Dupuytrens contracture
| Dupuytren's contracture | |
 | |
|---|---|
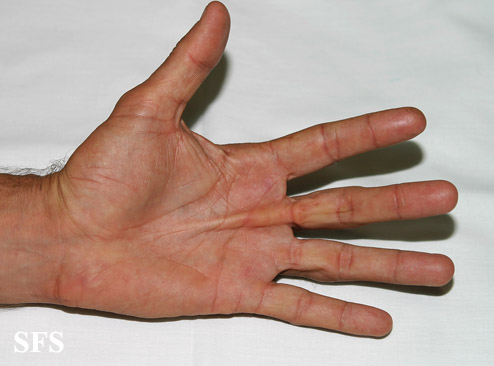
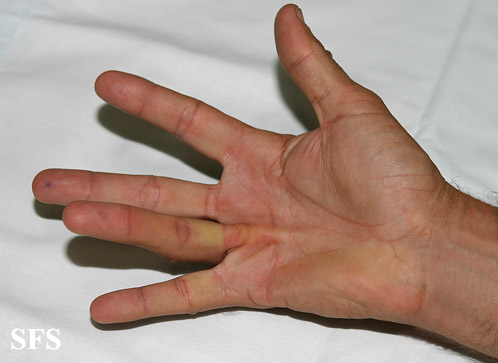
| Dupuytren's contracture of the fourth digit (ring finger). | |
| ICD-10 | M72.0 |
| ICD-9 | 728.6 |
| OMIM | 126900 |
| DiseasesDB | 4011 |
| MedlinePlus | 001233 |
Editors-In-Chief: Mohamed Riad, M.D.[1], Matthew I. Leibman, M.D.[2]; Mark R. Belsky, M.D.[3]; David E. Ruchelsman, M.D.[4]Kiran Singh, M.D. [5]
Synonyms and keywords: Dupuytren contracture I, included; DUPC1; palmar fascial fibromatosis; palmar fibromatosis
Overview
Dupuytren's contracture (also known as Morbus Dupuytren) is an abnormal thickening of the hand (palmar fascia) causing curling of fingers and impaired function of the fingers, especially the little and ring fingers.. It is named after the famous surgeon Baron Guillaume Dupuytren, who described an operation to correct the affliction. It is thought that Dupuytren's contracture is the result of microvascular angiopathy. The incidence of Dupuytren's contracture increases with age; the median age at diagnosis is 50-70 years. men are affected more often than women. Common risk factors in the development of Dupuytren's contracture include family history, diabetes, antiepileptic medications, liver disease, smoking, alcoholism and manual work. Dupuytren’s disease is progressive in nature with no available definitive cure.
Historical Perspective
- Dupuytren's contracture was named after Baron Guillaume Dupuytren, a famous surgeon, following describing an operation to correct the affliction.
Pathophysiology
Pathogenesis
- The exact pathogenesis of Dupuytren's contracture is not fully understood.
- It is thought that Dupuytren's contracture is the result of microvascular angiopathy.
Associated Conditions
Causes
The cause of Dupuytren's contracture has not been identified.
Epidemiology and Demographics
Prevalence
- The prevalence of Dupuytren's contracture among the UK population is 3-5%.
Age
- The incidence of Dupuytren's contracture increases with age; the median age at diagnosis is 50-70 years.
Race
- Dupuytren's contracture usually affects individuals of the northern Europeans race (Icelandic and Scandinavian populations).
Gender
- Males are more commonly affected by Dupuytren's contracture than females. The male to female ratio is approximately 3 to 1.
Risk Factors
Common risk factors in the development of Dupuytren's contracture include:
- Family history: genetic predisposition may account for 80% of cases.
- Diabetes and its medications
- Smoking
- Alcohol intake
- Antiepileptic medications
- There is also some speculation that Dupuytren's contracture may be caused by physical trauma, such as manual labor or other over-exertion of the hands. However, the fact that Dupuytren's is not connected with handedness casts some doubt on this claim.
- Surgery of the hand may trigger growth of Dupuytren nodules and cords if an inclination existed before.
- Certain occupations with repetitive hand trauma
Natural History, Complications and Prognosis
Natural History
- Dupuytren’s disease is progressive in nature with no available definitive cure.
- Improvement of the painful nodules may occur with time, and many patients never experience a contracture.
Complications
- Ectopic disease involving the penis (Pyronie's disease) or the feet (Ledderhose disease)
- Limitation of daily activities and work capabilities
Prognosis
- Prognosis is generally poor.
- Development of Dupuytren's disease at an earlier age is associated with more severe deformities.
Diagnosis
Diagnostic Study of Choice
Dupuytren’s disease is primarily diagnosed based on the clinical presentation.
History and Symptoms
- Symptoms of Dupuytren's disease include abnormal thickening of the hand (palmar fascia) causing curling of fingers and impaired function of the fingers, especially the little and ring fingers.
- It usually has a gradual onset, often beginning as a tender lump in the palm.
- It often starts as a nodule, usually in line with the ring finger.
- Over time, pain associated with the condition tends to go away, but tough bands of tissue may develop.
- These bands, which are the source of the reduced mobility commonly associated with the condition, are visible on the surface of the palm, and may appear similar to a small callus.
- It commonly develops in both hands, and has no connection to dominant- or non-dominant hands, nor any correlation with right- or left-handedness.
- The contracture sets on very slowly, especially in women. However, when present in both hands, and when there is associated foot involvement, it tends to accelerate more rapidly.
Physical Examination
- The earliest sign of a Dupuytren's contracture is a triangular "puckering" of the palmar skin over the flexor tendon just before the flexor crease of the finger, at the metacarpophalangeal joint.
- The most commonly affected finger is the ring and little finger. The thumb and index fingers rarely involved.
-
 Dupuytren contracture. Adapted from Dermatology Atlas.
Dupuytren contracture. Adapted from Dermatology Atlas. -
 Dupuytren contracture. Adapted from Dermatology Atlas.
Dupuytren contracture. Adapted from Dermatology Atlas. -
 Dupuytren contracture. Adapted from Dermatology Atlas.
Dupuytren contracture. Adapted from Dermatology Atlas. -
 Dupuytren contracture. Adapted from Dermatology Atlas.
Dupuytren contracture. Adapted from Dermatology Atlas. -
 Dupuytren contracture. Adapted from Dermatology Atlas.
Dupuytren contracture. Adapted from Dermatology Atlas. -
 Dupuytren contracture. Adapted from Dermatology Atlas.
Dupuytren contracture. Adapted from Dermatology Atlas.






Treatment
Medical Therapy
- Pharmacologic medical therapies for Dupuytren's disease include pain management and corticosteroid injection into the nodules,
- In some cases, repeated corticosteroid injections may cause softening of the nodules and slow down the disease progression.
- Most cases with simple nodules and without significant functional impairment benefit from conservative medical therapy.
Interventions
Collagenase clostridium histolyticum (CCH) injections
- The mechanism of action is to weaken the contracted cord by breaking down collagen.
- It is done in an outpatient practice but requires another clinic visit to snap the cord.
- I t is generally safe; however several complications were reported, such as tendon rupture and pulley injury.
- CCH injectiont is available in only North America after its withdrawal from European, Australian, and Asian markets.
Surgery
Surgery is not the first-line treatment option for patients with Dupuytren's disease. Surgery is usually reserved for patients with either:
- Rapid progression over a few months
- Severe thumb contractures with functional impairment
- More than 30° metacarpophalangeal joint contracture or 10-20° proximal interphalangeal joint contracture
The choice of the type of surgery depends the following variables:
- Severity of the disease
- Individual characteristics (such as age, occupation, degree of functional disability)
- Patient and/or physician preference
Surgical options include:
- Percutaneous needle fasciotomy (PNF): involves division of the cord using a needle. It is generally effective and safe with no complications; however tendon and digital nerve and vessel damage were reported in some cases. Its efficacy is low in the management of extensive contractures or contractures involving the proximal interphalangeal joints. The recurrence rate is high.
- Fasciectomy either partial (segmental aponeurectomy) or complete (limited fasciectomy): involves excision of the cord with higher rate of complications PNF.
- Dermofasciectomy: a more invasive procedure that involves excising the whole diseased tissue, along with the overlying subcutaneous fat and skin. It is reserved for more severe cases with extensive skin involvement when the other surgical options have failed. The complication rate is the highest among the three surgical options. The recurrence rate is low.
External links
http://www.nlm.nih.gov/medlineplus/ency/article/001233.htm
Template:Diseases of the musculoskeletal system and connective tissue
de:Morbus Dupuytren
it:Malattia di Dupuytren
nl:Ziekte van Dupuytren