Multiple myeloma overview
|
Multiple myeloma Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Multiple myeloma overview On the Web |
|
American Roentgen Ray Society Images of Multiple myeloma overview |
|
Risk calculators and risk factors for Multiple myeloma overview |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Haytham Allaham, M.D. [2] Associate Editor(s)-in-Chief: "sandbox:SN"
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [3]; Associate Editor(s)-in-Chief:
Overview
Pernicious anemia (also called Addison's anemia) is a type of red blood cell disorder caused by impaired vitamin B12 metabolism. Vitamin B12 is primarily absorbed by the small intestine, after being bound to intrinsic factor secreted by parietal cells of gastric mucosa. When this process is disrupted by conditions like atrophic gastritis, celiac disease, small bowel resection etc, B12 deficiency ensues.
Historical perspective
- Pernicious anemia was first discovered by Thomas Addison, hence it is also known as addison's anemia.
- Loss of life from large volume blood loss in the people fighting in the first world war inspired George Whipple to investigate blood forming components such as arsenic, iron pills etc, but found liver to be the most effective. He bled dogs until they had clinical anemia and fed them cooked liver which showed an improvement in symptoms and hematopoeisis. [1]
- In 1948, Smith, Rickles et al., isolated the anti-pernicious factor from liver extract and named it Vitamin B12. They showed that even small amounts of this factor can be used to treat and to prevent pernicious anemia. [2]
Pathophysiology
Vitamin B12 is an essential vitamin for humans and animals because we cannot synthesise it on our own. B12 is a cofactor in DNA synthesis and other important biochemical reactions. Vitamin B12 deficiency manifests as anemia because hematopoetic stem cells in the bone marrow which are rapidly dividing need B12 for division and DNA production. This process is impaired leading to ineffective hematopoeisis. Vitamin B12 is also necessary for production of myelin which is an important component in the covering sheath of nerves. Deficiency results in improper nerve conduction due to nerve destabilisation. [3]
Physiology
- Vitamin B12 is also called cobalamin because it contains cobalt at the core of its structure. Dietary sources of vitamin B12 include meat, fish and eggs.[4]
- When consumed through its dietary source, B12 is bound to protein till it enters the stomach.
- In the stomach, B12 is uncoupled from its carrier protein due to the presence of gastric acid, which is why vitamin B12 deficiency is so commonly seen among those on chronic antacid medication. [5]
- Once in the stomach, it is then bound to gastric R binder, a glycoprotein secreted by the salivary glands till it reaches the duodenum.[6]
- In the duodenum and jejunum, the pancreatic enzymes digest the gastric R binder and cobalamin is bound to intrinsic factor (IF).
- Intrinsic factor is secreted by the gastric parietal cells. Once bound to IF, vitamin B12 travels up to the ileum where IF is removed and B12 binds with carrier proteins called transcobalamins and this complex is taken up by the liver and bone marrow, among other tissues.
- Inside the cells, the transcobalamin-B12 complex is dissolved and cobalamin is reduced to methylcobalamin which serves as a cofactor and coenzyme in many important biochemical reactions[7].
The two major reactions involving B12 in the human body are:
- Vitamin B12 in the from of cyanocobalamin is required in the synthesis of methionine. Methionine is produced from homocysteine and is catalysed by the enzyme methionine synthase. This enzyme utilises cyanocobalamin as a cofactor. Deficiency of vitamin B12 causes a decreased production of methionine and buildup of homocysteine. Hyperhomocysteinemia is implicated as a risk factor in cardiovascular disease.[8]
- The Kreb's cycle utilises vitamin B12 in the reaction converting methylmalonyl-CoA to succinyl-CoA. Thus vitamin B12 deficiency causes a buildup of methylmalonic acid, the substrate for the enzyme methylmalonyl coenzyme A mutase. Methylmalonic acid levels are elevated in the urine of people affected with pernicious anemia and other forms of B12 deficiency.
Storage
The human body can store anywhere from 2-5mg of vitamin B12. Most of this is stored in the liver and is recycled via enterohepatic circulation.
Pathogenesis
Pernicious anemia is a type of megaloblastic anemia caused due to improper vitamin B12 absorption by the body. Impaired absorption occurs because of deficiency of intrinsic factor which is produced by the parietal cells of the stomach. The etiology of pernicious anemia can be due to autoimmune causes or genetic disease. In autoimmune disease, the antibodies attack most of the gastric mucosa, but the antrum is spared.
Autoimmune causes of pernicious anemia
This is the most common cause of pernicious anemia. In autoimmune pernicious anemia, the body produces antibodies against parietal cells or intrinsic factor.
- Antibodies against parietal cells of the gastric mucosa work to inhibit the H+/K(+)-ATPase which is the proton pump present in the parietal cells. The proton pump serves as an auto antigen and activates the cytotoxic CD4+ T cells which proceed to destroy gastric mucosal cells.[9][10]
- Intrinsic factor antibodies are present in fewer cases of pernicious anaemia but are highly specific. There are 2 types of IF antibodies. They prevent the binding and absorption of cobalamin in the ileum via its receptor.[11]
Clinical features
- The symptoms of pernicious anemia take months, and often years to manifest. Patients most commonly present with symptoms of anemia like lightheadedness, dizziness, shortness of breath etc. The population affected with pernicious anemia is usually the elderly (>60 years) owing to its insidious onset.
- Pernicious anemia has hematological, gastrointestinal and neurological manifestations.
- Hematological signs are the earliest manifestation of the disease while neurological signs are seen much later.
- Patients with pernicious anemia usually have very low levels of hydrochloric acid in the stomach (achlorhydria) and high levels on gastrin (hypergastrinemia).
Differentiating pernicious anemia from other diseases
Pernicious anemia shares many similarities with other forms of megaloblastic anemia like B12 and folate deficiency.
- Vitamin B12 deficiency due to insufficient intake (eg veganism) has all the features of pernicious anemia like megaloblasts, hypersegmented neutrophils, neuropsychiatric manifestations. But atrophic gastritis is absent, so achlorhydria, parietal cell antibodies or IF antibodies are absent. Intrinsic factor levels are also normal.[6]
- Folic acid deficiency also results in megaloblastic anemia and similar hematological changes as pernicious anemia, but urinary excretion of methylmalonic acid is absent, so are features of pernicious anemia like achlorhydria, antibodies and normal IF levels.
- Ileal resection causes B12 deficiency due to decreased absorption.
- Certain drugs such as methotrexate, azathioprine cause folate deficiency and result in megaloblastic anemia. This is usually seen in patients taking chemotherapy or other chronic conditions such as rheumatoid arthritis. [12]
- Chronic proton pump inhibitor therapy also results in B12 deficiency as vitamin B12 cannot dissociate from its carrier protein in the absence of an acidic environment.[13]
- Long term use of metformin, such as in diabetics, is linked to vitamin B12 deficiency and symptoms similar to pernicious anemia, but this can be differentiated from pernicious anemia as it is seen in diabetics on chronic therapy.[14]
Associated Conditions
People affected with pernicious anemia might have other coexisting autoimmune conditions such as autoimmune thyroiditis, autoimmune diabetes, vitiligo etc. Autoimmune thyroiditis is most commonly seen in patients with pernicious anemia, particularly females. HLA DR3 has been implicated in the development of autoimmune diseases such as pernicious anemia[15].
Epidemiology and demographics
- Pernicious anemia is a disease of the elderly. The mean age of patients who are symptomatic is >60.[16]
- An exception is the genetic form of the disease which is a congenital deficiency of intrinsic factor and is seen in children <10 years of age.
- Men and women are equally affected
- Prevalence of pernicious anemia is estimated at 0.1% of the population.[17]
Genetics
- Some forms of pernicious anemia are congenital and a genetic link has been postulated because of a higher incidence in certain populations.
- Affected people have a complete or near total absence of intrinsic factor and the presence of antibodies against intrinsic factor.
- The genetic variant is transmitted through an autosomal recessive pattern.[18]
Risk factors
- People who have autoimmune conditions like diabetes mellitus, autoimmune thyroiditis are at higher risk of developing pernicious anemia.
Natural History, Complications and Prognosis
- In most cases, patients affected with pernicious anemia remain asymptomatic for many years.
- Early manifestations include fatigue, shortness of breath, pallor and weakness.
- Long standing untreated pernicious anemia results in irreversible neurological damage such as subacute combined degeneration of the spinal cord.
- Neurological changes are irreversible once they set in and do not resolve with cobalamin supplementation.
Diagnosis
A diagnosis of pernicious anemia is made by a history and physical examination, along with hematological and neurological examination.
Diagnostic criteria
- The only specific criteria to diagnose pernicious anemia is an intrinsic factor output of less than 200U/h after pentagastrin stimulation, where normal levels would be >2000U/h. [19]
Symptoms
Symptoms of pernicious anemia are summarised below
| Hematological symptoms | Gastrointestinal symptoms | Neurological symptoms |
|---|---|---|
| Fatigue | Loss of appetite | Parasthesias |
| Weakness | Weight loss
|
Depression |
| Shortness of breath | Nausea | Gait problems |
| Dizziness | Burning sensation on tongue | Weakness |
| Tachycardia | Diarrhea | Loss of balance |
| Lightheadedness | Vomiting | Confusion |
Physical examination findings
Most important physical examination findings are the neurological findings of long standing B12 deficiency which leads to subacute combined degeneration of the spinal cord.
- Hematological signs include pallor and icterus.[20]
- Neurological signs: Vitamin B12 deficiency causes nerve demyelination. B12 deficiency also causes a buildup of methylmalonic acid which is toxic to neuronal cells and causes apoptosis.[21].
The main neurological manifestation of pernicious anemia and vitamin B12 deficiency is subacute combined degeneration. The posterior and lateral columns of the spinal cord are affected. Lateral column demyelination manifests as hyperreflexia and spasticity, while posterior column defects are loss of proprioception and vibration sense. Ataxia and loss of tandem gait are also manifestations of posterior column demyelination. Recreational or accidental inhalation of nitrous oxide gas (laughing gas) can precipitate subacute combined degeneration in people with low levels of vitamin B12.[22]
- Gastrointestinal signs: Upto 25% of people affected with pernicious anemia develop glossitis. The tongue appears red, "beefy" and smooth due to atrophy and blunting of the lingual papillae.[23]
Subacute combined degeneration

Laboratory findings
- The first step in diagnosis is a blood vitamin B12 level. Blood levels less than 200 pg/ml are seen in pernicious anemia.
- Intrinsic factor antibodies and Parietal cell antibodies.
- Low intrinsic factor level.[24]
- Gastric mucosal sampling shows parietal cell atrophy with antral sparing.[25]
- Increased level of gastrin.
- Increased levels of homocysteine and methylmalonyl-CoA.
- Decreased folate levels are seen due to "folate trapping" in the form of methyltetrahydrofolate.
Shilling Test
The Shilling test is no longer done to detect an IF deficiency but has historical importance. After a vitamin B12 deficiency is noted, the patient is given radioactively tagged cobalamin to take orally. Soon after this step, the patient is injected with unlabelled cobalamin intramuscularly. Urine is checked for radioactive cobalamin for the next 24 hours. In pernicious anemia, there is an intrinsic factor deficiency, therefore the orally consumed radioactive cobalamin will not be absorbed and can be detected in the urine. In the next step, the patient is given radioactive cobalamin along with intrinsic factor and their urine is checked for traces of radioactive cobalamin. Absence of radioactive cobalamin in the urine points to the deficiency of intrinsic factor in the patients stomach which is the cause of vitamin B12 deficiency[26]. If the cobalamin absorption does not increase even with intrinsic factor supplementation, patient can be given a course of antibiotics as bacterial overgrowth may hinder absorption.
Peripheral smear findings
- The most obvious peripheral smear finding is megaloblasts and macrocytes.
Megaloblastic anemia results due to the lagging behind of nuclear development when compared to cytoplasmic development. This is known as nuclear-cytoplasmic asynchrony. Such defective cells are destroyed in the bone marrow (intramedullary hemolysis).
- Decreased number of RBCs (erythopenia)
- Macrocytosis- the RBCs in pernicious anemia are very large. Macrocytosis is defined as cells that have an MCV >100 femtolitres (normal :80-100fL)
- Hypersegmented neutrophils : Neutrophils containing ≥ 6 lobes. [27]
- Poikilocytosis and anisocytosis
- Low reticulocyte count (reticulopenia)
- Howell-Jolly bodies
-
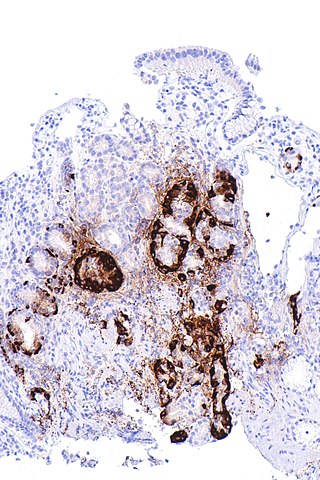
Atrophic gastritis
-
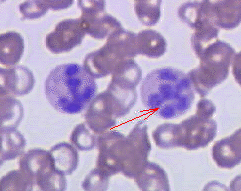
Hypersegmented neutrophil


Treatment
- Standard treatment for pernicious anemia is replacement of cobalamin via intramuscular injection. [28]
- 1000 mcg IM everyday for one week, followed by weekly injections the next month and then monthly once injections.
- Response to treatment is measured by an increase in reticulocyte count within 5 days of starting therapy.
- Patient also experience a sense of wellbeing shortly after beginning therapy.
- If reticulocytosis is not observed within the first week of therapy, other factors such as hypothyroidism, folate deficiency should be considered.
- Intramuscular therapy can be replaced by high dose oral therapy.[17]
- Neurological disease always warrants parenteral treatment.
- Within the first 3-4 weeks of treatment, marrow changes revert and there is resolution in macrocytosis.
- Most patients require lifelong monthly therapy.
- Routine follow up should be done with a CBC every few months.
- A small percentage of patients develop gastric carcinoma, particularly in the elderly. Regular surveillance helps in early detection and treatment. [29]
Prevention
- There is no primary preventive measure for pernicious anemia.
- Once sucessfully diagnosed and treated, patients with pernicious anemia are followed up every year for development of stomach cancer[30], or symptoms of anemia.
==References== Shyam Patel [4]
Overview
Multiple myeloma is a mature plasma cell neoplastic proliferative disease. Multiple myeloma is part of the broad group of diseases called hematological malignancies and is also known as plasma cell myeloma, myelomatosis, or Kahler disease.[31] Multiple myeloma can be caused by genetic mutations and chromosomal aberrations. Multiple myeloma must be differentiated from other plasma cell disorders, such as monoclonal gammopathy of undetermined significance(MGUS), isolated plasmacytoma of the bone, and extramedullary plasmacytoma. The prognosis of multiple myeloma is good with treatment, while without treatment, multiple myeloma will result in death with a median survival of 7 months.[32][33] Multiple myeloma is the second most common blood cancer after non-Hodgkin's lymphoma and the 14th most common cancer overall in United States.[34][35][36] There is insufficient evidence to recommend routine screening for multiple myeloma. If left untreated, most of patients with multiple myeloma may progress to develop fatigue, bone pain, and pallor. Laboratory findings consistent with the diagnosis of multiple myeloma include abnormal complete blood count, basic metabolic panel, electrophoresis and immunohistochemistry. While patients with smoldering (asymptomatic) multiple myeloma are managed by observation and undergoing follow up tests every 3 to 6 months, patients with active multiple myeloma usually require treatment to prevent progression of disease which can lead to death.
Historical Perspective
Multiple myeloma was first reported by Dr. Samuel Solly in the mid-19th century. The Bence Jones protein was first discovered by Dr. Henry Bence Jones around that time and was found to be associated with multiple myeloma. In the mid-20th century, chemotherapy was first used to treat multiple myeloma. Over the ensuing years, various agents were approved by the U.S. Food and Drug administration. In the late 20th century, it was shown that high-dose therapy and autologous stem cell transplantation could improve survival. The International Myeloma Working Group recently revised the criteria for a diagnosis of multiple myeloma in 2014 to better define the disease.
Classification
Multiple myeloma can be classified into several subtypes based on the extent of organ involvement (medullary or extramedullary) and the disease clinical presentation (active symptomatic or smoldering asymptomatic).[37] The four general categories include solitary plasmacytoma, monoclonal gammopathy of undetermined significance, smoldering multiple myeloma, and active multiple myeloma. Within the category of active multiple myeloma, the three risk groups include standard risk, intermediate risk, and high risk, based on the cytogenetic profile.
Pathophysiology
Multiple myeloma arises from post-germinal center plasma cells that are normally involved in production of human immunoglobulins.[38][36][39] Both sporadic events and familial contributions contribute to the pathogenesis of multiple myeloma. Renal involvement by multiple myeloma is catergorized into three entities: light chain cast nephropathy, monoclonal immunoglobulin deposition disease, and amyloidosis. Osseous involvement by multiple myeloma is based on cytokine and cellular interactions that lead to bone breakdown. On microscopic histopathological analysis, abundant eosinophilic cytoplasm, eccentrically placed nucleus, and Russell bodies are characteristic findings of multiple myeloma.[40]
Causes
The causes of multiple myeloma include sporadic mutations and genetic predisposition. Mutations in tumor suppressors or oncogenes can cause multiple myeloma. Mutations in the tumor suppressor TP53 is most common. Chromosomal aberrations such as translocations can trigger the onset of malignancy and allow for uncontrolled plasma cell proliferation.[41] Familial causes are less contributory to the development of multiple myeloma compared to sporadic causes.[41]
Differentiating Multiple Myeloma from other Diseases
Multiple myeloma must be differentiated from osteoporosis, osteomalacia, scurvy, osteogenesis imperfecta, and homocystinuria. Each condition has unique causes, features, and treatments.
Epidemiology and Demographics
In 2012, the incidence of multiple myeloma was approximately 6.3 per 100,000 cases with a mortality rate of 3.3 per 100,000 cases in the United States.[42] The prevalence of multiple myeloma was estimated to be 89,658 cases in 2012 in the United States.[35][36] Multiple myeloma is the second most common blood cancer after non-Hodgkin's lymphoma and 14th most common cancer overall in United States.[34][35][36] Males are more commonly affected with multiple myeloma than females; the male to female ratio is approximately 1.54 to 1.[36][38] Multiple myeloma usually affects individuals of the African American race. Asian individuals are less likely to develop multiple myeloma.[36] The incidence of multiple myeloma increases with age.
Risk Factors
Risk factors for multiple myeloma include advanced age, African American race, male gender, obesity, exposure to chemicals and radiation, presence of family history of hematologic conditions.
Screening
There is insufficient evidence to recommend routine screening for multiple myeloma in the general population.[43][44] However, laboratory assessment should be done often (typically once per year or more frequently) for patients who have monoclonal gammopathy of undetermined significance and smoldering multiple myeloma.
Natural History, Complications and Prognosis
The natural history of multiple myeloma begins with an asymptomatic phase, then progresses to symptomatic involvement and organ involvement. Outcomes are generally good if treatment is begun at an appropriate time. Complications of multiple myeloma include hematologic complications, such as cytopenias, and skeletal complications, such as pathologic fractures. The prognosis of multiple myeloma is based on chromosome changes, stage of disease, kidney function, labelling index, age, performance status, and various laboratory values.
Diagnosis
Diagnostic Criteria
The diagnosis of monoclonal gammopathy of undetermined significance requires the presence of clonal plasma cells < 10% and serum monoclonal protein <3g/dl but the absence of end-organ damage. The diagnosis of smoldering multiple myeloma requires the presence of clonal plasma cells 10%-60% and serum monoclonal protein >3g/dl but the absence of end-organ damage. The diagnosis of active multiple myeloma requires the presence of end-organ damage. In November 2014, the International Myeloma Working Group (IMWG) updated the criteria for the diagnosis of multiple myeloma to include novel validated biomarkers to better encompass the extent of disease. Prior to 2014, the original diagnostic criteria for end-organ damage included CRAB features (hypercalcemia, renal failure, anemia, and bone lesions) without consideration of the plasma cell burden or free light chain ratio. The 2014 update also clarified the underlying laboratory and radiographic findings of CRAB features, as well as the histological and monoclonal protein requirements for the disease diagnosis.[45]
Staging
Multiple myeloma may be divided into three stages based on either the International Staging System (ISS) or Durie-Salmon Staging System.[46] The International Staging System for multiple myeloma was published by the International Myeloma Working Group in 2003 and is the most widely used staging system.[46][47] It is used for both guiding treatment as well as predicting prognosis. The Durie-Salmon staging system, first published in 1975, is a clinical staging system for multiple myeloma that correlates measured myeloma cell mass to the presenting clinical features, response to treatment, and survival.[48] Durie-Salmon Staging System is still in use, but has been largely superseded by the more practical ISS and revised ISS [46]
History and Symptoms
The history and symptoms of multiple myeloma are based on the underlying effect of excess plasma cells on various organ systems. Pain is usually a symptom of newly diagnosed multiple myeloma. Broad categories of symptoms include bone-related symptoms, neurological symptoms, hypercalcemia-related symptoms, bone marrow failure-related symptoms, and thrombotic-related symptoms. Although all of these symptoms are possible, the presentation of multiple myeloma varies from patient to patient.
Physical Examination
Patients with multiple myeloma usually appear fatigued and lethargic. Physical examination of patients with multiple myeloma is usually remarkable for pallor, purpura, hepatosplenomegaly, bony tenderness, carpal tunnel syndrome, and signs of cord compression. Any of these physical findings may warrant further evaluation, and thus lead to an incidental diagnosis of multiple myeloma.[49][50]
Laboratory Findings
Laboratory findings consistent with the diagnosis of multiple myeloma include abnormal complete blood count, abnormal basic metabolic panel, elevated monoclonal protein on serum electrophoresis, elevated serum free light chains, and presence of myeloma-specific protein markers by immunohistochemistry or immunophenotyping. Some of the laboratory tests are factors that determine the stage of multiple myeloma.
Electrocardiography
There are two indications for obtaining an electrocardiogram in the workup and management of multiple myeloma: carfilzomib use and evaluation of cardiac amyloidosis. In both of these situations, a baseline electrocardiogram may be useful. Subsequent electrocardiograms may be useful for monitoring. Electrocardiogram abnormalities include atrioventricular block and low voltage QRS complexes.
X Ray
X-ray may be helpful in the diagnosis of multiple myeloma. Findings on X-ray suggestive of multiple myeloma include punched out bony lesions, generalized osteopenia, and hair-on-end appearance.[38][51] In some cases, MRI may be needed if X-ray is insufficient for diagnosis.
CT
CT scan does not have a major role in the diagnosis of disseminated multiple myeloma.[52] but low-dose whole-body CT may be helpful.[53][51] CT may also be useful for diagnosis of thrombotic-related complications and bony destruction from multiple myeloma. CT carries a high risk for radiation and should not be performed in pregnant patients.
MRI
MRI may be diagnostic of multiple myeloma.[53]Findings on MRI suggestive of multiple myeloma include infiltration and replacement of the bone marrow.[38][51] MRI is a more expensive test than an X-ray.
Other Imaging Findings
Positron emission tomography (PET) scan may be diagnostic of multiple myeloma.[50][44][54][55][53]Findings on PET scan suggestive of multiple myeloma include uptake of the F18-FDG molecule by lesions of bone lysis seen on PET-CT scan.[44][53]
Other Diagnostic Studies
Bone marrow biopsy is an important diagnostic test in multiple myeloma. Bone marrow biopsy consists of the collection of the bone marrow aspirate and the solid core biopsy. Tests that can be performed on the bone marrow biopsy include karyotyping (chromosomal analysis) and immunophenotyping.
Treatment
Medical Therapy
First-line therapies include bortezomib, lenalidomide, dexamethasone, melphalan, and cyclophosphamide. Second-line therapies (used for relapsed or refractory disease) include ixazomib, carfilzomib, daratumumab, elotuzumab, and pomalidomide. Autologous stem cell transplant is done after remission is achieved with chemotherapy. The choice of the treatment regimen partly depends on transplant eligibility. Supportive therapy is an important component of care while patients are receiving anti-cancer therapy.
Surgery
Surgery places a role for specific conditions that occur in patients with multiple myeloma. Surgical removal of plasmacytoma is frequently done in an attempt to achieve cure. Surgery can be done for bone stabilization in patients who have osseous breakdown. Benefits of surgical intervention include pain relief, restoration of functional disability, and alleviation of neurologic deficits. Risks of surgery include neurologic compromise (for vertebral spine surgeries), bleeding, infection, and inherent surgical risk.
Future or Investigational Therapies
Chimeric antigen receptor T (CAR-T) cell therapy is actively under study for the treatment of relapsed and refractory multiple myeloma. This form of cell-based therapy employs one's own T lymphocytes, which are engineered to be tumor-specific. The antigen of interest for multiple myeloma CAR-T therapy is B cell maturation antigen (BCMA). Other investigational therapies include lymphoma-like polychemotherapy regimen and Bruton's tyrosine kinase inhibitor CC-292.
References
- ↑ Sinclair L (2008). "Recognizing, treating and understanding pernicious anaemia". J R Soc Med. 101 (5): 262–4. doi:10.1258/jrsm.2008.081006. PMC 2376267. PMID 18463283.
- ↑ SMITH EL (1948). "Purification of anti-pernicious anaemia factors from liver". Nature. 161 (4095): 638. doi:10.1038/161638a0. PMID 18856623.
- ↑ Miles LM, Allen E, Clarke R, Mills K, Uauy R, Dangour AD (2017). "Impact of baseline vitamin B12 status on the effect of vitamin B12 supplementation on neurologic function in older people: secondary analysis of data from the OPEN randomised controlled trial". Eur J Clin Nutr. 71 (10): 1166–1172. doi:10.1038/ejcn.2017.7. PMID 28225050.
- ↑ Watanabe F (2007). "Vitamin B12 sources and bioavailability". Exp Biol Med (Maywood). 232 (10): 1266–74. doi:10.3181/0703-MR-67. PMID 17959839.
- ↑ Jung SB, Nagaraja V, Kapur A, Eslick GD (2015). "Association between vitamin B12 deficiency and long-term use of acid-lowering agents: a systematic review and meta-analysis". Intern Med J. 45 (4): 409–16. doi:10.1111/imj.12697. PMID 25583062.
- ↑ 6.0 6.1 Del Corral A, Carmel R (1990). "Transfer of cobalamin from the cobalamin-binding protein of egg yolk to R binder of human saliva and gastric juice". Gastroenterology. 98 (6): 1460–6. doi:10.1016/0016-5085(90)91076-i. PMID 2110915.
- ↑ Harrington DJ (2017). "Laboratory assessment of vitamin B12 status". J Clin Pathol. 70 (2): 168–173. doi:10.1136/jclinpath-2015-203502. PMID 27169753.
- ↑ Tinelli C, Di Pino A, Ficulle E, Marcelli S, Feligioni M (2019). "Hyperhomocysteinemia as a Risk Factor and Potential Nutraceutical Target for Certain Pathologies". Front Nutr. 6: 49. doi:10.3389/fnut.2019.00049. PMC 6491750. PMID 31069230.
- ↑ Callaghan JM, Khan MA, Alderuccio F, van Driel IR, Gleeson PA, Toh BH (1993). "Alpha and beta subunits of the gastric H+/K(+)-ATPase are concordantly targeted by parietal cell autoantibodies associated with autoimmune gastritis". Autoimmunity. 16 (4): 289–95. doi:10.3109/08916939309014648. PMID 7517707.
- ↑ Toh BH, Sentry JW, Alderuccio F (2000). "The causative H+/K+ ATPase antigen in the pathogenesis of autoimmune gastritis". Immunol Today. 21 (7): 348–54. doi:10.1016/s0167-5699(00)01653-4. PMID 10871877.
- ↑ Schade SG, Abels J, Schilling RF (1967). "Studies on antibody to intrinsic factor". J Clin Invest. 46 (4): 615–20. doi:10.1172/JCI105563. PMC 442045. PMID 6021209.
- ↑ Green R, Datta Mitra A (2017). "Megaloblastic Anemias: Nutritional and Other Causes". Med Clin North Am. 101 (2): 297–317. doi:10.1016/j.mcna.2016.09.013. PMID 28189172.
- ↑ Heidelbaugh JJ (2013). "Proton pump inhibitors and risk of vitamin and mineral deficiency: evidence and clinical implications". Ther Adv Drug Saf. 4 (3): 125–33. doi:10.1177/2042098613482484. PMC 4110863. PMID 25083257.
- ↑ Aroda VR, Edelstein SL, Goldberg RB, Knowler WC, Marcovina SM, Orchard TJ; et al. (2016). "Long-term Metformin Use and Vitamin B12 Deficiency in the Diabetes Prevention Program Outcomes Study". J Clin Endocrinol Metab. 101 (4): 1754–61. doi:10.1210/jc.2015-3754. PMC 4880159. PMID 26900641.
- ↑ Zulfiqar AA, Andres E (2017). "Association pernicious anemia and autoimmune polyendocrinopathy: a retrospective study". J Med Life. 10 (4): 250–253. PMC 5771255. PMID 29362601.
- ↑ Carmel R (1996). "Prevalence of undiagnosed pernicious anemia in the elderly". Arch Intern Med. 156 (10): 1097–100. PMID 8638997.
- ↑ 17.0 17.1 Andres E, Serraj K (2012). "Optimal management of pernicious anemia". J Blood Med. 3: 97–103. doi:10.2147/JBM.S25620. PMC 3441227. PMID 23028239.
- ↑ Gordon MM, Brada N, Remacha A, Badell I, del Río E, Baiget M; et al. (2004). "A genetic polymorphism in the coding region of the gastric intrinsic factor gene (GIF) is associated with congenital intrinsic factor deficiency". Hum Mutat. 23 (1): 85–91. doi:10.1002/humu.10297. PMID 14695536.
- ↑ Cattan D (2011). "Pernicious anemia: what are the actual diagnosis criteria?". World J Gastroenterol. 17 (4): 543–4. doi:10.3748/wjg.v17.i4.543. PMC 3027024. PMID 21274387.
- ↑ Seynabou F, Fatou Samba Diago N, Oulimata Diop D, Abibatou Fall S, Nafissatou D (2016). "Biermer anemia: Hematologic characteristics of 66 patients in a Clinical Hematology Unit at Senegal". Med Sante Trop. 26 (4): 402–407. doi:10.1684/mst.2016.0625. PMID 28073728.
- ↑ Han L, Wu S, Han F, Gu X (2015). "Insights into the molecular mechanisms of methylmalonic acidemia using microarray technology". Int J Clin Exp Med. 8 (6): 8866–79. PMC 4538064. PMID https://www.ncbi.nlm.nih.gov/pubmed/26309541 Check
|pmid=value (help). - ↑ Choi C, Kim T, Park KD, Lim OK, Lee JK (2019). "Subacute Combined Degeneration Caused by Nitrous Oxide Intoxication: A Report of Two Cases". Ann Rehabil Med. 43 (4): 530–534. doi:10.5535/arm.2019.43.4.530. PMC 6734019 Check
|pmc=value (help). PMID 31499607. - ↑ Stoopler ET, Kuperstein AS (2013). "Glossitis secondary to vitamin B12 deficiency anemia". CMAJ. 185 (12): E582. doi:10.1503/cmaj.120970. PMC 3761039. PMID 23359038.
- ↑ Lahner E, Annibale B (2009). "Pernicious anemia: new insights from a gastroenterological point of view". World J Gastroenterol. 15 (41): 5121–8. doi:10.3748/wjg.15.5121. PMC 2773890. PMID 19891010.
- ↑ Korman MG, Strickland RG, Hansky J (1972). "The functional 'G' cell mass in atrophic gastritis". Gut. 13 (5): 349–51. doi:10.1136/gut.13.5.349. PMC 1412218. PMID 5036089.
- ↑ "StatPearls". 2020. PMID 29939561.
- ↑ Farrelly SJ, O'Connor KA (2017). "Hypersegmented neutrophils and oval macrocytes in the setting of B12 deficiency and pancytopaenia". BMJ Case Rep. 2017. doi:10.1136/bcr-2016-218508. PMC 5612428. PMID 28821482.
- ↑ Annibale B, Lahner E, Fave GD (2011). "Diagnosis and management of pernicious anemia". Curr Gastroenterol Rep. 13 (6): 518–24. doi:10.1007/s11894-011-0225-5. PMID 21947876.
- ↑ Murphy G, Dawsey SM, Engels EA, Ricker W, Parsons R, Etemadi A; et al. (2015). "Cancer Risk After Pernicious Anemia in the US Elderly Population". Clin Gastroenterol Hepatol. 13 (13): 2282-9.e1-4. doi:10.1016/j.cgh.2015.05.040. PMC 4655146. PMID 26079040.
- ↑ Venerito M, Link A, Rokkas T, Malfertheiner P (2016). "Gastric cancer - clinical and epidemiological aspects". Helicobacter. 21 Suppl 1: 39–44. doi:10.1111/hel.12339. PMID 27531538.
- ↑ Sergentanis TN, Zagouri F, Tsilimidos G, Tsagianni A, Tseliou M, Dimopoulos MA, Psaltopoulou T (October 2015). "Risk Factors for Multiple Myeloma: A Systematic Review of Meta-Analyses". Clin Lymphoma Myeloma Leuk. 15 (10): 563–77.e1–3. doi:10.1016/j.clml.2015.06.003. PMID 26294217.
- ↑ Multiple myeloma. National Cancer Institute(2015) www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#link/_40_toc Accessed on September, 20th 2015
- ↑ Multiple myeloma. Librepathology (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_pathophysiology&action=edit§ion Accessed on September, 20th 2015=1
- ↑ 34.0 34.1 Collins, CD. (2005). "Problems monitoring response in multiple myeloma". Cancer Imaging. 5 Spec No A: S119–26. doi:10.1102/1470-7330.2005.0033. PMID 16361127.
- ↑ 35.0 35.1 35.2 Seer stat fact sheet. National cancer institute (2015)http://seer.cancer.gov/statfacts/html/mulmy.html Accessed on September, 20th 2015
- ↑ 36.0 36.1 36.2 36.3 36.4 36.5 Multiple myeloma. Wikipedia (2015)https://en.wikipedia.org/wiki/Multiple_myeloma#Pathophysiology Accessed on September, 20th 2015
- ↑ Alexiou C, Kau RJ, Dietzfelbinger H, Kremer M, Spiess JC, Schratzenstaller B; et al. (1999). "Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts". Cancer. 85 (11): 2305–14. PMID 10357398.
- ↑ 38.0 38.1 38.2 38.3 Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
- ↑ Multiple myeloma. Medlineplus (2015)https://www.nlm.nih.gov/medlineplus/multiplemyeloma.html Accessed on September, 20th 2015
- ↑ Multiple myeloma. Librepathology (2015)http://www.wikidoc.org/index.php?title=Multiple_myeloma_pathophysiology&action=edit§ion=1 Accessed on September, 20th 2015
- ↑ 41.0 41.1 Rajkumar SV (2016). "Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management". Am J Hematol. 91 (7): 719–34. doi:10.1002/ajh.24402. PMC 5291298. PMID 27291302.
- ↑ Plasma cell neoplasm.National cancer institute (2015)http://www.cancer.gov/types/myeloma/hp/myeloma-treatment-pdq#cit/section_1.1 Accessed on September, 20th 2015
- ↑ Multiple Myeloma Prevention and Screening.(2015)http://www.mdanderson.org/patient-and-cancer-information/cancer-information/cancer-types/multiple-myeloma/prevention/index.html
- ↑ 44.0 44.1 44.2 Can multiple myeloma be prevented?(2015)http://www.cancer.org/cancer/multiplemyeloma/detailedguide/multiple-myeloma-prevention
- ↑ Rajkumar, S. Vincent, Meletios A. Dimopoulos, Antonio Palumbo, Joan Blade, Giampaolo Merlini, María-Victoria Mateos, Shaji Kumar et al. "International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma." The Lancet Oncology 15, no. 12 (2014): e538-e548
- ↑ 46.0 46.1 46.2 About multiple myeloma. University of California San Francisco (2015)http://cancer.ucsf.edu/research/multiple-myeloma/ Accessed on September, 18 2015
- ↑ Greipp PR, San Miguel J, Fonseca R, Avet-Loiseau H, Jacobson JL, Rasmussen E, Crowley J, Durie BMG. Development of an international prognostic index (IPI) for myeloma: report of the international myeloma working group. Hematology Journal 2003;4:S42. NLM ID 100965523.
- ↑ Durie BG, Salmon SE (1975). "A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival". Cancer. 36 (3): 842–54. PMID 1182674.
- ↑ Multiple myeloma. Wikipedia (2015) https://en.wikipedia.org/wiki/Multiple_myeloma#Signs_and_symptoms Accessed on September, 20th 2015
- ↑ 50.0 50.1 Multiple myeloma. Canadian Cancer Society (2015) http://www.cancer.ca/en/cancer-information/cancer-type/multiple-myeloma/signs-and-symptoms/?region=mb Accessed on September 20th 2015
- ↑ 51.0 51.1 51.2 Reisenbuckler C (2014). "Multiple myeloma and diagnostic imaging". Radiol Technol. 85 (4): 391–410, quiz 411–3. PMID 24614435.
- ↑ Multiple myeloma. Radiopaedia (2015)http://radiopaedia.org/articles/multiple-myeloma-1 Accessed on September, 20th 2015
- ↑ 53.0 53.1 53.2 53.3 Gerecke C, Fuhrmann S, Strifler S, Schmidt-Hieber M, Einsele H, Knop S (July 2016). "The Diagnosis and Treatment of Multiple Myeloma". Dtsch Arztebl Int. 113 (27–28): 470–6. doi:10.3238/arztebl.2016.0470. PMC 4973001. PMID 27476706.
- ↑ Shortt CP, Gleeson TG, Breen KA, McHugh J, O'Connell MJ, O'Gorman PJ; et al. (2009). "Whole-Body MRI versus PET in assessment of multiple myeloma disease activity". AJR Am J Roentgenol. 192 (4): 980–6. doi:10.2214/AJR.08.1633. PMID 19304704.
- ↑ Agarwal A, Chirindel A, Shah BA, Subramaniam RM (2013). "Evolving role of FDG PET/CT in multiple myeloma imaging and management". AJR Am J Roentgenol. 200 (4): 884–90. doi:10.2214/AJR.12.9653. PMID 23521465.