Delayed puberty MRI: Difference between revisions
No edit summary |
No edit summary |
||
| Line 3: | Line 3: | ||
{{CMG}}; {{AE}}{{EG}} | {{CMG}}; {{AE}}{{EG}} | ||
{| align="right" | {| align="right" | ||
| {{#ev:youtube|N7x5a4WCymE}} | |||
|-| | |||
| [[image:Webp.net-gifmaker (35).gif|thumb|500px|Absent right olfactory bulb - Case courtesy of Dr Joseph Scheller, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/54233">rID: 54233</a>]] | | [[image:Webp.net-gifmaker (35).gif|thumb|500px|Absent right olfactory bulb - Case courtesy of Dr Joseph Scheller, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/54233">rID: 54233</a>]] | ||
|} | |} | ||
==Overview== | |||
[[Brain]] [[MRI]] may be helpful in the diagnosis of delayed [[puberty]]. Findings on [[MRI]] suggestive of delayed [[puberty]] include [[Hypothalamus|hypothalamo]]-[[pituitary]] lesions, [[aplasia]] of [[olfactory bulb]] and/or [[Sulci (anatomy)|sulci]] ([[Kallmann syndrome]]), [[optic nerve]] compression ([[pituitary adenoma]]), and [[inner ear]] abnormalities ([[CHARGE syndrome]]). Showing the [[aplasia]] of [[olfactory bulbs]] and/or [[Sulci (anatomy)|sulci]] in [[MRI]], it is assumed as differentiation of [[Kallmann syndrome]] from isolated [[hypogonadotropic hypogonadism]], in patient without smelling problems or hard to evaluate. | |||
==MRI== | ==MRI== | ||
* [[Brain]] [[MRI]] may be helpful in the diagnosis of delayed [[puberty]]. Findings on [[MRI]] suggestive of delayed [[puberty]] include:<ref name="pmid26194704">{{cite journal |vauthors=Boehm U, Bouloux PM, Dattani MT, de Roux N, Dodé C, Dunkel L, Dwyer AA, Giacobini P, Hardelin JP, Juul A, Maghnie M, Pitteloud N, Prevot V, Raivio T, Tena-Sempere M, Quinton R, Young J |title=Expert consensus document: European Consensus Statement on congenital hypogonadotropic hypogonadism--pathogenesis, diagnosis and treatment |journal=Nat Rev Endocrinol |volume=11 |issue=9 |pages=547–64 |year=2015 |pmid=26194704 |doi=10.1038/nrendo.2015.112 |url=}}</ref> | * [[Brain]] [[MRI]] may be helpful in the diagnosis of delayed [[puberty]]. Findings on [[MRI]] suggestive of delayed [[puberty]] include:<ref name="pmid26194704">{{cite journal |vauthors=Boehm U, Bouloux PM, Dattani MT, de Roux N, Dodé C, Dunkel L, Dwyer AA, Giacobini P, Hardelin JP, Juul A, Maghnie M, Pitteloud N, Prevot V, Raivio T, Tena-Sempere M, Quinton R, Young J |title=Expert consensus document: European Consensus Statement on congenital hypogonadotropic hypogonadism--pathogenesis, diagnosis and treatment |journal=Nat Rev Endocrinol |volume=11 |issue=9 |pages=547–64 |year=2015 |pmid=26194704 |doi=10.1038/nrendo.2015.112 |url=}}</ref> | ||
Revision as of 17:26, 11 September 2017
|
Delayed puberty Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Delayed puberty MRI On the Web |
|
American Roentgen Ray Society Images of Delayed puberty MRI |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Eiman Ghaffarpasand, M.D. [2]
| N7x5a4WCymE}} |
.gif) |
Overview
Brain MRI may be helpful in the diagnosis of delayed puberty. Findings on MRI suggestive of delayed puberty include hypothalamo-pituitary lesions, aplasia of olfactory bulb and/or sulci (Kallmann syndrome), optic nerve compression (pituitary adenoma), and inner ear abnormalities (CHARGE syndrome). Showing the aplasia of olfactory bulbs and/or sulci in MRI, it is assumed as differentiation of Kallmann syndrome from isolated hypogonadotropic hypogonadism, in patient without smelling problems or hard to evaluate.
MRI
- Brain MRI may be helpful in the diagnosis of delayed puberty. Findings on MRI suggestive of delayed puberty include:[1]
- Hypothalamo-pituitary lesions
- Aplasia of olfactory bulb and/or sulci (Kallmann syndrome)
- Optic nerve compression (pituitary adenoma)
- Inner ear abnormalities (CHARGE syndrome)
- Brain MRI is indicated in patients with delayed puberty, experiencing some alarm signs, such as headache, visual impairment, and behavioral changes.
- Showing the aplasia of olfactory bulbs and/or sulci in MRI, it is assumed as differentiation of Kallmann syndrome from isolated hypogonadotropic hypogonadism, in patient without smelling problems or hard to evaluate.[2]
- A moderate agreement is seen between the smell identification test (UPSIT) and presence of the olfactory bulbs in MRI, in patients with hypogonadotropic hypogonadism. While, there is a good agreement between them in absence of the olfactory bulbs in MRI and anosmia.[3][2]
-
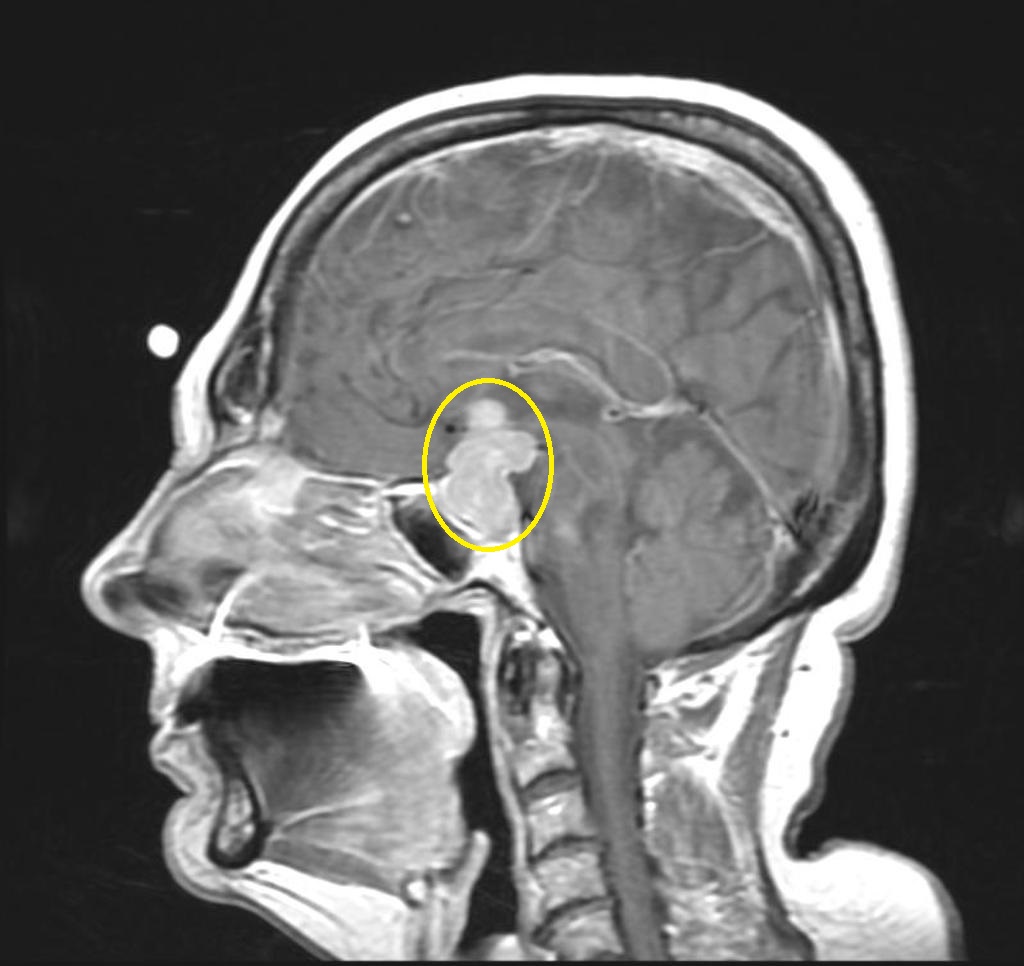
Pituitary adenoma - Case courtesy of A.Prof Frank Gaillard, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/16890">rID: 16890</a>
-
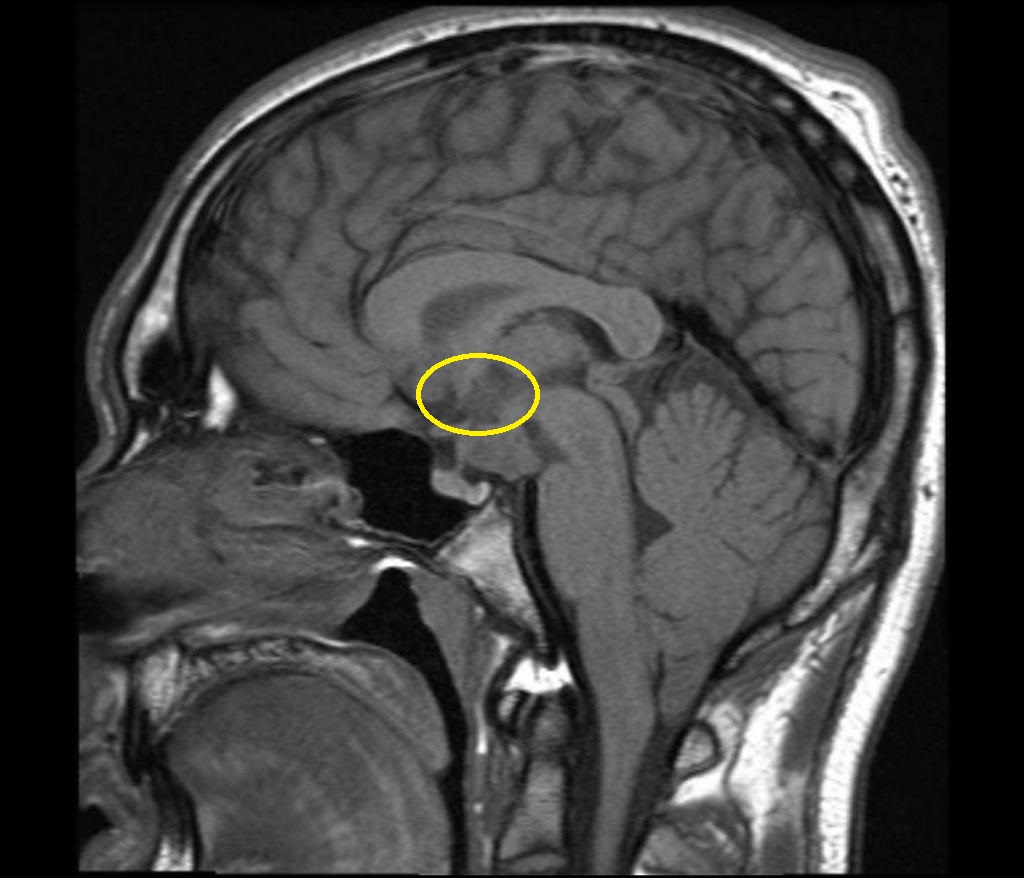
Hypothalamic lesion - Case courtesy of A.Prof Frank Gaillard, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/16890">rID: 16890</a>
-
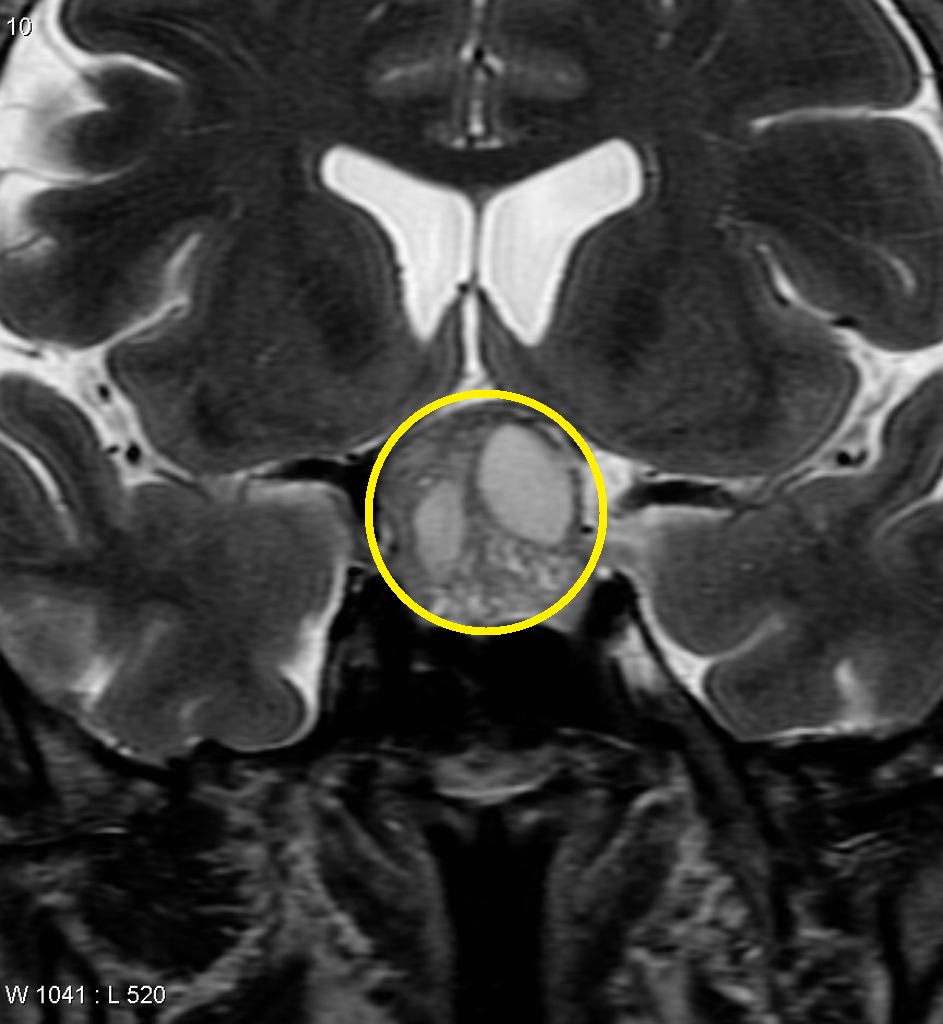
Pituitary non-functioning macroadenoma - Case courtesy of A.Prof Frank Gaillard, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/5562">rID: 5562</a>
-
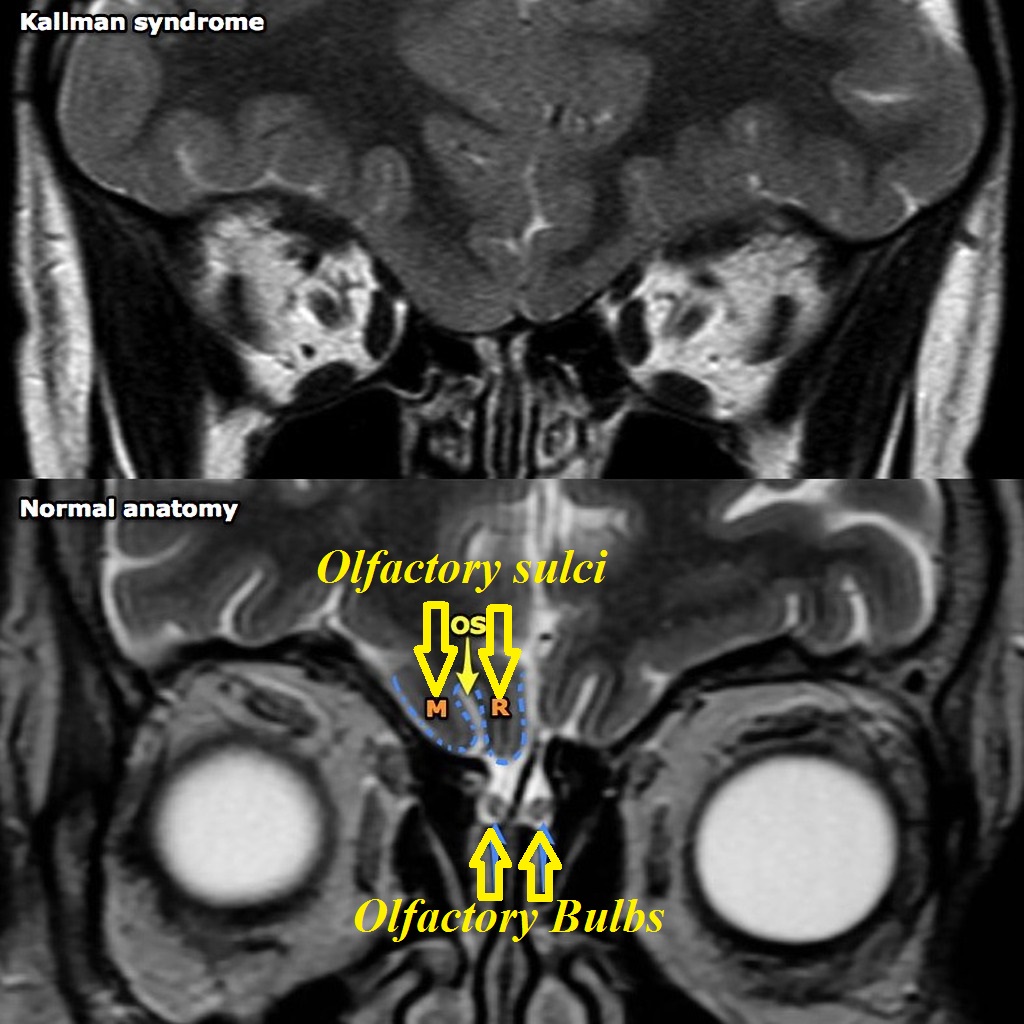
Kallman syndrome difference with normal brain - Case courtesy of A.Prof Frank Gaillard, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/6083">rID: 6083</a>


.jpg)

References
- ↑ Boehm U, Bouloux PM, Dattani MT, de Roux N, Dodé C, Dunkel L, Dwyer AA, Giacobini P, Hardelin JP, Juul A, Maghnie M, Pitteloud N, Prevot V, Raivio T, Tena-Sempere M, Quinton R, Young J (2015). "Expert consensus document: European Consensus Statement on congenital hypogonadotropic hypogonadism--pathogenesis, diagnosis and treatment". Nat Rev Endocrinol. 11 (9): 547–64. doi:10.1038/nrendo.2015.112. PMID 26194704.
- ↑ 2.0 2.1 Palmert, Mark R.; Dunkel, Leo (2012). "Delayed Puberty". New England Journal of Medicine. 366 (5): 443–453. doi:10.1056/NEJMcp1109290. ISSN 0028-4793.
- ↑ Doty RL, Shaman P, Kimmelman CP, Dann MS (1984). "University of Pennsylvania Smell Identification Test: a rapid quantitative olfactory function test for the clinic". Laryngoscope. 94 (2 Pt 1): 176–8. PMID 6694486.