Aortic coarctation pathophysiology
Jump to navigation
Jump to search
| https://https://www.youtube.com/watch?v=0OqTJwZkRL4%7C350}} |
|
Aortic coarctation Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Aortic coarctation pathophysiology On the Web |
|
American Roentgen Ray Society Images of Aortic coarctation pathophysiology |
|
Risk calculators and risk factors for Aortic coarctation pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[4]
Overview
An aortic coarctation results from both, congenital and acquired means. Factors directly influencing the pathophysiology include defect location and sites of secondary dilation.
Pathophysiology
-
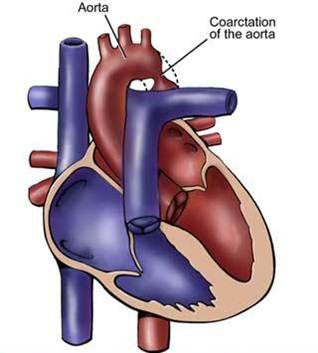 Coarctation of the descending aorta.
Coarctation of the descending aorta. -
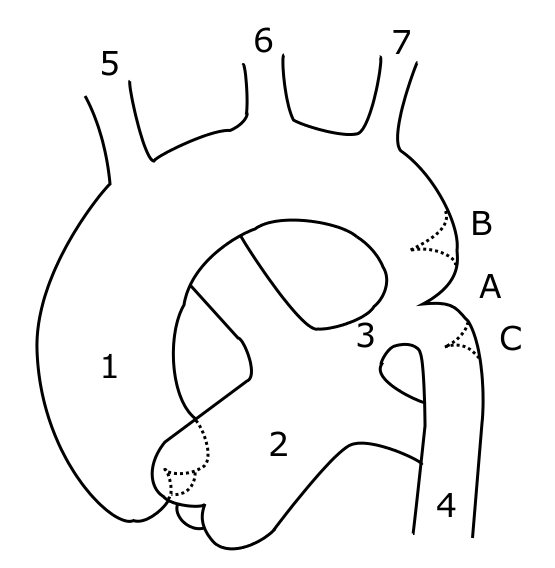 Schematic drawing of alternative locations of a coarctation of the aorta, relative to the ductus arteriosus. A: ductal coarctation, B: preductal coarctation, C: postductal coarctation. 1: Aorta ascendens, 2: Arteria pulmonalis, 3: Ductus arteriosus, 4: Aorta descendens, 5: Trunchus brachiocephalicus, 6: Arteria carotis communis sinister, 7: Arteria subclavia sinister
Schematic drawing of alternative locations of a coarctation of the aorta, relative to the ductus arteriosus. A: ductal coarctation, B: preductal coarctation, C: postductal coarctation. 1: Aorta ascendens, 2: Arteria pulmonalis, 3: Ductus arteriosus, 4: Aorta descendens, 5: Trunchus brachiocephalicus, 6: Arteria carotis communis sinister, 7: Arteria subclavia sinister


Coarctation of the aorta can be:
- Congenital coarctation resulting from an infolding of the aortic media that incorportaes ductal tissue, forming a ridge that eccentrically narrows the lumen of the vessel. Subsequent intimal proliferation on the ridge leads to progressive narrowing of the vessel lumen. There is a dilatation before and after the narrowing, giving the aorta an hourglass appearance. The exact etiology of the aortic abnormality remains unclear but likely involves a defect in the vascular wall of the aorta due to reduced antegrade intrauterine blood flow or to constriction of ductal tissue extending into the thoracic aorta.
- Acquired coarctation occurring in systemic arteritides such as Takayasu arteritis. Additionally it may occur in rare cases of severe atherosclerosis.
Defect Location

- 95% of the lesions are located distal to the left subclavian artery and proximal to the ductus arteriosus (preductal coarctation) or just at or distal to the ductus (postductal coarctation).
- 5% of coarctations are located proximal to the left subclavian artery, or rarely in the abdominal aorta.
- In some cases, coarctation presents as a long segment or a tubular hypoplasia.
- The stenosis is caused by an infolding of the left posterolateral aspect of the aortic wall resulting in an eccentric narrowing.
Sites of Secondary Dilation
- Aorta proximal to the coarct
- Aorta distal to the coarctation
- Left subclavian artery
- The narrowing progresses throughout life, and extensive collaterals develop from the subclavian (predominantly) and axillary arteries through:
- Internal mammary artery
- Scapular artery
- Intercostal arteries
- Epigastric arteries
- Anterior spinal arteries
Genetics
- Aortic coarctation, like many congenital heart diseases, is more common in patients with other genetic conditions.
- As many as 10-25% of patients with Turner syndrome have an accompanying coarctation of the aorta.
Gross Pathology
-
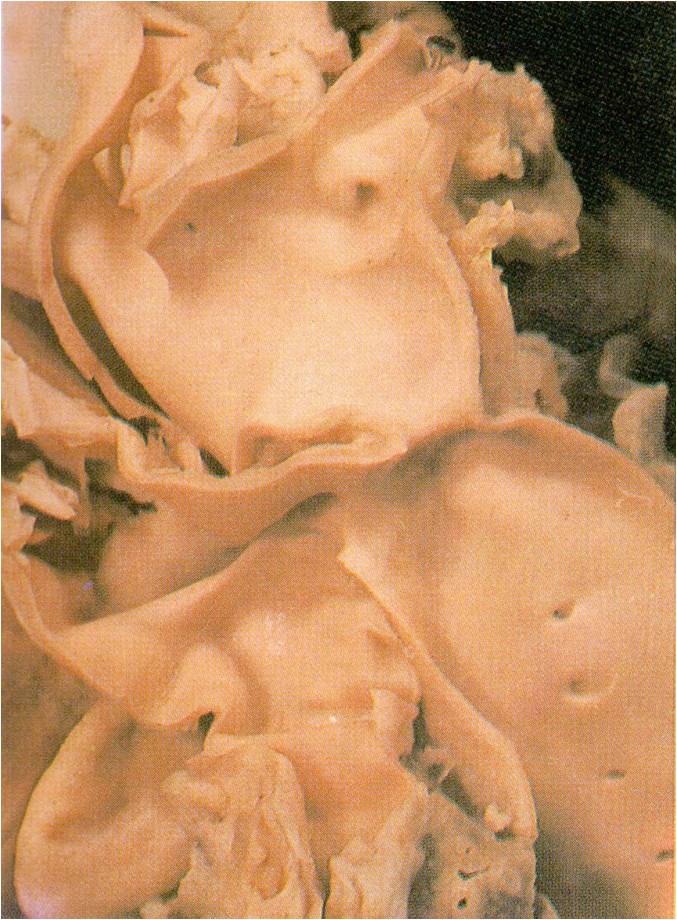
 AORTA: Coarctation, Adult: Gross, fixed tissue, an excellent illustration of postductal coarctation
AORTA: Coarctation, Adult: Gross, fixed tissue, an excellent illustration of postductal coarctation -
 AORTA: Coarctation: Gross, hypoplastic aortic arch and infantile coarctation well demonstrated.
AORTA: Coarctation: Gross, hypoplastic aortic arch and infantile coarctation well demonstrated. -
 Localized Coarctation of the aorta.
Localized Coarctation of the aorta.



Associated Conditions
- It is commonly associated with bicuspid aortic valve.
- There is 5 fold increase in the intracranial aneurysm in patient with coarctation.
Videos
{{#ev:youtube|SiNJfvK_qeI}}