Hydrocephalus MRI
Jump to navigation
Jump to search
|
Hydrocephalus Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Hydrocephalus MRI On the Web |
|
American Roentgen Ray Society Images of Hydrocephalus MRI |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Syed Ahsan Hussain, M.D.[2]
MRI
- The MRI findings are given below:[1][2][3]
- Ventricular enlargement not entirely attributable to cerebral atrophy or congenital enlargement (Evans index >0.3).
- No macroscopic obstruction to CSF flow.
- Enlargement of the temporal horns of the lateral ventricles not entirely attributable to hippocampus atrophy.
- Callosal angle of 40º or greater. Evidence of altered brain water content, including periventricular signal changes on CT and MRI not attributable to microvascular ischemic *Changes or demyelination. An aqueductal or fourth ventricular flow void.
- Phase-contrast MRI to measure the volume of CSF flowing through the aqueduct in either direction over a cardiac cycle.
- When this aqueductal CSF stroke volume is sufficiently elevated, there is an excellent chance of shunt responsiveness (100% positive predictive value).
- Idiopathic NPH appears to be a "two-hit" disease-benign external hydrocephalus (BEH) in infancy followed by DWMI in late adulthood.
- As BEH occurs when the sutures are still open, these infants present with large heads, a finding also noted in patients with NPH.
- Although BEH has been attributed to immature arachnoidal granulations with decreased CSF resorptive capacity, this now appears to be permanent and may lead to a parallel pathway for CSF resorption via the extracellular space of the brain.
- With DWMI, the myelin lipid is lost, exposing the polar water molecules to myelin protein, increasing resistance to CSF outflow and leading to backing up of CSF and hydrocephalus.
Marked Hyrocephalus



Aqueductal Stenosis
-
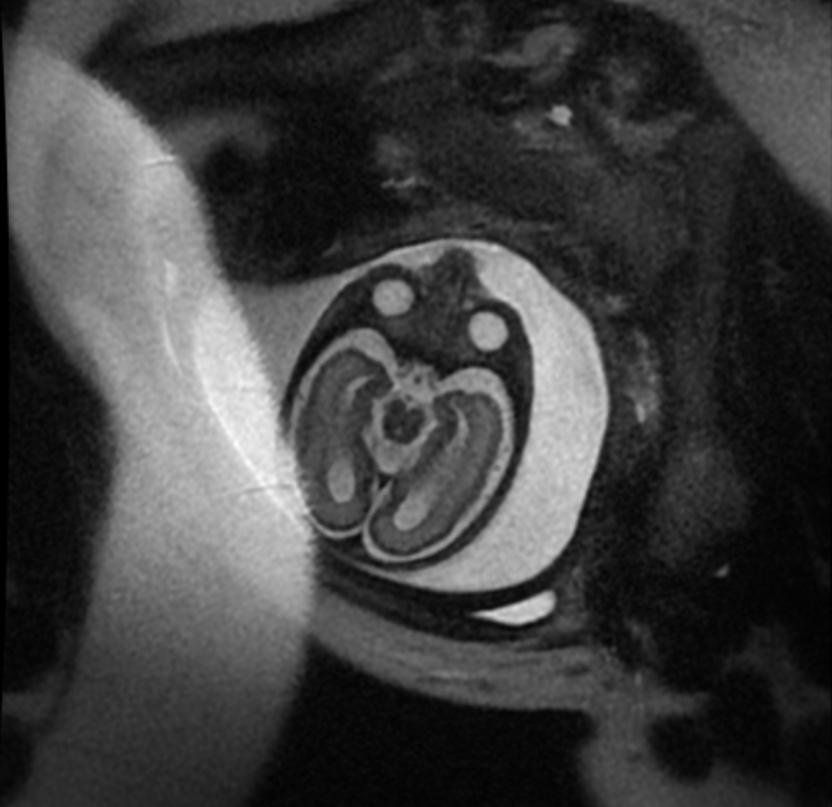 Fetal MRI: Aqueductal stenosis
Fetal MRI: Aqueductal stenosis -
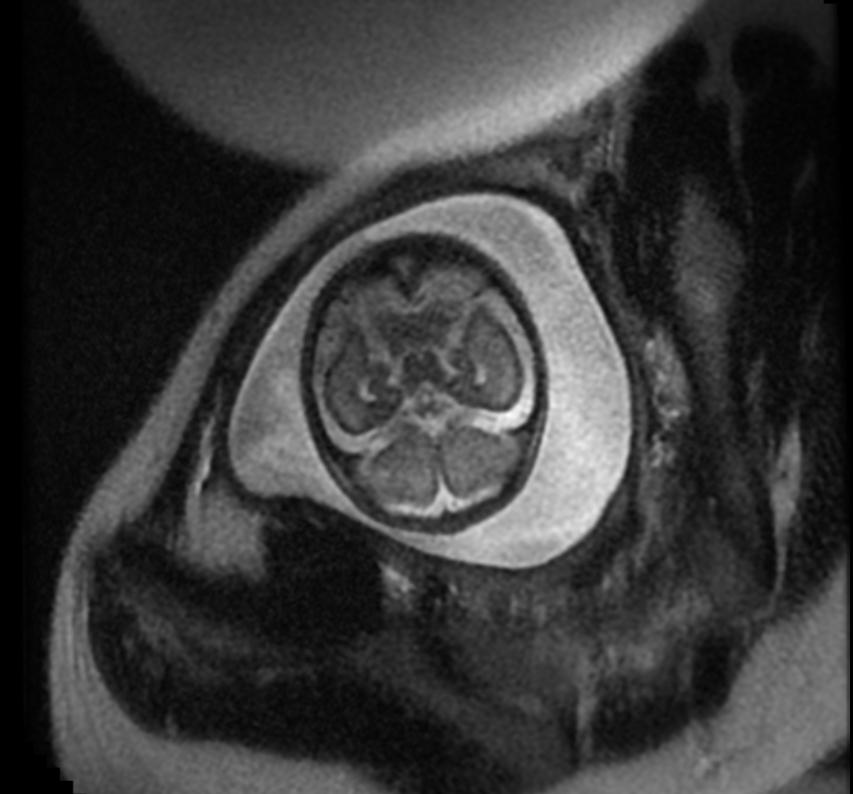 Fetal MRI: Aqueductal stenosis
Fetal MRI: Aqueductal stenosis -
 Fetal MRI: Aqueductal stenosis
Fetal MRI: Aqueductal stenosis -
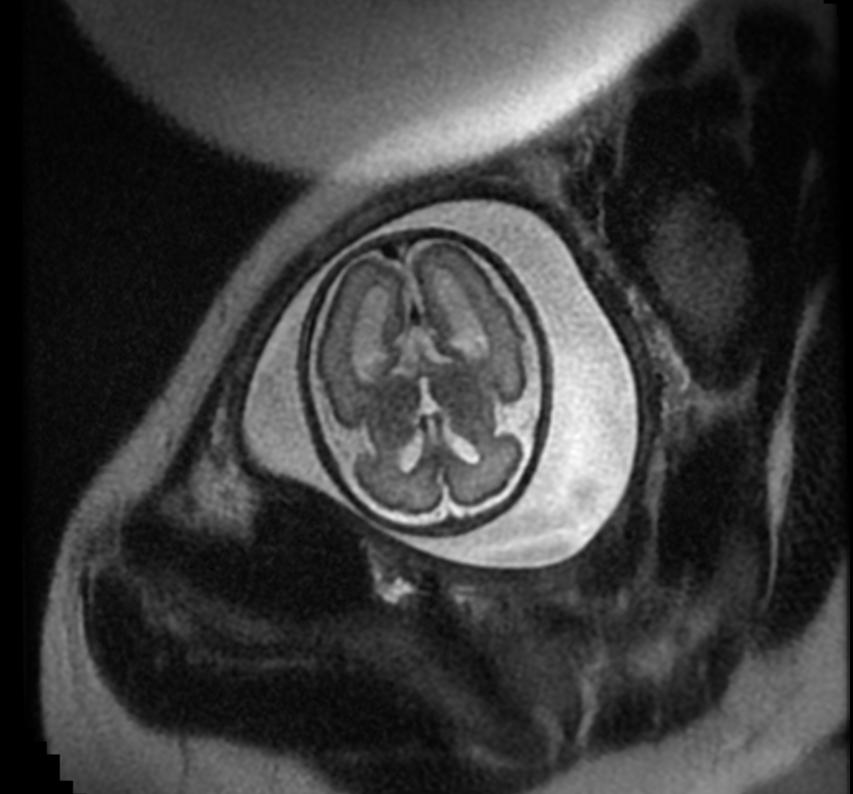 Fetal MRI: Aqueductal stenosis
Fetal MRI: Aqueductal stenosis -
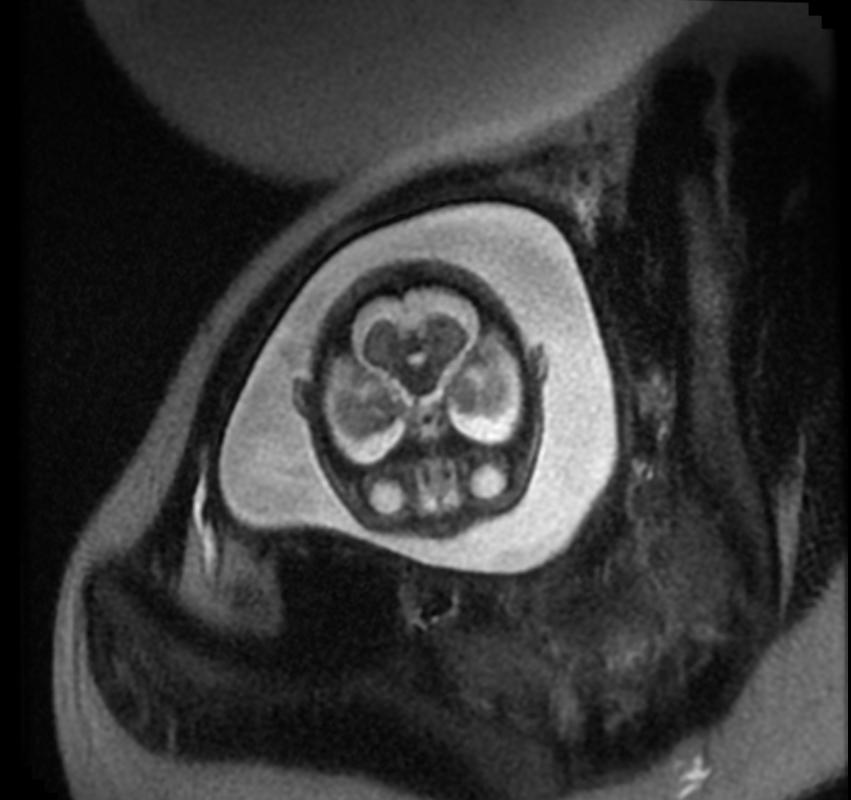 Fetal MRI: Aqueductal stenosis
Fetal MRI: Aqueductal stenosis





It gives better visualisation of microstructral changes in periventricular white matter areas than conventional MRI[4]
References
- ↑ Bradley WG (April 2016). "Magnetic Resonance Imaging of Normal Pressure Hydrocephalus". Semin. Ultrasound CT MR. 37 (2): 120–8. doi:10.1053/j.sult.2016.01.005. PMID 27063662.
- ↑ Mori E, Ishikawa M, Kato T, Kazui H, Miyake H, Miyajima M, Nakajima M, Hashimoto M, Kuriyama N, Tokuda T, Ishii K, Kaijima M, Hirata Y, Saito M, Arai H (2012). "Guidelines for management of idiopathic normal pressure hydrocephalus: second edition". Neurol. Med. Chir. (Tokyo). 52 (11): 775–809. PMID 23183074.
- ↑ Agarwal A, Bathla G, Kanekar S (April 2016). "Imaging of Communicating Hydrocephalus". Semin. Ultrasound CT MR. 37 (2): 100–8. doi:10.1053/j.sult.2016.02.007. PMID 27063660.
- ↑ Hattingen E, Jurcoane A, Melber J; et al. (2010). "Diffusion tensor imaging in patients with adult chronic idiopathic hydrocephalus". Neurosurgery. 66 (5): 917–24. doi:10.1227/01.NEU.0000367801.35654.EC. PMID 20404696. Unknown parameter
|month=ignored (help)