g., lymphosarcoma, Hodgkin's disease (termed "granulomatous thymoma" in the past), should not be regarded as thymoma.[1]
Thymomas associated with autoimmune disorders usually are benign. Malignant thymomas can metastasize, generally to pleura, kidney, bone, liver or brain.[2]
Pathophysiology
In 1999, a WHO Working group suggested a non-committal terminology (Masaoka classification), preserving the distinct categories of the histogenetic classification, but using letters and numbers to designate tumour entities. Recently, it has been very well accepted as it provides an easy comparison of clinical, pathological and immunological studies
Epidemiology and Demographics
Thymic neoplasms are the most common tumors located in the anterior mediastinum (20%). Thymoma is a rare malignancy of unknown etiology that accounts for 0.2–1.5% of all malignancies. It's incidence in the U.S. population is 0.13 per 100,000 person-years.
Risk Factors
Most available evidence regarding risk factors for thymoma derives from descriptive epidemiologic studies of thymoma and associated malignancies. Unfortunately, no available data concerning the role of occupation, environmental exposures, or diet and nutrition.
Complications and Prognosis
The main prognostic factors for recurrence and survival are the stage at diagnosis and whether a complete resection has been achieved. Other prognostic factors with less impact on prognosis are the histological subtype, tumour size at diagnosis, age, gender and presence or absence of myasthenia gravis.
The natural history of thymoma certainly illustrates the tendency for local mediastinal recurrence and pleural ‘‘droplet’’ recurrence presumably caused by mediastinal pleural invasion after resection. Local recurrences have been noted in the surgical incision used to completely remove a thymoma.
Diagnosis
One-third of patients have their tumors discovered because they have an associated autoimmune disorder. The most common of those conditions is myasthenia gravis (MG); 10–15% of patients with MG have a thymoma and, conversely, 30–45% of patients with thymomas have MG. Historically, a classifiaction system used both histological features and clinical behavior. Masaoka staging is the clinically used staging system, although it may not be predictive for thymic carcinoma. GETT staging is the surgical staging system, and may have better correlation with outcome. Computed Tomography is the radiologic modality of choice to diagnose and evaluate thymoma.
Treatment
Surgery is the only curative treatment. Surgical biopsy should be avoided if a thymoma is highly suspecte based on clinical and radiological evaluation.The goal of surgery is complete resection of the tumor by total thymectomy and complete resection of the contiguous and noncontiguous disease. Chemo and radio therapy are used as adjuvant or neoadjuvant therapies. Sometimes they are used prior to surgery to make the tumor resectable. Signs and symptoms of myasthenia gravis should be evaluated before surgery and medically controlled.
-
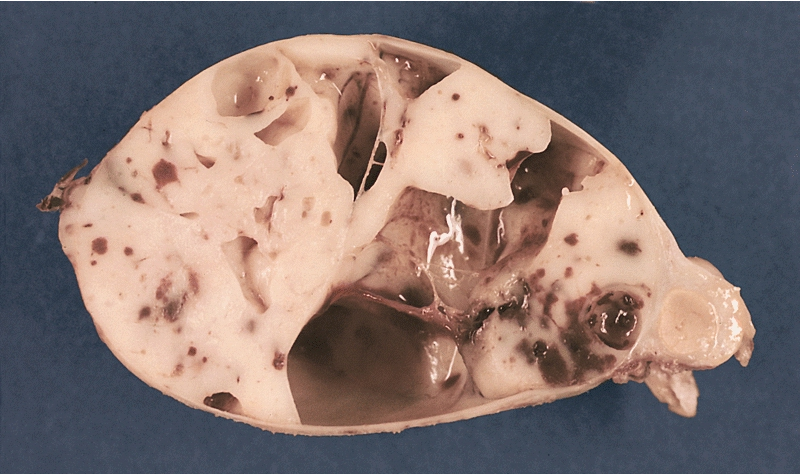
MEDIASTINUM: ENCAPSULATED CYSTIC THYMOMA. Post-formalin-fixed cut surface reveals an ivory-colored tumor with multiple cystic spaces varying from pin-head sized to a few centimeters in diameter. Small hemorrhages are also noted.

References
- ↑ Thomas CR, Wright CD, Loehrer PJ (1999). "Thymoma: state of the art". J. Clin. Oncol. 17 (7): 2280–9. PMID 10561285.
- ↑ Thomas CR, Wright CD, Loehrer PJ (1999). "Thymoma: state of the art". Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 17 (7): 2280–9. PMID 10561285. Retrieved 2012-01-18. Unknown parameter
|month=ignored (help)