Linaclotide
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
WARNING
See full prescribing information for complete Boxed Warning.
Pediatric Risk:
|
Overview
Linaclotide is a guanylate cyclase-C agonist that is FDA approved for the {{{indicationType}}} of irritable bowel syndrome with constipation (IBS-C), chronic idiopathic constipation (CIC). There is a Black Box Warning for this drug as shown here. Common adverse reactions include diarrhea, abdominal pain, flatulence and abdominal distension.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Irritable Bowel Syndrome with Constipation (IBS-C)
- The recommended dose of LINZESS is 290 mcg taken orally once daily on an empty stomach, at least 30 minutes prior to the first meal of the day.
Chronic Idiopathic Constipation (CIC)
- The recommended dose of LINZESS is 145 mcg taken orally once daily on an empty stomach, at least 30 minutes prior to the first meal of the day.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Linaclotide in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Linaclotide in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Linaclotide in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Linaclotide in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Linaclotide in pediatric patients.
Contraindications
- Pediatric patients under 6 years of age.
- Patients with known or suspected mechanical gastrointestinal obstruction.
Warnings
|
WARNING
See full prescribing information for complete Boxed Warning.
Pediatric Risk:
|
Precautions
- Pediatric Risk
- LINZESS is contraindicated in children under 6 years of age. The safety and effectiveness of LINZESS in pediatric patients under 18 years of age have not been established. In neonatal mice, increased fluid secretion as a consequence of GC-C agonism resulted in mortality within the first 24 hours due to dehydration. Due to increased intestinal expression of GC-C, children under 6 years of age may be more likely than older children and adults to develop significant diarrhea and its potentially serious consequences.
- Avoid use of LINZESS in pediatric patients 6 through 17 years of age. Although there were no deaths in older juvenile mice, given the deaths in young juvenile mice and the lack of clinical safety and efficacy data in pediatric patients, avoid the use of LINZESS in pediatric patients 6 through 17 years of age.
- Diarrhea
- Diarrhea was the most common adverse reaction of LINZESS-treated patients in the pooled IBS-C and CIC double-blind placebo-controlled trials. Severe diarrhea was reported in 2% of the LINZESS-treated patients. The incidence of diarrhea was similar between the IBS-C and CIC populations.
- Instruct patients to stop LINZESS if severe diarrhea occurs and to contact their healthcare provider. The healthcare provider should consider dose suspension and rehydration.
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
- During clinical development, approximately 2570, 2040, and 1220 patients with either IBS-C or CIC were treated with LINZESS for 6 months or longer, 1 year or longer, and 18 months or longer, respectively (not mutually exclusive).
Irritable Bowel Syndrome with Constipation (IBS-C)
- Most Common Adverse Reactions
- The data described below reflect exposure to LINZESS in the two placebo-controlled clinical trials involving 1605 adult patients with IBS-C (Trials 1 and 2). Patients were randomized to receive placebo or 290 mcg LINZESS once daily on an empty stomach for up to 26 weeks. Demographic characteristics were comparable between treatment groups. Table 1 provides the incidence of adverse reactions reported in at least 2% of IBS-C patients in the LINZESS treatment group and at an incidence that was greater than in the placebo group.
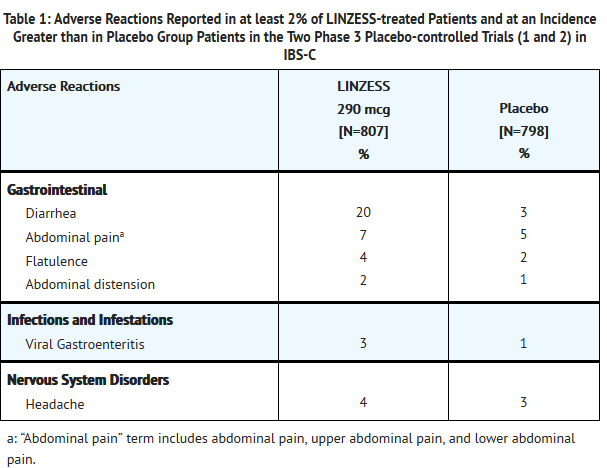
This image is provided by the National Library of Medicine.

- Diarrhea
- Diarrhea was the most commonly reported adverse reaction of the LINZESS-treated patients in the pooled IBS-C pivotal placebo-controlled trials. In these trials, 20% of LINZESS-treated patients reported diarrhea compared to 3% of placebo-treated patients. Severe diarrhea was reported in 2% of the LINZESS-treated patients versus less than 1% of the placebo-treated patients, and 5% of LINZESS-treated patients discontinued due to diarrhea vs less than 1% of placebo-treated patients. The majority of reported cases of diarrhea started within the first 2 weeks of LINZESS treatment. Fecal incontinence and dehydration were each reported in less than or equal to 1% of patients in the LINZESS treatment group.
- Adverse Reactions Leading to Discontinuation
- In placebo-controlled trials in patients with IBS-C, 9% of patients treated with LINZESS and 3% of patients treated with placebo discontinued prematurely due to adverse reactions. In the LINZESS treatment group, the most common reasons for discontinuation due to adverse reactions were diarrhea (5%) and abdominal pain (1%). In comparison, less than 1% of patients in the placebo group withdrew due to diarrhea or abdominal pain.
- Adverse Reactions Leading to Dose Reductions
- In the open-label, long-term trials, 2147 patients with IBS-C received 290 mcg of LINZESS daily for up to 18 months. In these trials, 29% of patients had their dose reduced or suspended secondary to adverse reactions, the majority of which were diarrhea or other GI adverse reactions.
- Other Adverse Reactions
- Adverse reactions that were reported in at least 1% and less than 2% of IBS-C patients in the LINZESS treatment group and at an incidence greater than in the placebo treatment group are listed below by body system:
Gastrointestinal Disorders
Gastroesophageal reflux disease, vomiting
General Disorders and Administration Site Conditions
- Other Adverse Events
- In placebo-controlled trials in patients with IBS-C, less than 1% LINZESS-treated patients and no placebo-treated patients reported hematochezia; no patient in either treatment group reported melena. Less than 1% of LINZESS-treated and placebo-treated patients reported allergic reactions, urticaria, or hives as adverse events.
Chronic Idiopathic Constipation (CIC)
- Most Common Adverse Reactions
- The data described below reflect exposure to LINZESS in the two double-blind placebo-controlled clinical trials of 1275 adult patients with CIC (Trials 3 and 4). Patients were randomized to receive placebo or 145 mcg LINZESS or 290 mcg LINZESS once daily on an empty stomach, for at least 12 weeks. Demographic characteristics were comparable between both LINZESS treatment groups and placebo [see Clinical Studies (14.2)]. Only data for the recommended LINZESS 145 mcg dose and placebo are presented. Table 2 provides the incidence of adverse reactions reported in at least 2% of CIC patients in the 145 mcg LINZESS treatment group and at an incidence that was greater than in the placebo treatment group.
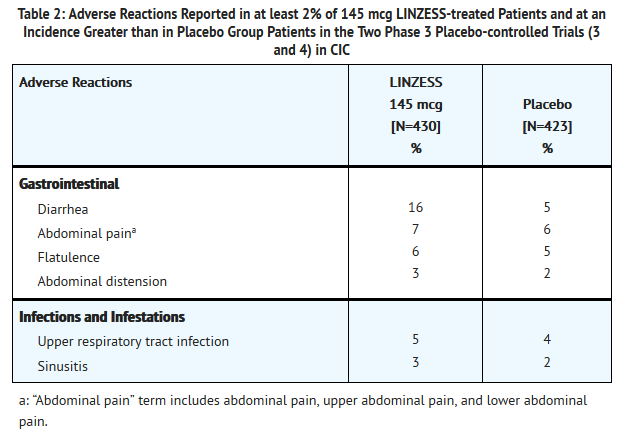
This image is provided by the National Library of Medicine.

- Diarrhea
- Diarrhea was the most commonly reported adverse reaction of the LINZESS-treated patients in the pooled CIC placebo-controlled trials. In these trials, 16% of LINZESS-treated patients reported diarrhea compared to 5% of placebo-treated patients. Severe diarrhea was reported in 2% of the 145 mcg LINZESS-treated patients versus less than 1% of the placebo-treated patients, and 5% of LINZESS-treated patients discontinued due to diarrhea vs less than 1% of placebo-treated patients. The majority of reported cases of diarrhea started within the first 2 weeks of LINZESS treatment. Fecal incontinence was reported in 1% of patients in the LINZESS treatment group, compared with less than 1% in the placebo group. Dehydration was reported in less than 1% of patients in the LINZESS treatment group.
- Adverse Reactions Leading to Discontinuation
- In placebo-controlled trials in patients with CIC, 8% of patients treated with LINZESS and 4% of patients treated with placebo discontinued prematurely due to adverse reactions. In the 145 mcg LINZESS treatment group, the most common reasons for discontinuation due to adverse reactions were diarrhea (5%) and abdominal pain (1%). In comparison, less than 1% of patients in the placebo group withdrew due to diarrhea or abdominal pain.
- Adverse Reactions Leading to Dose Reductions
- In the open-label, long-term trials, 1129 patients with CIC received 290 mcg of LINZESS daily for up to 18 months. In these trials, 27% of patients had their dose reduced or suspended secondary to adverse reactions, the majority of which were diarrhea or other GI adverse reactions.
- Other Adverse Reactions
- Adverse reactions that were reported in at least 1% of and less than 2% of CIC patients in the 145 mcg LINZESS treatment group and at an incidence greater than in the placebo treatment group are listed below by body system:
Gastrointestinal Disorders
Infections and Infestations
Viral gastroenteritis
- Other Adverse Events
- In placebo-controlled trials in patients with CIC, less than 1% of both LINZESS-treated and placebo-treated patients reported rectal hemorrhage, hematochezia or melena. Less than 1% of LINZESS-treated and placebo-treated patients reported allergic reactions, urticaria, or hives as adverse events.
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Linaclotide in the drug label.
Drug Interactions
- No drug-drug interaction studies have been conducted with LINZESS. Linaclotide and its active metabolite are not measurable in plasma following administration of the recommended clinical doses; hence, no systemic drug-drug interactions or drug interactions mediated by plasma protein binding of linaclotide or its metabolite are anticipated.
- Linaclotide does not interact with the cytochrome P450 enzyme system based on the results of in vitro studies. In addition, linaclotide is neither a substrate nor an inhibitor of the efflux transporter P-glycoprotein (P-gp).
Use in Specific Populations
Pregnancy
- Pregnancy Category C
- Risk Summary
- There are no adequate and well-controlled studies with LINZESS in pregnant women. In animal developmental studies, adverse fetal effects were observed only with maternal toxicity and at doses of linaclotide much higher than the maximum recommended human dose. LINZESS should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Animal Data
- The potential for linaclotide to cause teratogenic effects was studied in rats, rabbits and mice. Oral administration of up to 100,000 mcg/kg/day in rats and 40,000 mcg/kg/day in rabbits produced no maternal toxicity and no effects on embryo-fetal development. In mice, oral dose levels of at least 40,000 mcg/kg/day produced severe maternal toxicity including death, reduction of gravid uterine and fetal weights, and effects on fetal morphology. Oral doses of 5000 mcg/kg/day did not produce maternal toxicity or any adverse effects on embryo-fetal development in mice.
- The maximum recommended human dose is approximately 5 mcg/kg/day, based on a 60-kg body weight. Limited systemic exposure to linaclotide was achieved at the tested dose levels in animals (AUC = 40, 640, and 25 ng•hr/mL in rats, rabbits, and mice, respectively, at the highest dose levels), whereas no detectable exposure occurred in humans. Therefore, animal and human doses should not be compared directly for evaluating relative exposure.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Linaclotide in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Linaclotide during labor and delivery.
Nursing Mothers
- It is not known whether linaclotide is excreted in human milk; however, linaclotide and its active metabolite are not measurable in plasma following administration of the recommended clinical doses.
Caution should be exercised when LINZESS is administered to nursing women [see Contraindications (4), Warnings and Precautions (5.1) and Use in Specific Populations (8.4)].
Pediatric Use
- LINZESS is contraindicated in children under 6 years of age. The safety and effectiveness of LINZESS in pediatric patients under 18 years of age have not been established. In neonatal mice, increased fluid secretion as a consequence of GC-C agonism resulted in mortality due to dehydration. Due to increased intestinal expression of GC-C, children under 6 years of age may be more likely than older children and adults to develop diarrhea and its potentially serious consequences.
- Avoid use of LINZESS in pediatric patients 6 through 17 years of age. Although there were no deaths in older juvenile mice, given the deaths in young juvenile mice and the lack of clinical safety and efficacy data in pediatric patients, avoid the use of LINZESS in pediatric patients 6 through 17 years of age.
Geriatic Use
- Irritable Bowel Syndrome with Constipation (IBS-C)
- Of 1605 IBS-C patients in the placebo-controlled clinical studies of LINZESS, 85 (5%) were at least 65 years of age, while 20 (1%) were at least 75 years old. Clinical studies of LINZESS did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects.
- Chronic Idiopathic Constipation (CIC)
- Of 1275 CIC patients in the placebo-controlled clinical studies of LINZESS, 155 (12%) were at least 65 years of age, while 30 (2%) were at least 75 years old. Clinical trials of LINZESS did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects.
Gender
There is no FDA guidance on the use of Linaclotide with respect to specific gender populations.
Race
There is no FDA guidance on the use of Linaclotide with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Linaclotide in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Linaclotide in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Linaclotide in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Linaclotide in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
There is limited information regarding Monitoring of Linaclotide in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Linaclotide in the drug label.
Overdosage
Acute Overdose
- There is limited experience with overdose of LINZESS. During the clinical development program of LINZESS, single doses of 2897 mcg were administered to 22 healthy volunteers; the safety profile in these subjects was consistent with that in the overall LINZESS-treated population, with diarrhea being the most commonly reported adverse reaction.
Chronic Overdose
There is limited information regarding Chronic Overdose of Linaclotide in the drug label.
Pharmacology
Mechanism of Action
- Linaclotide is a guanylate cyclase-C (GC-C) agonist. Both linaclotide and its active metabolite bind to GC-C and act locally on the luminal surface of the intestinal epithelium. Activation of GC-C results in an increase in both intracellular and extracellular concentrations of cyclic guanosine monophosphate (cGMP). Elevation in intracellular cGMP stimulates secretion of chloride and bicarbonate into the intestinal lumen, mainly through activation of the cystic fibrosis transmembrane conductance regulator (CFTR) ion channel, resulting in increased intestinal fluid and accelerated transit. In animal models, linaclotide has been shown to both accelerate GI transit and reduce intestinal pain. The linaclotide-induced reduction in visceral pain in animals is thought to be mediated by increased extracellular cGMP, which was shown to decrease the activity of pain-sensing nerves.
Structure
- LINZESS (linaclotide) is a guanylate cyclase-C agonist. Linaclotide is a 14-amino acid peptide with the following chemical name: L-cysteinyl-L-cysteinyl-L-glutamyl-L-tyrosyl-L-cysteinyl-L-cysteinyl-L-asparaginyl-L-prolyl-L-alanyl-L-cysteinyl-L-threonyl-glycyl-L-cysteinyl-L-tyrosine, cyclic (1-6), (2-10), (5-13)-tris (disulfide).
- The molecular formula of linaclotide is C59H79N15O21S6 and its molecular weight is 1526.8. The amino acid sequence for linaclotide is shown below:
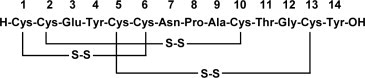
This image is provided by the National Library of Medicine.

- Linaclotide is an amorphous, white to off-white powder. It is slightly soluble in water and aqueous sodium chloride (0.9%). LINZESS contains linaclotide-coated beads in hard gelatin capsules. LINZESS is available as 145 mcg and 290 mcg capsules for oral administration.
- The inactive ingredients of LINZESS capsules include: calcium chloride dihydrate, L-leucine, hypromellose, microcrystalline cellulose, gelatin, and titanium dioxide.
Pharmacodynamics
- Although the pharmacologic effects of LINZESS in humans have not been fully evaluated, in clinical studies, LINZESS has been shown to change stool consistency as measured by the Bristol Stool Form Scale (BSFS) and increase stool frequency.
Pharmacokinetics
- Absorption
- LINZESS is minimally absorbed with low systemic availability following oral administration. Concentrations of linaclotide and its active metabolite in plasma are below the limit of quantitation after oral doses of 145 mcg or 290 mcg were administered. Therefore, standard pharmacokinetic parameters such as area under the curve (AUC), maximum concentration (Cmax), and half-life (t½) cannot be calculated.
- Distribution
- Given that linaclotide plasma concentrations following therapeutic oral doses are not measurable, linaclotide is expected to be minimally distributed to tissues.
- Metabolism
- Linaclotide is metabolized within the gastrointestinal tract to its principal, active metabolite by loss of the terminal tyrosine moiety. Both linaclotide and the metabolite are proteolytically degraded within the intestinal lumen to smaller peptides and naturally occurring amino acids.
- Elimination
- Active peptide recovery in the stool samples of fed and fasted subjects following the daily administration of 290 mcg of LINZESS for seven days averaged about 5% (fasted) and about 3% (fed) and virtually all as the active metabolite.
- Food Effect
- In a cross-over study, 18 healthy subjects were given LINZESS 290 mcg for 7 days both in the non-fed and fed state. Neither linaclotide nor its active metabolite was detected in the plasma. Taking LINZESS immediately after the high fat breakfast resulted in looser stools and a higher stool frequency compared with taking it in the fasted state. In clinical trials, LINZESS was administered on an empty stomach, at least 30 minutes before breakfast.
- Specific Populations
- Age and Gender
- Clinical studies to determine the impact of age and gender on the pharmacokinetics of LINZESS have not been conducted.
- Hepatic Impairment
- LINZESS has not been specifically studied in patients who have hepatic impairment. Hepatic impairment is not expected to affect the metabolism or clearance of the parent drug or its metabolite because linaclotide is metabolized within the gastrointestinal tract.
- Renal Impairment
- LINZESS has not been specifically studied in patients who have renal impairment. Renal impairment is not expected to affect clearance of the parent drug or its metabolite because linaclotide has low systemic availability following oral administration and is metabolized within the gastrointestinal tract.
Nonclinical Toxicology
- Carcinogenesis
- In 2-year carcinogenicity studies, linaclotide was not tumorigenic in rats at doses up to 3500 mcg/kg/day or in mice at doses up to 6000 mcg/kg/day. The maximum recommended human dose is approximately 5 mcg/kg/day based on a 60-kg bodyweight. Limited systemic exposure to linaclotide was achieved at the tested dose levels in animals, whereas no detectable exposure occurred in humans. Therefore, animal and human doses should not be compared directly for evaluating relative exposure.
- Mutagenesis
- Linaclotide was not genotoxic in an in vitro bacterial reverse mutation (Ames) assay or in the in vitro chromosomal aberration assay in cultured human peripheral blood lymphocytes.
- Impairment of Fertility
- Linaclotide had no effect on fertility or reproductive function in male and female rats at oral doses of up to 100,000 mcg/kg/day.
- Animal Toxicology and/or Pharmacology
- In toxicology studies in neonatal mice, linaclotide caused deaths at 10 mcg/kg/day after oral administration of 1 or 2 daily doses on post-natal day 7. These deaths were due to rapid and severe dehydration produced by significant fluid shifts into the intestinal lumen resulting from GC-C agonism in neonatal mice. Supplemental subcutaneous fluid administration prevented death after linaclotide administration in neonatal mice.
- In studies conducted without supplemental fluid administration, tolerability to linaclotide increases with age in juvenile mice. In 2-week-old mice, linaclotide was well tolerated at a dose of 50 mcg/kg/day, but deaths occurred after a single oral dose of 100 mcg/kg. In 3-week-old mice, linaclotide was well tolerated at 100 mcg/kg/day, but deaths occurred after a single oral dose of 600 mcg/kg. Linaclotide was well tolerated and did not cause death in 4-week-old juvenile mice at a dose of 1,000 mcg/kg/day for 7 days and in 6-week-old juvenile mice at a dose of 20,000 mcg/kg/day for 28 days
- Linaclotide did not cause death in adult mice, rats, rabbits and monkeys at dose levels up to 5,000 mcg/kg/day. The maximum recommended dose in adults is approximately 5 mcg/kg/day, based on a 60-kg body weight. Animal and human doses of linaclotide should not be compared directly for evaluating relative exposure.
Clinical Studies
Irritable Bowel Syndrome with Constipation (IBS-C)
- The efficacy of LINZESS for the management of symptoms of IBS-C was established in two double-blind, placebo-controlled, randomized, multicenter trials in adult patients (Trials 1 and 2). A total of 800 patients in Trial 1 and 804 patients in Trial 2 [overall mean age of 44 years (range 18 - 87 years with 5% at least 65 years of age), 90% female, 77% white, 19% black, and 12% Hispanic] received treatment with LINZESS 290 mcg or placebo once daily and were evaluated for efficacy. All patients met Rome II criteria for IBS and were required, during the 2-week baseline period, to meet the following criteria:
- a mean abdominal pain score of at least 3 on a 0-to-10-point numeric rating scale
- less than 3 complete spontaneous bowel movements (CSBMs) per week [a CSBM is a spontaneous bowel movement (SBM) that is associated with a sense of complete evacuation; a SBM is a bowel movement occurring in the absence of laxative use], and
- less than or equal to 5 SBMs per week.
- The trial designs were identical through the first 12 weeks, and thereafter differed only in that Trial 1 included a 4-week randomized withdrawal (RW) period, and Trial 2 continued for 14 additional weeks (total of 26 weeks) of double-blind treatment. During the trials, patients were allowed to continue stable doses of bulk laxatives or stool softeners but were not allowed to take laxatives, bismuth, prokinetic agents, or other drugs to treat IBS-C or chronic constipation.
- Efficacy of LINZESS was assessed using overall responder analyses and change-from-baseline endpoints. Results for endpoints were based on information provided daily by patients in diaries.
- The 4 primary efficacy responder endpoints were based on a patient being a weekly responder for either at least 9 out of the first 12 weeks of treatment or at least 6 out of the first 12 weeks of treatment. For the 9 out of 12 weeks combined primary responder endpoint, a patient had to have at least a 30% reduction from baseline in mean abdominal pain, at least 3 CSBMs and an increase of at least 1 CSBM from baseline, all in the same week, for at least 9 out of the first 12 weeks of treatment. Each of the 2 components of the 9 out of 12 weeks combined responder endpoint, abdominal pain and CSBMs, was also a primary endpoint.
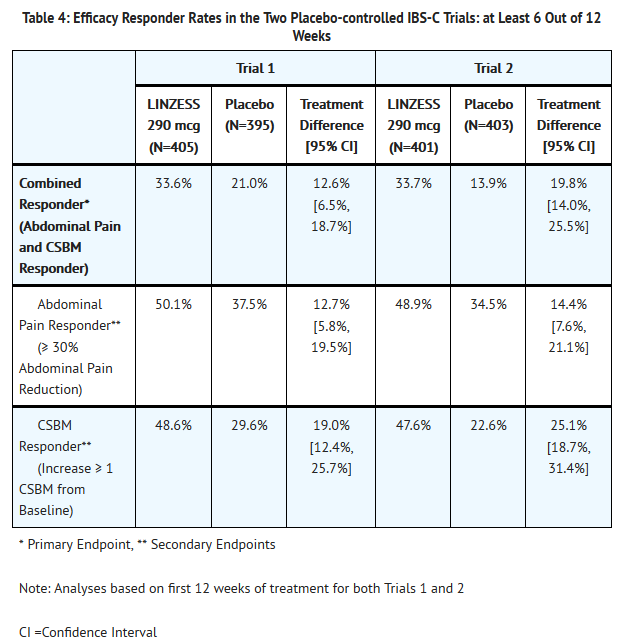
- For the 6 out of 12 weeks combined primary responder endpoint, a patient had to have at least a 30% reduction from baseline in mean abdominal pain and an increase of at least 1 CSBM from baseline, all in the same week, for at least 6 out of the first 12 weeks of treatment. To be considered a responder for this analysis, patients did not have to have at least 3 CSBMs per week.
- The efficacy results for the 9 out of 12 weeks and the 6 out of 12 weeks responder endpoints are shown in Tables 3 and 4, respectively. In both trials, the proportion of patients who were responders to LINZESS 290 mcg was statistically significantly higher than with placebo.
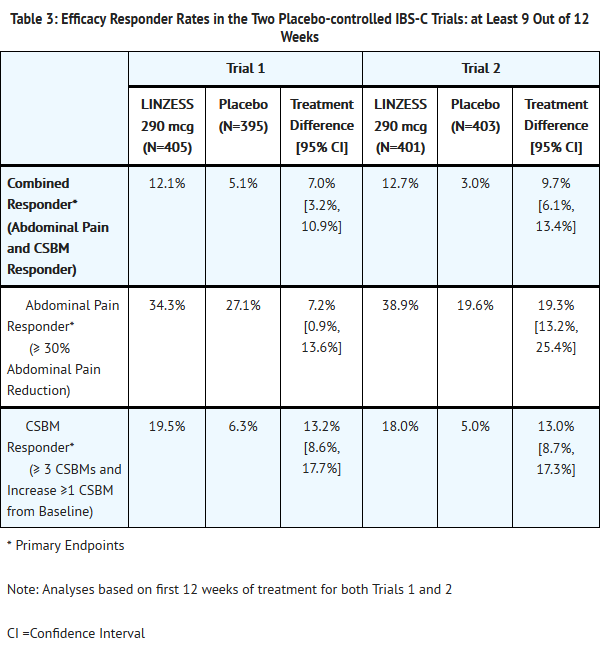
This image is provided by the National Library of Medicine.

This image is provided by the National Library of Medicine.

- In each trial, improvement from baseline in abdominal pain and CSBM frequency was seen over the first 12-weeks of the treatment periods. For change from baseline in the 11-point abdominal pain scale, LINZESS 290 mcg began to separate from placebo in the first week. Maximum effects were seen at weeks 6 - 9 and were maintained until the end of the study. The mean treatment difference from placebo at week 12 was a decrease in pain score of approximately 1.0 point in both trials (using an 11-point scale). Maximum effect on CSBM frequency occurred within the first week, and for change from baseline in CSBM frequency at week 12, the difference between placebo and LINZESS was approximately 1.5 CSBMs per week in both trials.
- During the 4-week randomized withdrawal period in Trial 1, patients who received LINZESS during the 12-week treatment period were re-randomized to receive placebo or continue treatment on LINZESS 290 mcg. In LINZESS-treated patients re-randomized to placebo, CSBM frequency and abdominal-pain severity returned toward baseline within 1 week and did not result in worsening compared to baseline. Patients who continued on LINZESS maintained their response to therapy over the additional 4 weeks. Patients on placebo who were allocated to LINZESS had an increase in CSBM frequency and a decrease in abdominal pain levels that were similar to the levels observed in patients taking LINZESS during the treatment period.
Chronic Idiopathic Constipation (CIC)
- The efficacy of LINZESS for the management of symptoms of CIC was established in two double-blind, placebo-controlled, randomized, multicenter clinical trials in adult patients (Trials 3 and 4). A total of 642 patients in Trial 3 and 630 patients in Trial 4 [overall mean age of 48 years (range 18 - 85 years with 12% at least 65 years of age), 89% female, 76% white, 22% black, 10% Hispanic] received treatment with LINZESS 145 mcg, 290 mcg, or placebo once daily and were evaluated for efficacy. All patients met modified Rome II criteria for functional constipation. Modified Rome II criteria were less than 3 Spontaneous Bowel Movements (SBMs) per week and 1 of the following symptoms for at least 12 weeks, which need not be consecutive, in the preceding 12 months:
- Straining during greater than 25% of bowel movements
- Lumpy or hard stools during greater than 25% of bowel movements
- Sensation of incomplete evacuation during greater than 25% of bowel movements
- Patients were also required to have less than 3 CSBMs per week and less than or equal to 6 SBMs per week during a 2-week baseline period. Patients were excluded if they met criteria for IBS-C or had fecal impaction that required emergency room treatment.
- The trial designs were identical through the first 12 weeks. Trial 3 also included an additional 4-week randomized withdrawal (RW) period. During the trials, patients were allowed to continue stable doses of bulk laxatives or stool softeners but were not allowed to take laxatives, bismuth, prokinetic agents, or other drugs to treat chronic constipation.
- Efficacy of LINZESS was assessed using overall responder analysis and change-from-baseline endpoints. Results for endpoints were based on information provided daily by patients in diaries.
- A CSBM overall responder in the CIC trials was defined as a patient who had at least 3 CSBMs and an increase of at least 1 CSBM from baseline in a given week for at least 9 weeks out of the 12-week treatment period. The CSBM responder rates are shown in Table 5. During the individual double-blind placebo-controlled trials, LINZESS 290 mcg did not consistently offer additional clinically meaningful treatment benefit over placebo than that observed with the LINZESS 145 mcg dose. Therefore, the 145 mcg dose is the recommended dose. Only the data for the approved 145 mcg dose of LINZESS are presented in Table 5.
- In Trials 3 and 4, the proportion of patients who were CSBM responders was statistically significantly greater with the LINZESS 145 mcg dose than with placebo.
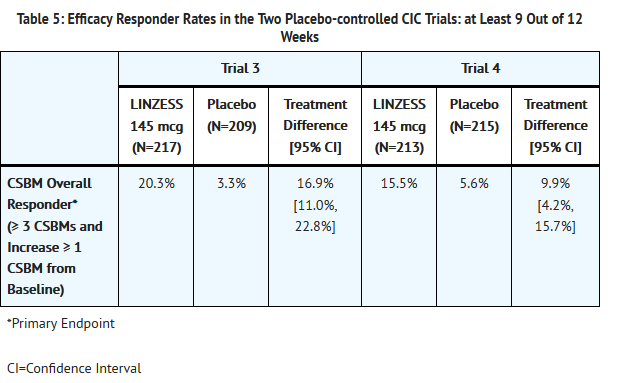
This image is provided by the National Library of Medicine.

- CSBM frequency reached maximum level during week 1 and was also demonstrated over the remainder of the 12-week treatment period in Trial 3 and Trial 4. For the mean change from baseline in CSBM frequency at week 12, the difference between placebo and LINZESS was approximately 1.5 CSBMs.
- On average, patients who received LINZESS across the 2 trials had significantly greater improvements compared with patients receiving placebo in stool frequency (CSBMs/week and SBMs/week), and stool consistency (as measured by the BSFS).
- During the 4-week randomized withdrawal period in Trial 3, patients who received LINZESS during the 12-week treatment period were re-randomized to receive placebo or continue treatment on the same dose of LINZESS taken during the treatment period. In LINZESS-treated patients re-randomized to placebo, CSBM and SBM frequency returned toward baseline within 1 week and did not result in worsening compared to baseline. Patients who continued on LINZESS maintained their response to therapy over the additional 4 weeks. Patients on placebo who were allocated to LINZESS had an increase in CSBM and SBM frequency similar to the levels observed in patients taking LINZESS during the treatment period.
How Supplied
- 145 mcg Capsules: White to off-white opaque hard gelatin capsules with grey imprint "FL 145"
- Bottle of 30: NDC 0456-1201-30
- 290 mcg Capsules: White to off-white opaque hard gelatin capsules with grey imprint "FL 290"
- Bottle of 30: NDC 0456-1202-30
- Storage
- Store at 25°C (77°F); excursions permitted between 15°C and 30°C (59°F and 86°F) [see USP Controlled Room Temperature].
- Keep LINZESS in the original container. Do not subdivide or repackage. Protect from moisture. Do not remove desiccant from the container. Keep bottles tightly closed in a dry place.
Storage
There is limited information regarding Linaclotide Storage in the drug label.
Images
Drug Images
 |
Drug Name: |
| This pill image is provided by the National Library of Medicine's PillBox. |
Package and Label Display Panel
 |
| This image of the FDA label is provided by the National Library of Medicine. |
 |
| This image of the FDA label is provided by the National Library of Medicine. |
 |
| This image of the FDA label is provided by the National Library of Medicine. |
Patient Counseling Information
- Patients should be instructed as follows:
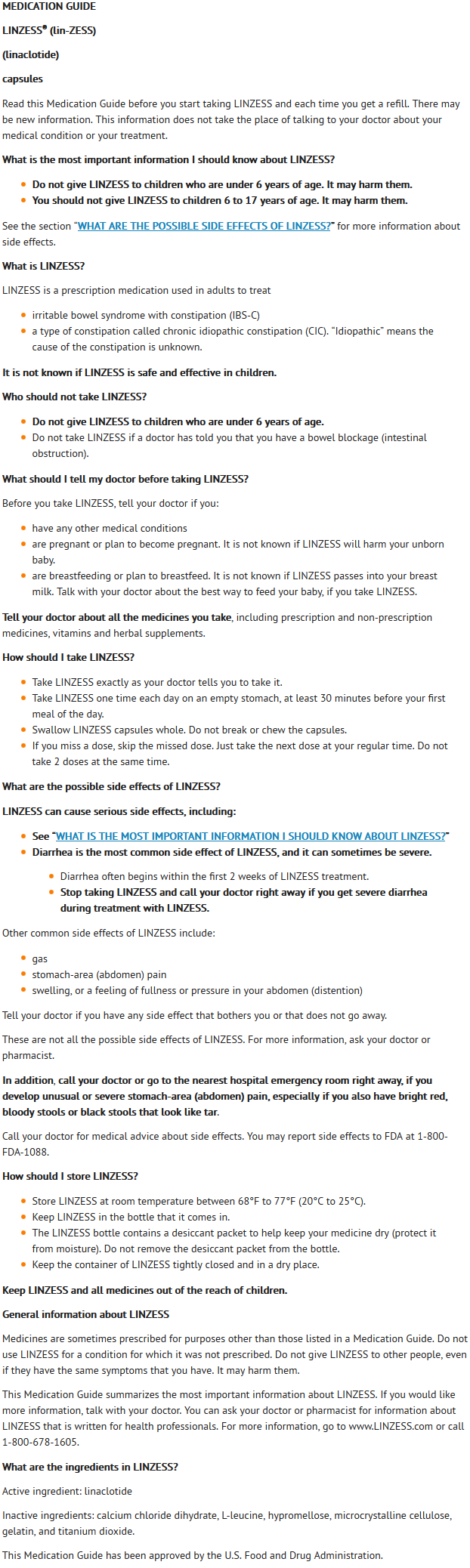
- Do not give LINZESS to children who are under 6 years of age. It may harm them. You should not give LINZESS to children 6 to 17 years of age. It may harm them.
- Keep LINZESS in the original container. Do not subdivide or repackage. Protect from moisture. Do not remove desiccant from the container. Keep bottles closed tightly in a dry place.
- Take LINZESS once daily on an empty stomach as prescribed. Swallow the capsule whole and do not break apart or chew.
- If you miss a dose, skip the missed dose. Just take the next dose at your regular time. Do not take 2 doses at the same time.
- Stop LINZESS and contact your physician if you experience severe diarrhea.
- Seek immediate medical attention if you develop unusual or severe abdominal pain, and /or severe diarrhea, especially if in combination with hematochezia or melena.
This image is provided by the National Library of Medicine.

{kind=link}
Precautions with Alcohol
- Alcohol-Linaclotide interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- LINZESS®[1]
Look-Alike Drug Names
There is limited information regarding Linaclotide Look-Alike Drug Names in the drug label.
Price
References
The contents of this FDA label are provided by the National Library of Medicine.