ST Elevation Myocardial Infarction in a Rare Variant of Single Coronary Anomaly: Difference between revisions
Tarek Nafee (talk | contribs) |
Tarek Nafee (talk | contribs) No edit summary |
||
| (31 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
< | <small>'''[[Tweetbook: Interventional Cardiology Cases|Click here]] to go back to the Tweetbook'''<br> | ||
'''[[Anomalous origins of coronary arteries|Click here]] to read more about anomalous origins of coronary arteries on WikiDoc'''</small> | |||
==Authors== | ==Authors== | ||
'''Bhalaghuru Chokkalingam Mani, MD; Alec Vishnevsky, MD; Ethan J. Halperin, MD; David L. Fischman, MD''' | '''Bhalaghuru Chokkalingam Mani, MD<sup>1</sup>; Alec Vishnevsky, MD<sup>2</sup>; Ethan J. Halperin, MD<sup>2</sup>; David L. Fischman, MD<sup>2</sup>''' | ||
<br><small><small>''<sup>1</sup>From Novant Heart and Vascular Institute, Matthews, NC; <sup>2</sup>From the Department of Medicine, Division of Cardiology, Sidney Kimmel Medical College at Thomas Jefferson University, Thomas Jefferson University Hospital, Philadelphia, PA''</small></small> | |||
==Case== | ==Case== | ||
A 53 year-old woman with a history of hypertension, dyslipidemia, diabetes, and tobacco use presented to the emergency room with the sudden onset of chest pain. An electrocardiogram (Figure 1) revealed an inferior ST elevation myocardial infarction and the patient was referred for emergent cardiac catheterization. An initial attempt to engage the left coronary artery was unsuccessful. Nonselective injection of the left coronary sinus failed to identify a coronary ostia ( | A 53 year-old woman with a history of hypertension, dyslipidemia, diabetes, and tobacco use presented to the emergency room with the sudden onset of chest pain. An electrocardiogram '''(Figure 1)''' revealed an inferior ST elevation myocardial infarction and the patient was referred for emergent cardiac catheterization. An initial attempt to engage the left coronary artery was unsuccessful. Nonselective injection of the left coronary sinus failed to identify a coronary ostia '''(Figure 2)'''. Selective angiography of the right coronary artery (RCA) revealed a single coronary trunk that gave rise to separate origins of the major coronary arteries. The left circumflex artery (LCx) reached the left atrioventricular groove by coursing anterior to the pulmonary artery. The left anterior descending artery (LAD) courses posterior to the right ventricular outflow tract (RVOT) and then intraseptally to emerge in the anterior interventricular groove. An acute RV marginal branch also wraps anterior to the pulmonary artery and then courses toward the cardiac apex parallel to the LAD just to the right of the interventricular groove. The right coronary artery was occluded beyond the origin of these vessels '''(Figures 3,4)''' and was successfully stented '''(Figure 5,6)'''. Multislice coronary computed tomography angiography confirmed the anatomical variant and the course of the vessels '''(Figures 7,8)'''. | ||
==Figures== | ==Figures== | ||
<gallery heights="175" widths="175"> | |||
File:10001 1.jpg|Figure 1. 12-lead electrocardiogram revealing inferior ST-elevation | |||
File:10001 2.jpg|'''Figure 2.''' Right anterior oblique cineangiography of non-selective injection of the left coronary sinus | |||
File:10001 3.jpg|'''Figure 3.''' Left anterior oblique cineangiography of selective coronary injection of the right coronary (RCA). LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery) | |||
File:10001 4.jpg|'''Figure 4.''' Right anterior oblique cineangiography of selective coronary injection of the right coronary artery (RCA). LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery) | |||
File:10001 5.jpg|'''Figure 5.''' Left anterior oblique cineangiography of the right coronary artery (RCA) following coronary stenting of the mid-vessel occlusion. LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery) | |||
File:10001 6.jpg|'''Figure 6.''' Right anterior oblique cineangiography of the right coronary artery (RCA) following coronary stenting. LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery) | |||
File:10001 7.jpg|'''Figure 7.''' Three dimensional reconstruction cardiac computed tomography image of the coronary arterial tree showing a single coronary ostium in the right anterior oblique projection with the left anterior descending artery emerging out of the septum into the anterior interventricular groove, and the acute marginal and circumflex arteries coursing anterior to the right ventricular outflow tract. RCA (right coronary artery); LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery); RVOT (right ventricular outflow tract) | |||
File:10001 8.jpg|'''Figure 8.''' Maximum intensity slab computed tomography image demonstrating the origins of the right coronary artery, left anterior descending artery, acute marginal and circumflex artery, all from a single trunk emerging from the right sinus of Valsalva. RCA (right coronary artery); LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery); RVOT (right ventricular outflow tract) | |||
</gallery> | |||
==Comments== | ==Comments== | ||
Single coronary arteries are among the rarest of coronary artery anomalies with a reported incidence of 0.06-0.024%. | Single coronary arteries are among the rarest of coronary artery anomalies with a reported incidence of 0.06-0.024%.<ref name="pmid1289093">{{cite journal| author=Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J et al.| title=Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. | journal=Eur Heart J | year= 1992 | volume= 13 | issue= 12 | pages= 1637-40 | pmid=1289093 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1289093 }} </ref> Classification schemes have been developed based on the vessel course and their relationship to the great vessels.<ref name="pmid758666">{{cite journal| author=Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L| title=Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. | journal=Radiology | year= 1979 | volume= 130 | issue= 1 | pages= 39-47 | pmid=758666 | doi=10.1148/130.1.39 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=758666 }} </ref><ref name="pmid2208265">{{cite journal| author=Yamanaka O, Hobbs RE| title=Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. | journal=Cathet Cardiovasc Diagn | year= 1990 | volume= 21 | issue= 1 | pages= 28-40 | pmid=2208265 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=2208265 }} </ref> Our patient’s anatomy is a Yamanaka R-III C (R-III combined) variant wherein the left coronary arteries have separate ostia arising from the RCA and have a combination of courses including an anterior and intraseptal course. ST elevation myocardial infarction in this setting is extremely rare.<ref name="pmid24765348">{{cite journal| author=Marchesini J, Campo G, Righi R, Benea G, Ferrari R| title=Coronary artery anomalies presenting with ST-segment elevation myocardial infarction. | journal=Clin Pract | year= 2011 | volume= 1 | issue= 4 | pages= e107 | pmid=24765348 | doi=10.4081/cp.2011.e107 | pmc=3981407 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=24765348 }} </ref> Interventional cardiologists should be aware of such scenarios in order to accurately identify the coronary anatomy and provide timely treatment. | ||
from the RCA and have a combination of courses including an anterior and intraseptal course. ST elevation myocardial infarction in this setting is extremely rare.4 | |||
==References== | ==References== | ||
{{Reflist|2}} | |||
{{WS}}{{WH}} | |||
{{ | [[Category:Tweetbook]] | ||
[[Category:Cardiology]] | |||
Latest revision as of 14:11, 5 July 2018
Click here to go back to the Tweetbook
Click here to read more about anomalous origins of coronary arteries on WikiDoc
Authors
Bhalaghuru Chokkalingam Mani, MD1; Alec Vishnevsky, MD2; Ethan J. Halperin, MD2; David L. Fischman, MD2
1From Novant Heart and Vascular Institute, Matthews, NC; 2From the Department of Medicine, Division of Cardiology, Sidney Kimmel Medical College at Thomas Jefferson University, Thomas Jefferson University Hospital, Philadelphia, PA
Case
A 53 year-old woman with a history of hypertension, dyslipidemia, diabetes, and tobacco use presented to the emergency room with the sudden onset of chest pain. An electrocardiogram (Figure 1) revealed an inferior ST elevation myocardial infarction and the patient was referred for emergent cardiac catheterization. An initial attempt to engage the left coronary artery was unsuccessful. Nonselective injection of the left coronary sinus failed to identify a coronary ostia (Figure 2). Selective angiography of the right coronary artery (RCA) revealed a single coronary trunk that gave rise to separate origins of the major coronary arteries. The left circumflex artery (LCx) reached the left atrioventricular groove by coursing anterior to the pulmonary artery. The left anterior descending artery (LAD) courses posterior to the right ventricular outflow tract (RVOT) and then intraseptally to emerge in the anterior interventricular groove. An acute RV marginal branch also wraps anterior to the pulmonary artery and then courses toward the cardiac apex parallel to the LAD just to the right of the interventricular groove. The right coronary artery was occluded beyond the origin of these vessels (Figures 3,4) and was successfully stented (Figure 5,6). Multislice coronary computed tomography angiography confirmed the anatomical variant and the course of the vessels (Figures 7,8).
Figures
-
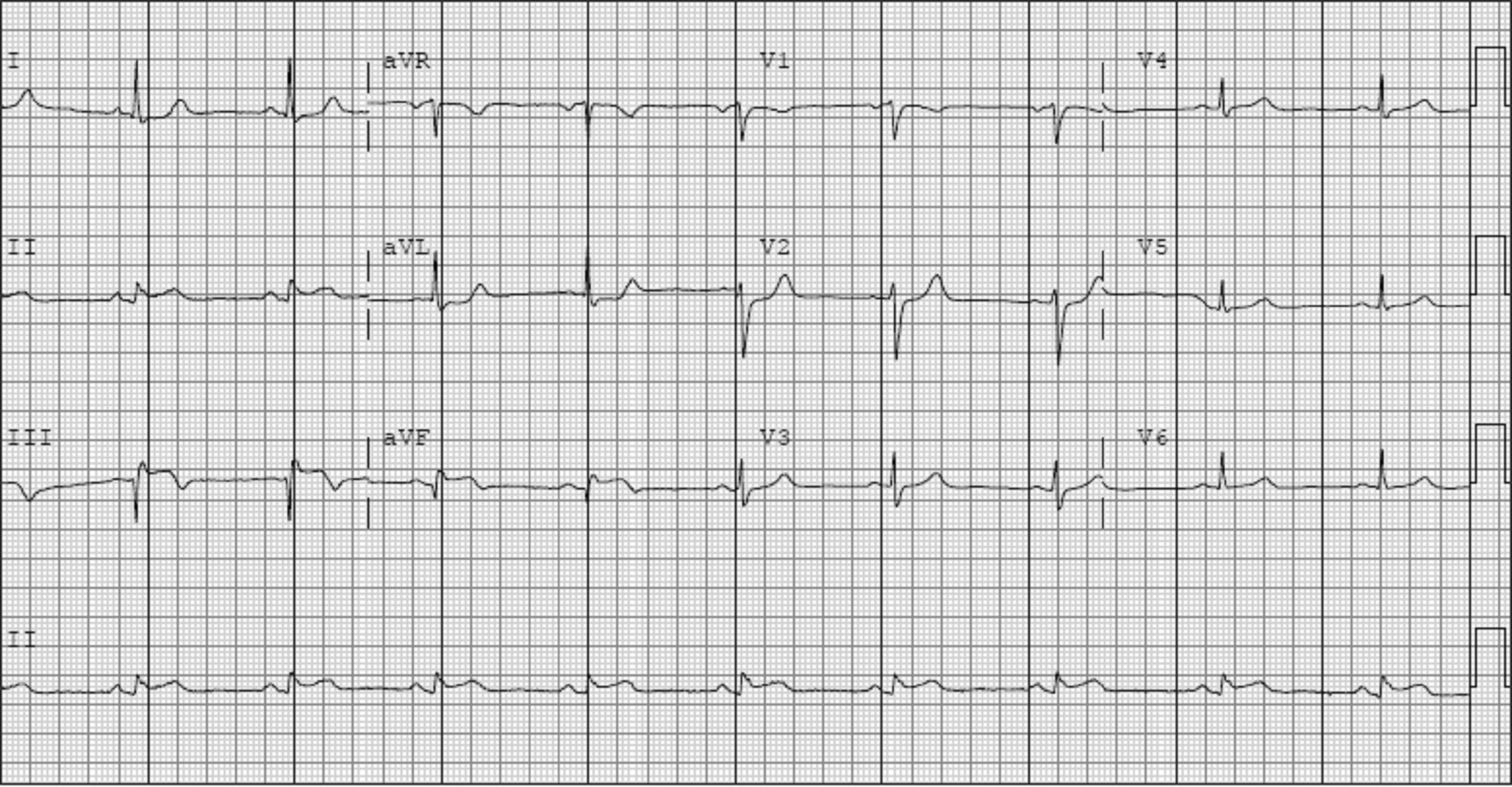
Figure 1. 12-lead electrocardiogram revealing inferior ST-elevation
-
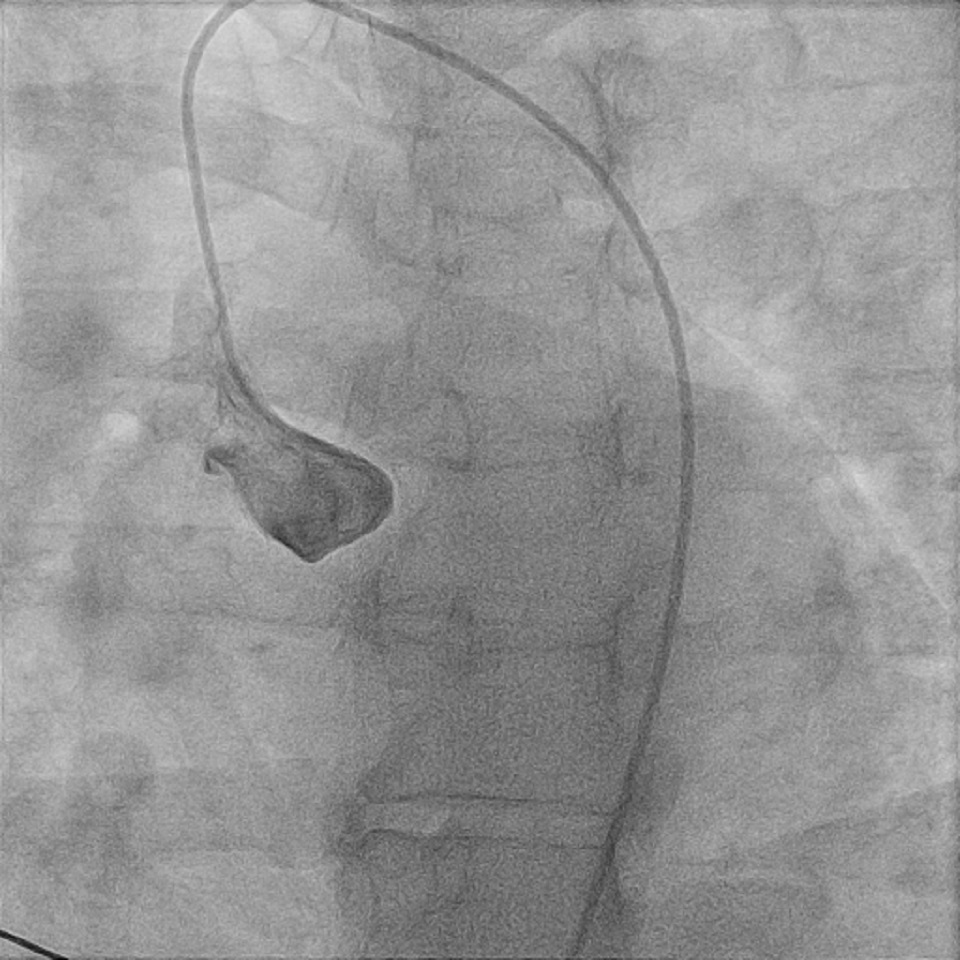
Figure 2. Right anterior oblique cineangiography of non-selective injection of the left coronary sinus
-
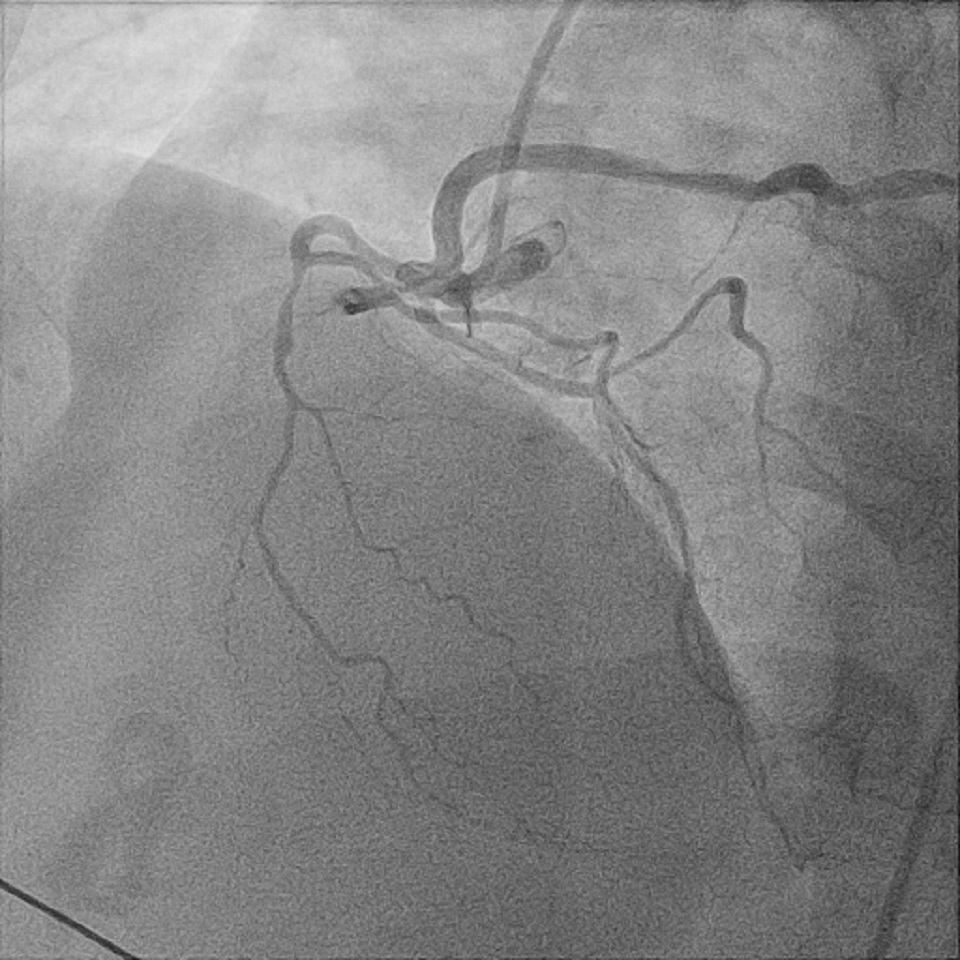
Figure 3. Left anterior oblique cineangiography of selective coronary injection of the right coronary (RCA). LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery)
-
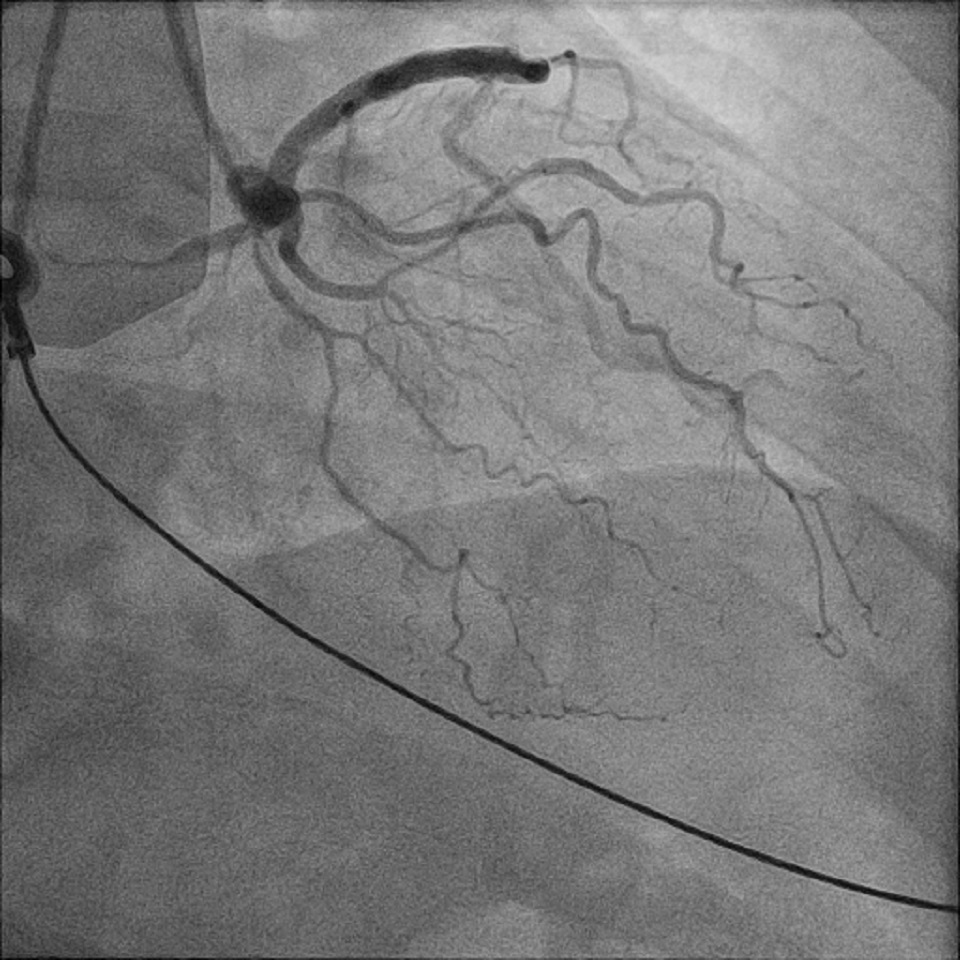
Figure 4. Right anterior oblique cineangiography of selective coronary injection of the right coronary artery (RCA). LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery)
-
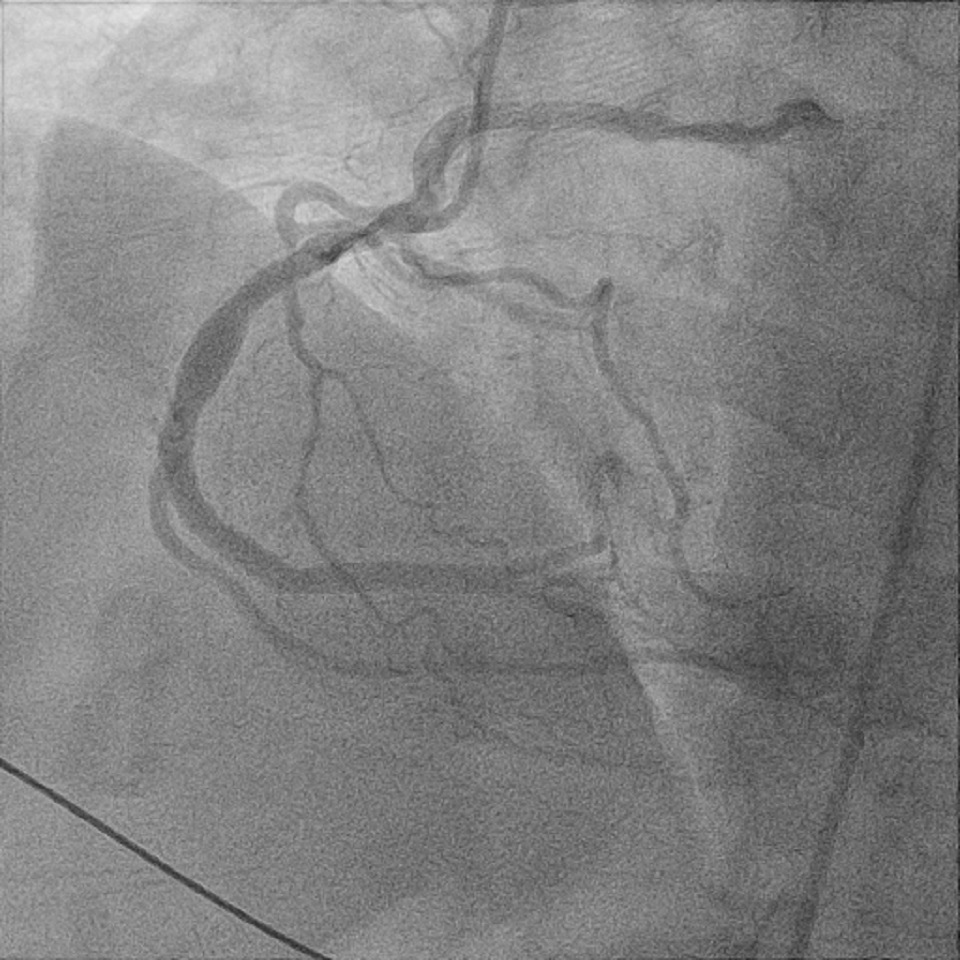
Figure 5. Left anterior oblique cineangiography of the right coronary artery (RCA) following coronary stenting of the mid-vessel occlusion. LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery)
-
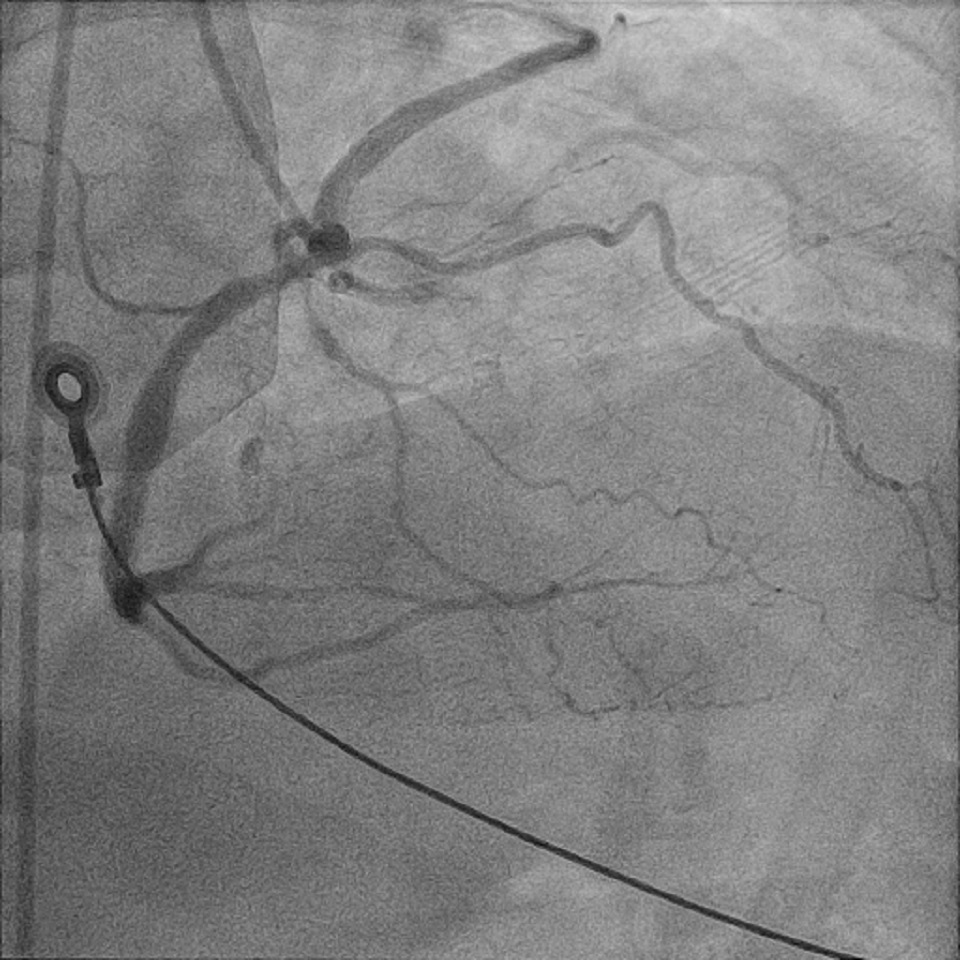
Figure 6. Right anterior oblique cineangiography of the right coronary artery (RCA) following coronary stenting. LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery)
-

Figure 7. Three dimensional reconstruction cardiac computed tomography image of the coronary arterial tree showing a single coronary ostium in the right anterior oblique projection with the left anterior descending artery emerging out of the septum into the anterior interventricular groove, and the acute marginal and circumflex arteries coursing anterior to the right ventricular outflow tract. RCA (right coronary artery); LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery); RVOT (right ventricular outflow tract)
-

Figure 8. Maximum intensity slab computed tomography image demonstrating the origins of the right coronary artery, left anterior descending artery, acute marginal and circumflex artery, all from a single trunk emerging from the right sinus of Valsalva. RCA (right coronary artery); LCx (left circumflex coronary artery); LAD (left anterior descending coronary artery); RVOT (right ventricular outflow tract)








Comments
Single coronary arteries are among the rarest of coronary artery anomalies with a reported incidence of 0.06-0.024%.[1] Classification schemes have been developed based on the vessel course and their relationship to the great vessels.[2][3] Our patient’s anatomy is a Yamanaka R-III C (R-III combined) variant wherein the left coronary arteries have separate ostia arising from the RCA and have a combination of courses including an anterior and intraseptal course. ST elevation myocardial infarction in this setting is extremely rare.[4] Interventional cardiologists should be aware of such scenarios in order to accurately identify the coronary anatomy and provide timely treatment.
References
- ↑ Desmet W, Vanhaecke J, Vrolix M, Van de Werf F, Piessens J, Willems J; et al. (1992). "Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies". Eur Heart J. 13 (12): 1637–40. PMID 1289093.
- ↑ Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L (1979). "Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance". Radiology. 130 (1): 39–47. doi:10.1148/130.1.39. PMID 758666.
- ↑ Yamanaka O, Hobbs RE (1990). "Coronary artery anomalies in 126,595 patients undergoing coronary arteriography". Cathet Cardiovasc Diagn. 21 (1): 28–40. PMID 2208265.
- ↑ Marchesini J, Campo G, Righi R, Benea G, Ferrari R (2011). "Coronary artery anomalies presenting with ST-segment elevation myocardial infarction". Clin Pract. 1 (4): e107. doi:10.4081/cp.2011.e107. PMC 3981407. PMID 24765348.