Sleep apnea polysomnography
|
Sleep Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Sleep apnea polysomnography On the Web |
|
American Roentgen Ray Society Images of Sleep apnea polysomnography |
|
Risk calculators and risk factors for Sleep apnea polysomnography |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Kashish Goel, M.D.
Overview
Polysomnography
Results of polysomnography in obstructive sleep apnea show pauses in breathing. As in central apnea, pauses are followed by a relative decrease in blood oxygen and an increase in the blood carbon dioxide. Whereas in central sleep apnea the body's motions of breathing stop, in obstructive sleep apnea the chest not only continues to make the movements of inhalation, the movements typically become even more pronounced. Monitors for airflow at the nose and mouth show the dynamics of airflow, but efforts to breathe are not only present, they are often exaggerated. The chest muscles and diaphragm contract and the entire body may thrash and struggle.
-
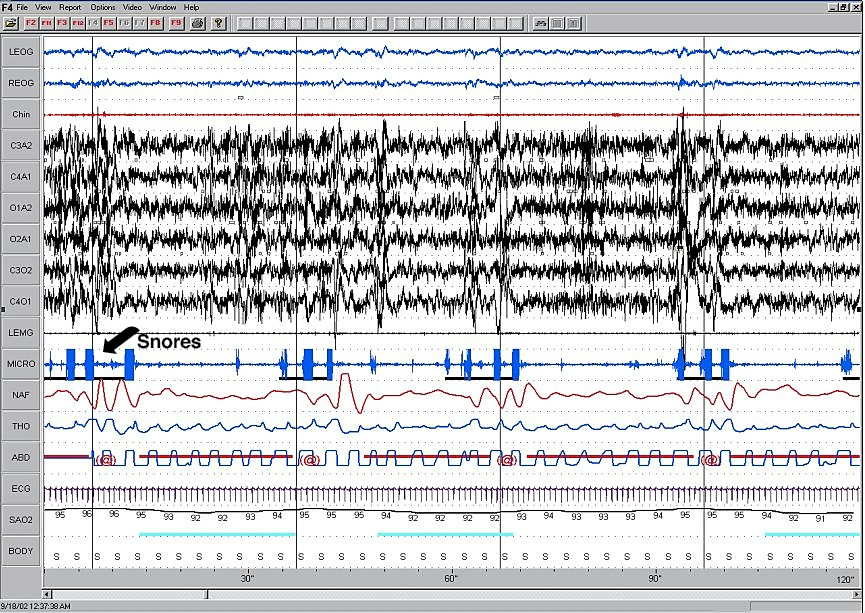
Two minute epoch representing continuous OSA. (Click on this image for larger version)

Obstructive sleep apnea is the most common category of sleep-disordered breathing. The prevalence of OSA among the adult population in western Europe and North America has not been confidently established, but in the mid-1990s was estimated to be 3-4% of women and 6-7% of men.
An "event" can be either an apnea, characterised by complete cessation of airflow for at least 10 seconds, or a hypopnea in which airflow decreases by 50 percent for 10 seconds or decreases by 30 percent if there is an associated decrease in the oxygen saturation or an arousal from sleep (American Academy of Sleep Medicine Task Force, 1999). To grade the severity of sleep apnea the number of events per hour is reported as the apnea-hypopnea index (AHI). An AHI of less than 5 is considered normal. An AHI of 5-15 is mild; 15-30 is moderate and more than 30 events per hour characterizes severe sleep apnea.