Thalassemia laboratory findings: Difference between revisions
(Created page with "__NOTOC__ {{Thalassemia}} {{CMG}} ==Overview== ==Laboratory Findings== ===Peripheral Smear=== (Images shown below are courtesy of Melih Aktan MD, Istanbul Medical Faculty ...") |
|||
| (14 intermediate revisions by 6 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{Thalassemia}} | {{Thalassemia}} | ||
{{CMG}}; {{AE}}{{shyam}} {{NP}} | |||
==Overview== | |||
Laboratory findings in patients with thalassemia include anemia with [[microcytosis]], abnormal bands on hemoglobin electrophoresis, and abnormal peripheral blood smear findings. Sequencing of the globin genes will reveal mutations that lead to defective globin production. In the case of hemolysis from thalassemia, laboratory findings include elevated LDH, elevated total bilirubin, elevated indirect bilirubin, high reticulocyte count, and low haptoglobin. Importantly, the range of laboratory findings is quite diverse depending on the severity of the disease. | |||
==Laboratory Findings== | ==Laboratory Findings== | ||
===Mean corpuscular volume=== | |||
*'''[[Microcytosis]]''': [[Red blood cells]] in thalassemia have low mean corpuscular volume (MCV), typically less than 80 femtoliters. This is similar to the MCV in [[iron-deficiency anemia]].<ref name="pmid16461765">{{cite journal| author=Chui DH, Cunningham MJ, Luo HY, Wolfe LC, Neufeld EJ, Steinberg MH| title=Screening and counseling for thalassemia. | journal=Blood | year= 2006 | volume= 107 | issue= 4 | pages= 1735-7 | pmid=16461765 | doi=10.1182/blood-2005-09-3557 | pmc=1895412 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16461765 }} </ref> | |||
The accuracy of the [[mean corpuscular volume]] (MCV) < 80 fl for diagnosing thalassemia traits (defined as [[hemoglobin A2]] 4.1–9.0%) is:<ref name="pmid15916654">{{cite journal |author=Sirichotiyakul S, Maneerat J, Sa-nguansermsri T, Dhananjayanonda P, Tongsong T |title=Sensitivity and specificity of mean corpuscular volume testing for screening for alpha-thalassemia-1 and beta-thalassemia traits |journal=The journal of obstetrics and gynaecology research |volume=31 |issue=3 |pages=198–201 |year=2005 |month=June |pmid=15916654 |doi=10.1111/j.1447-0756.2005.00280.x |url=http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=1341-8076&date=2005&volume=31&issue=3&spage=198 |issn=}}</ref> | |||
* [[sensitivity (tests)|sensitivity]] = 93% | |||
* [[specificity (tests)|specificity]] = 84% | |||
===Red blood cell count === | |||
A red blood cell count > 5 suggests thalassemia<ref name="pmid2620095"/>. | |||
===Mentzer index=== | |||
The Mentzer index suggest thalassemia if less than 13 and suggests [[iron deficiency anemia]] if over 13.<ref name="pmid4123424">{{cite journal| author=Mentzer WC| title=Differentiation of iron deficiency from thalassaemia trait. | journal=Lancet | year= 1973 | volume= 1 | issue= 7808 | pages= 882 | pmid=4123424 | doi=10.1016/s0140-6736(73)91446-3 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=4123424 }} </ref><ref name="pmid17476506">{{cite journal| author=Ntaios G, Chatzinikolaou A, Saouli Z, Girtovitis F, Tsapanidou M, Kaiafa G | display-authors=etal| title=Discrimination indices as screening tests for beta-thalassemic trait. | journal=Ann Hematol | year= 2007 | volume= 86 | issue= 7 | pages= 487-91 | pmid=17476506 | doi=10.1007/s00277-007-0302-x | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17476506 }} </ref><br/> | |||
<math>\text{Mentzer index} = \frac{mean\ corpuscular\ volume}{RBC\ count}</math> | |||
===Green & King Index=== | |||
Green & King Index is:<ref name="pmid2620095">{{cite journal| author=Green R, King R| title=A new red cell discriminant incorporating volume dispersion for differentiating iron deficiency anemia from thalassemia minor. | journal=Blood Cells | year= 1989 | volume= 15 | issue= 3 | pages= 481-91; discussion 492-5 | pmid=2620095 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=2620095 }} </ref> | |||
<math>\text{Green and King Index} = MCV^2 + \frac{RDW}{Hb * 100}</math> | |||
A Green and King Index < 73 suggests thalassemia and was more sensitive than other tests in a comparison<ref name="pmid2620095"/>. | |||
MCV [2] × RDW / (Hb×100) | |||
===Hemoglobin A2=== | |||
The accuracy of an elevated [[hemoglobin A2]] at detecting abnormal DNA testing is uncertain. There are several situations in which its value will be normal:<ref name="pmid9333270">{{cite journal |author=Cao A, Saba L, Galanello R, Rosatelli MC |title=Molecular diagnosis and carrier screening for beta thalassemia |journal=JAMA |volume=278 |issue=15 |pages=1273–7 |year=1997 |month=October |pmid=9333270 |doi= |url= |issn=}}</ref> | |||
* Specific mild mutations such as the Beta+ IVS-1 nt6 mutation | |||
* In delta beta-thalassemia, creation of Hemoglobin A2 is impaired due to delta.<ref name="urlOMIM-HBD">{{cite web |url=http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=142000 |title=HEMOGLOBIN--DELTA LOCUS; HBD|author= |authorlink= |coauthors= |date= |format= |work= |publisher=Online Mendelian Inheritance in Man |pages= |language= |archiveurl= |archivedate= |quote= |accessdate=2008-11-10}}</ref> | |||
* The triple alpha globin arrangement.<ref name="urlOMIM-triple">{{cite web |url=http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=141800 |title=HEMOGLOBIN--ALPHA LOCUS 1; HBA1|author= |authorlink= |coauthors= |date= |format= |work= |publisher=Online Mendelian Inheritance in Man |pages= |language= |archiveurl= |archivedate= |quote= |accessdate=2008-11-10}}</ref> | |||
* Silent beta thalassemia, which also has [[mean corpuscular volume]]. The most common mutation for this is the -101 C to T substitution with the distal CACC box.<ref name="urlOMIM-Silent Beta">{{cite web |url=http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?cmd=entry&id=187550 |title=THALASSEMIA, BETA+, SILENT ALLELE|author= |authorlink= |coauthors= |date= |format= |work= |publisher=Online Mendelian Inheritance in Man |pages= |language= |archiveurl= |archivedate= |quote= |accessdate=2008-11-10}}</ref> | |||
===Other tests=== | |||
*'''Elevated [[red blood cell]] mass''': This is a somewhat unique feature of thalassemia. A low hemoglobin plus elevated [[red blood cell]] mass should prompt a clinician to consider thalassemia as the cause of anemia. In contrast, patients with iron deficiency anemia have low hemoglobin but do not have elevated [[red blood cell]] mass. | |||
*'''Hypochromasia''': [[Red blood cells]] in thalassemia have central pallor, similar to [[red blood cells]] in [[iron-deficiency anemia]].<ref name="pmid16461765">{{cite journal| author=Chui DH, Cunningham MJ, Luo HY, Wolfe LC, Neufeld EJ, Steinberg MH| title=Screening and counseling for thalassemia. | journal=Blood | year= 2006 | volume= 107 | issue= 4 | pages= 1735-7 | pmid=16461765 | doi=10.1182/blood-2005-09-3557 | pmc=1895412 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16461765 }} </ref> | |||
*'''Elevated [[lactate dehydrogenase]] (LDH):''' This is due to hemolysis, in which intracellular contents (such as LDH) are released into the circulation. | |||
*'''Indirect, or [[unconjugated]], [[hyperbilirubinemia]]:''' This is due to hemolysis, in which breaskdown products of heme are released into the bloodstream. | |||
*'''Low haptoglobin:''' This is due to hemolysis, in which free hemoglobin in the circulation binds to and reduces the level of haptoglobin. | |||
*'''Elevated reticulocyte count''': This is due to a bone marrow compensatory response to low hemoglobin levels from thalassemia. [[Reticulocytes]] are precursors of [[red blood cells]] and thus an elevated [[reticulocyte]] count signifies an adequate compensatory attempt to produce more [[red blood cells]]. | |||
*'''Abnormal bands on hemoglobin [[electrophoresis]]:''' Hemoglobin [[electrophoresis]] is the gold standard diagnostic test for thalassemia. In normal persons, a hemoglobin electrophoresis will show a strong band corresponding to hemoglobin A (tetramer of 2 alpha-globin chains and 2 beta-globin chains) and a weak band corresponding to hemoglobin A2 (tetramer of 2 alpha-globin chains and 2 delta-globin chains). In thalassemia, various other bands can be present on [[electrophoresis]]. These include tetramers of gamma-globin chains (such as in Hb Barts) or tetramers of beta-globin chains (such as in HbH disease). | |||
*''' Abnormal cells on peripheral blood smear''': The peripheral blood smear is perhaps the most inexpensive laboratory test that can accurately lead to a diagnosis of thalassemia. Patients with thalassemia have target cells and hypochromic (low color) and microcytic (small-sized) [[red blood cells]]. | |||
*'''Mutations in alpha-globin on DNA [[sequencing]]''': This is a specialized test that can definitively determine the presence of alpha-thalassemia. Sequencing of the alpha-globin chain from peripheral blood cells can help diagnose alpha-thalassemia. This laboratory test is more expensive than the other tests. These laboratory findings are pathognomonic for alpha-thalassemia. Deletions or insertions are more common in the alpha-globin gene compared to the beta-globin gene. | |||
*'''Mutations in beta-globin on DNA sequencing''': This is a specialized test that can definitively determine the presence of beta-thalassemia. Sequencing of the beta-globin chain from peripheral blood cells can help diagnose beta-thalassemia. This laboratory test is more expensive than the other tests. These laboratory findings are pathognomonic for beta-thalassemia. Point mutations (substitutions) are more common in the beta-globin gene compared to the alpha-globin gene. | |||
===Peripheral Smear=== | ===Peripheral Smear=== | ||
(Images shown below are courtesy of Melih Aktan MD, Istanbul Medical Faculty - Turkey, and Kyoto University - Japan, and Hospital Universitario La Fe Servicio Hematologia) | (Images shown below are courtesy of Melih Aktan MD, Istanbul Medical Faculty - Turkey, and Kyoto University - Japan, and Hospital Universitario La Fe Servicio Hematologia) | ||
<div align="left"> | <div align="left"> | ||
| Line 27: | Line 75: | ||
{{Reflist|2}} | {{Reflist|2}} | ||
[[Category:Hematology]] | |||
{{WH}} | {{WH}} | ||
{{WS}} | {{WS}} | ||
Latest revision as of 23:05, 13 July 2022
|
Thalassemia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Thalassemia laboratory findings On the Web |
|
American Roentgen Ray Society Images of Thalassemia laboratory findings |
|
Risk calculators and risk factors for Thalassemia laboratory findings |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Shyam Patel [2] Neel Patel, M.B.B.S[3]
Overview
Laboratory findings in patients with thalassemia include anemia with microcytosis, abnormal bands on hemoglobin electrophoresis, and abnormal peripheral blood smear findings. Sequencing of the globin genes will reveal mutations that lead to defective globin production. In the case of hemolysis from thalassemia, laboratory findings include elevated LDH, elevated total bilirubin, elevated indirect bilirubin, high reticulocyte count, and low haptoglobin. Importantly, the range of laboratory findings is quite diverse depending on the severity of the disease.
Laboratory Findings
Mean corpuscular volume
- Microcytosis: Red blood cells in thalassemia have low mean corpuscular volume (MCV), typically less than 80 femtoliters. This is similar to the MCV in iron-deficiency anemia.[1]
The accuracy of the mean corpuscular volume (MCV) < 80 fl for diagnosing thalassemia traits (defined as hemoglobin A2 4.1–9.0%) is:[2]
- sensitivity = 93%
- specificity = 84%
Red blood cell count
A red blood cell count > 5 suggests thalassemia[3].
Mentzer index
The Mentzer index suggest thalassemia if less than 13 and suggests iron deficiency anemia if over 13.[4][5]
<math>\text{Mentzer index} = \frac{mean\ corpuscular\ volume}{RBC\ count}</math>
Green & King Index
Green & King Index is:[3]
<math>\text{Green and King Index} = MCV^2 + \frac{RDW}{Hb * 100}</math>
A Green and King Index < 73 suggests thalassemia and was more sensitive than other tests in a comparison[3].
MCV [2] × RDW / (Hb×100)
Hemoglobin A2
The accuracy of an elevated hemoglobin A2 at detecting abnormal DNA testing is uncertain. There are several situations in which its value will be normal:[6]
- Specific mild mutations such as the Beta+ IVS-1 nt6 mutation
- In delta beta-thalassemia, creation of Hemoglobin A2 is impaired due to delta.[7]
- The triple alpha globin arrangement.[8]
- Silent beta thalassemia, which also has mean corpuscular volume. The most common mutation for this is the -101 C to T substitution with the distal CACC box.[9]
Other tests
- Elevated red blood cell mass: This is a somewhat unique feature of thalassemia. A low hemoglobin plus elevated red blood cell mass should prompt a clinician to consider thalassemia as the cause of anemia. In contrast, patients with iron deficiency anemia have low hemoglobin but do not have elevated red blood cell mass.
- Hypochromasia: Red blood cells in thalassemia have central pallor, similar to red blood cells in iron-deficiency anemia.[1]
- Elevated lactate dehydrogenase (LDH): This is due to hemolysis, in which intracellular contents (such as LDH) are released into the circulation.
- Indirect, or unconjugated, hyperbilirubinemia: This is due to hemolysis, in which breaskdown products of heme are released into the bloodstream.
- Low haptoglobin: This is due to hemolysis, in which free hemoglobin in the circulation binds to and reduces the level of haptoglobin.
- Elevated reticulocyte count: This is due to a bone marrow compensatory response to low hemoglobin levels from thalassemia. Reticulocytes are precursors of red blood cells and thus an elevated reticulocyte count signifies an adequate compensatory attempt to produce more red blood cells.
- Abnormal bands on hemoglobin electrophoresis: Hemoglobin electrophoresis is the gold standard diagnostic test for thalassemia. In normal persons, a hemoglobin electrophoresis will show a strong band corresponding to hemoglobin A (tetramer of 2 alpha-globin chains and 2 beta-globin chains) and a weak band corresponding to hemoglobin A2 (tetramer of 2 alpha-globin chains and 2 delta-globin chains). In thalassemia, various other bands can be present on electrophoresis. These include tetramers of gamma-globin chains (such as in Hb Barts) or tetramers of beta-globin chains (such as in HbH disease).
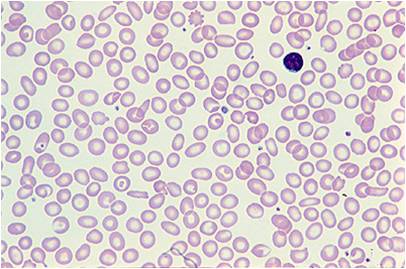
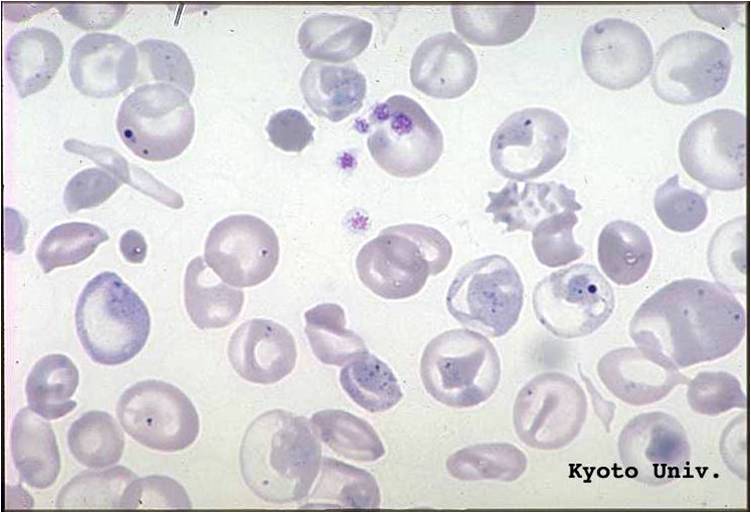
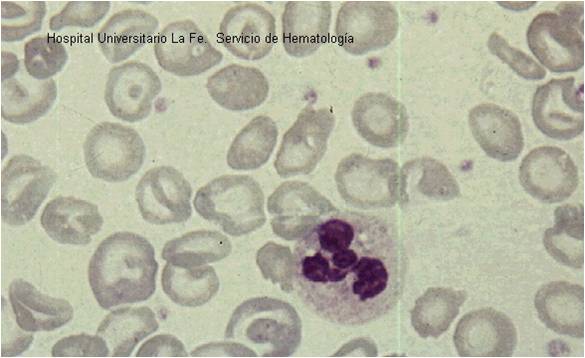
- Abnormal cells on peripheral blood smear: The peripheral blood smear is perhaps the most inexpensive laboratory test that can accurately lead to a diagnosis of thalassemia. Patients with thalassemia have target cells and hypochromic (low color) and microcytic (small-sized) red blood cells.
- Mutations in alpha-globin on DNA sequencing: This is a specialized test that can definitively determine the presence of alpha-thalassemia. Sequencing of the alpha-globin chain from peripheral blood cells can help diagnose alpha-thalassemia. This laboratory test is more expensive than the other tests. These laboratory findings are pathognomonic for alpha-thalassemia. Deletions or insertions are more common in the alpha-globin gene compared to the beta-globin gene.
- Mutations in beta-globin on DNA sequencing: This is a specialized test that can definitively determine the presence of beta-thalassemia. Sequencing of the beta-globin chain from peripheral blood cells can help diagnose beta-thalassemia. This laboratory test is more expensive than the other tests. These laboratory findings are pathognomonic for beta-thalassemia. Point mutations (substitutions) are more common in the beta-globin gene compared to the alpha-globin gene.
Peripheral Smear
(Images shown below are courtesy of Melih Aktan MD, Istanbul Medical Faculty - Turkey, and Kyoto University - Japan, and Hospital Universitario La Fe Servicio Hematologia)
-

Thalassemia
-
Thalassemia


-
Thalassemia
-
Thalassemia


References
- ↑ 1.0 1.1 Chui DH, Cunningham MJ, Luo HY, Wolfe LC, Neufeld EJ, Steinberg MH (2006). "Screening and counseling for thalassemia". Blood. 107 (4): 1735–7. doi:10.1182/blood-2005-09-3557. PMC 1895412. PMID 16461765.
- ↑ Sirichotiyakul S, Maneerat J, Sa-nguansermsri T, Dhananjayanonda P, Tongsong T (2005). "Sensitivity and specificity of mean corpuscular volume testing for screening for alpha-thalassemia-1 and beta-thalassemia traits". The journal of obstetrics and gynaecology research. 31 (3): 198–201. doi:10.1111/j.1447-0756.2005.00280.x. PMID 15916654. Unknown parameter
|month=ignored (help) - ↑ 3.0 3.1 3.2 Green R, King R (1989). "A new red cell discriminant incorporating volume dispersion for differentiating iron deficiency anemia from thalassemia minor". Blood Cells. 15 (3): 481–91, discussion 492-5. PMID 2620095.
- ↑ Mentzer WC (1973). "Differentiation of iron deficiency from thalassaemia trait". Lancet. 1 (7808): 882. doi:10.1016/s0140-6736(73)91446-3. PMID 4123424.
- ↑ Ntaios G, Chatzinikolaou A, Saouli Z, Girtovitis F, Tsapanidou M, Kaiafa G; et al. (2007). "Discrimination indices as screening tests for beta-thalassemic trait". Ann Hematol. 86 (7): 487–91. doi:10.1007/s00277-007-0302-x. PMID 17476506.
- ↑ Cao A, Saba L, Galanello R, Rosatelli MC (1997). "Molecular diagnosis and carrier screening for beta thalassemia". JAMA. 278 (15): 1273–7. PMID 9333270. Unknown parameter
|month=ignored (help) - ↑ "HEMOGLOBIN--DELTA LOCUS; HBD". Online Mendelian Inheritance in Man. Retrieved 2008-11-10.
- ↑ "HEMOGLOBIN--ALPHA LOCUS 1; HBA1". Online Mendelian Inheritance in Man. Retrieved 2008-11-10.
- ↑ "THALASSEMIA, BETA+, SILENT ALLELE". Online Mendelian Inheritance in Man. Retrieved 2008-11-10.