Pancreatic neuroendocrine tumor: Difference between revisions
Shanshan Cen (talk | contribs) |
Shanshan Cen (talk | contribs) No edit summary |
||
| Line 42: | Line 42: | ||
==Diagnosis== | ==Diagnosis== | ||
[[Pancreatic neuroendocrine tumor | [[Pancreatic neuroendocrine tumor staging| Staging]] | [[Pancreatic neuroendocrine tumor history and symptoms| History and Symptoms]] | [[Pancreatic neuroendocrine tumor physical examination | Physical Examination]] | [[Pancreatic neuroendocrine tumor laboratory findings|Laboratory Findings]] | [[Pancreatic neuroendocrine tumor other imaging findings|Other Imaging Findings]] | [[Pancreatic neuroendocrine tumor other diagnostic studies|Other Diagnostic Studies]] | ||
==Treatment== | ==Treatment== | ||
Revision as of 19:02, 17 August 2015
| Pancreatic neuroendocrine tumor | |
| Classification and external resources | |

| |
|---|---|
| ICD-10 | C25.4 |
| eMedicine | med/ |
|
Pancreatic neuroendocrine tumor Microchapters |
|
Differentiating Pancreatic neuroendocrine tumor from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Pancreatic neuroendocrine tumor On the Web |
|
American Roentgen Ray Society Images of Pancreatic neuroendocrine tumor |
|
Directions to Hospitals Treating Pancreatic neuroendocrine tumor |
|
Risk calculators and risk factors for Pancreatic neuroendocrine tumor |
For patient information on this page, click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]
Synonyms and keywords: Islet-cell carcinoma
Overview
Historical Perspective
Classification
Pathophysiology
Causes
Differentiating Pancreatic neuroendocrine tumor from other Diseases
Epidemiology and Demographics
Risk Factors
Natural History, Complications and Prognosis
Diagnosis
Staging | History and Symptoms | Physical Examination | Laboratory Findings | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Surgery | Primary Prevention | Secondary Prevention | Future or Investigational Therapies
Case Studies
|
Pancreatic neuroendocrine tumor Microchapters |
|
Differentiating Pancreatic neuroendocrine tumor from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Pancreatic neuroendocrine tumor On the Web |
|
American Roentgen Ray Society Images of Pancreatic neuroendocrine tumor |
|
Directions to Hospitals Treating Pancreatic neuroendocrine tumor |
|
Risk calculators and risk factors for Pancreatic neuroendocrine tumor |
Please help WikiDoc by adding content here. It's easy! Click here to learn about editing.
References
Staging
The 2010 WHO classification of tumors of the digestive system grades all the neuroendocrine tumors into three categories, based on their degree of cellular differentiation (from well-differentiated "NET G1" through to poorly-differentiated "NET G3"). The NCCN recommends use of the same AJCC-UICC staging system as pancreatic adenocarcinoma. Using this scheme, the stage by stage outcomes for PanNETs are dissimilar to pancreatic exocrine cancers.[1] A different TNM system for PanNETs has been proposed by The European Neuroendocrine Tumor Society.
- Pancreatic neuroendocrine tumor staging (AJCC)
-
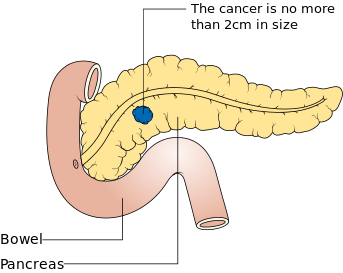
Stage T1
-
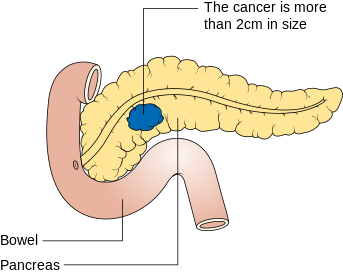
Stage T2
-
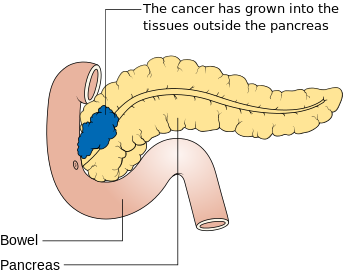
Stage T3
-
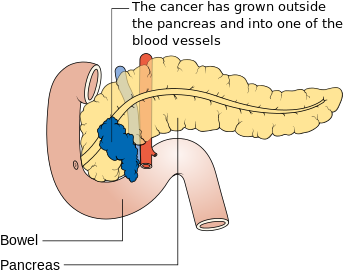
Stage T4
-
Involvement of nearby lymph nodes – Stage N1
-
Metastasis – stage M1





Treatment
In general, treatment for PanNET encompasses the same array of options as other neuroendocrine tumors, as discussed in that main article. However, there are some specific differences, which are discussed here.
In functioning PanNETs, octreotide is usually recommended prior to biopsy or surgery but is generally avoided in insulinomas to avoid profound hypoglycemia.
PanNETs in MEN1 are often multiple, and thus require different treatment and surveillance strategies.
Some PanNETs are more responsive to chemotherapy than are gastroenteric carcinoid tumors. Several agents have shown activity. In well differentiated PanNETs, chemotherapy is generally reserved for when there are no other treatment options. Combinations of several medicines have been used, such as doxorubicin with streptozocin and fluorouracil (5-FU) and capecitabine with temozolomide. Although marginally effective in well-differentiated PETs, cisplatin with etoposide has some activity in poorly differentiated neuroendocrine cancers (PDNECs), particularly if the PDNEC has an extremely high Ki-67 score of over 50%.
Several targeted therapy agents have been approved in PanNETs by the FDA based on improved progression-free survival (PFS):
- everolimus (Afinitor) is labeled for treatment of progressive neuroendocrine tumors of pancreatic origin in patients with unresectable, locally advanced or metastatic disease. The safety and effectiveness of everolimus in carcinoid tumors have not been established.
- sunitinib (Sutent) is labeled for treatment of progressive, well-differentiated pancreatic neuroendocrine tumors in patients with unresectable locally advanced or metastatic disease. Sutent also has approval from the European Commission for the treatment of 'unresectable or metastatic, well-differentiated pancreatic neuroendocrine tumors with disease progression in adults'. A phase III study of sunitinib treatment in well differentiated pNET that had worsened within the past 12 months (either advanced or metastatic disease) showed that sunitinib treatment improved progression-free survival (11.4 months vs. 5.5 months), overall survival, and the objective response rate (9.3% vs. 0.0%) when compared with placebo.
Genetics
DNA mutation analysis in well-differentiated pancreatic neuroendocrine tumors identified four important findings:[2][3]
- as expected, the genes mutated in NETs, MEN1, ATRX, DAXX, TSC2, PTEN and PIK3CA,[2] are different from the mutated genes previously found in pancreatic adenocarcinoma.[4][5]
- one in six well-differentiated pancreatic NETs have mutations in mTOR pathway genes, such as TSC2, PTEN and PIK3CA.[2] The sequencing discovery might allow selection of which NETs would benefit from mTOR inhibition such as with everolimus, but this awaits validation in a clinical trial.
- mutations affecting a new cancer pathway involving ATRX and DAXX genes were found in about 40% of pancreatic NETs.[2] The proteins encoded by ATRX and DAXX participate in chromatin remodeling of telomeres; these mutations are associated with a telomerase-independent maintenance mechanism termed ALT (alternative lengthening of telomeres) that results in abnormally long telomeric ends of chromosomes.
References
- ↑ National Cancer Institute. Pancreatic Neuroendocrine Tumors (Islet Cell Tumors) Treatment (PDQ®) Incidence and Mortality [1]
- ↑ 2.0 2.1 2.2 2.3 2.4 Jiao, Y.; Shi, C.; Edil, B. H.; De Wilde, R. F.; Klimstra, D. S.; Maitra, A.; Schulick, R. D.; Tang, L. H.; Wolfgang, C. L.; Choti, M. A.; Velculescu, V. E.; Diaz Jr, L. A.; Vogelstein, B.; Kinzler, K. W.; Hruban, R. H.; Papadopoulos, N. (2011). "DAXX/ATRX, MEN1, and mTOR Pathway Genes Are Frequently Altered in Pancreatic Neuroendocrine Tumors". Science. 331 (6021): 1199–1203. doi:10.1126/science.1200609. PMID 21252315.
- ↑ McKenna, L. R.; Edil, B. H. (2014). "Update on pancreatic neuroendocrine tumors". Gland surgery. 3 (4): 258–275. doi:10.3978/j.issn.2227-684X.2014.06.03. PMID 25493258.
- ↑ PMID 18772397 (PMID 18772397)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand - ↑ PMID 19077451 (PMID 19077451)
Citation will be completed automatically in a few minutes. Jump the queue or expand by hand