Parietal lobe

Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
The parietal lobe is a lobe in the brain. It is positioned above (superior to) the occipital lobe and behind (posterior to) the frontal lobe.
The parietal lobe integrates sensory information from different modalities, particularly determining spatial sense and navigation. For example, it comprises somatosensory cortex and the dorsal stream of the visual system. This enables regions of the parietal cortex to map objects perceived visually into body coordinate positions.
Anatomy
The parietal lobe is defined by four anatomical boundaries: the central sulcus separates the parietal lobe from the frontal lobe; the parieto-occipital sulcus separates the parietal and occipital lobe; the lateral sulcus (sylvian fissure) is the most lateral boundary separating it from the temporal lobe; and the medial longitudinal fissure divides the two hemispheres.
Immediately posterior to the central sulcus, and the most anterior part of the parietal lobe, is the postcentral gyrus (Brodmann area 3), the primary somatosensory cortical area. Dividing this and the posterior parietal cortex is the postcentral sulcus.
The posterior parietal cortex can be subdivided into the superior parietal lobule (Brodmann areas 5 + 7) and the inferior parietal lobule (39 + 40), separated by the intraparietal sulcus (IP). The intraparietal sulcus and adjacent gyri are essential in guidance of limb and eye movement, and based on cytoarchitectural and functional differences is further divided into medial (MIP), lateral (LIP), ventral (VIP), and anterior (AIP) areas.
Function
The parietal lobe plays important roles in integrating sensory information from various parts of the body, knowledge of numbers and their relations[1], and in the manipulation of objects. Portions of the parietal lobe are involved with visuospatial processing. Much less is known about this lobe than the other three in the cerebrum.
Various studies in the 1990s found that different regions of the parietal cortex in Macaques represent different parts of space.
- The lateral intraparietal (LIP) contains a 2-dimensional topographic map of retinotopically-coded space representing the saliency of spatial locations. It can be used by the oculomotor system for targeting eye movements, when appropriate.
- The ventral intraparietal (VIP) area receives input from a number of senses (visual, somatosensory, auditory, and vestibular[2]). Neurons with tactile receptive fields represented space in a head-centered reference frame[2]. The cells with visual receptive fields also fire with head-centered reference frames[3] but possibly also with eye-centered coordinates[2]
- The medial intraparietal (MIP) area neurons encode the location of a reach target in eye-centered coordinates.[4]
- The anterior intraparietal (AIP) area contains neurons responsive to shape, size, and orientation of objects to be grasped[5] as well as for manipulation of hands themselves, both to viewed[5] and remembered stimuli. [6]
Pathology
Gerstmann's syndrome is associated with lesion to the dominant (usually left) parietal lobe. Balint's syndrome is associated with bilateral lesions. The syndrome of hemispatial neglect is usually associated with large deficits of attention of the non-dominant hemisphere.
Additional images
-
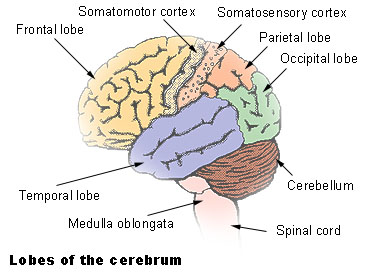
Lobes
-
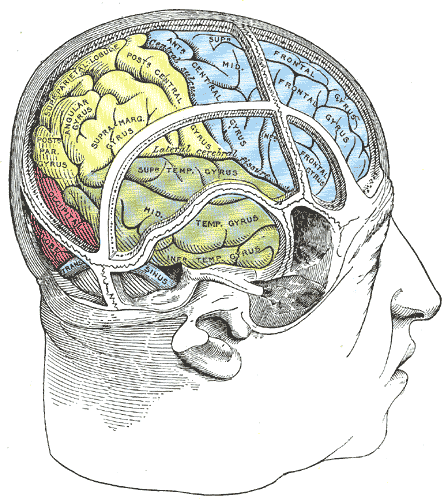
Drawing to illustrate the relations of the brain to the skull.


References
- ↑ Blakemore & Frith (2005). The Learning Brain. Blackwell Publishing. ISBN 1-4051-2401-6
- ↑ 2.0 2.1 2.2 Avillac M, Deneve S, Olivier E, Pouget A, Duhamel JR. (2005) Reference frames for representing visual and tactile locations in parietal cortex. Nat Neurosci. 8(7):941-9.
- ↑ Zhang T, Heuer HW, Britten KH. (2004) Parietal area VIP neuronal responses to heading stimuli are encoded in head-centered coordinates. Neuron 42(6):993-1001.
- ↑ Pesaran B, Nelson MJ, Andersen RA. (2006) Dorsal premotor neurons encode the relative position of the hand, eye, and goal during reach planning. Neuron 51(1):125-34.
- ↑ 5.0 5.1 Murata A, Gallese V, Luppino G, Kaseda M, Sakata H. (2000) Selectivity for the shape, size, and orientation of objects for grasping in neurons of monkey parietal area AIP. J Neurophysiol 83(5):2580. PMID 10805659
- ↑ Murata A, Gallese V, Kaseda M, Sakata H. (1996) Parietal neurons related to memory-guided hand manipulation. J Neurophysiol 75(5):2180-6. PMID 8734616
See also
Lobes of the brain Template:Prosencephalon
de:Parietallappen nl:Pariëtale kwab no:Isselapp fi:Päälakilohko sv:Parietallob