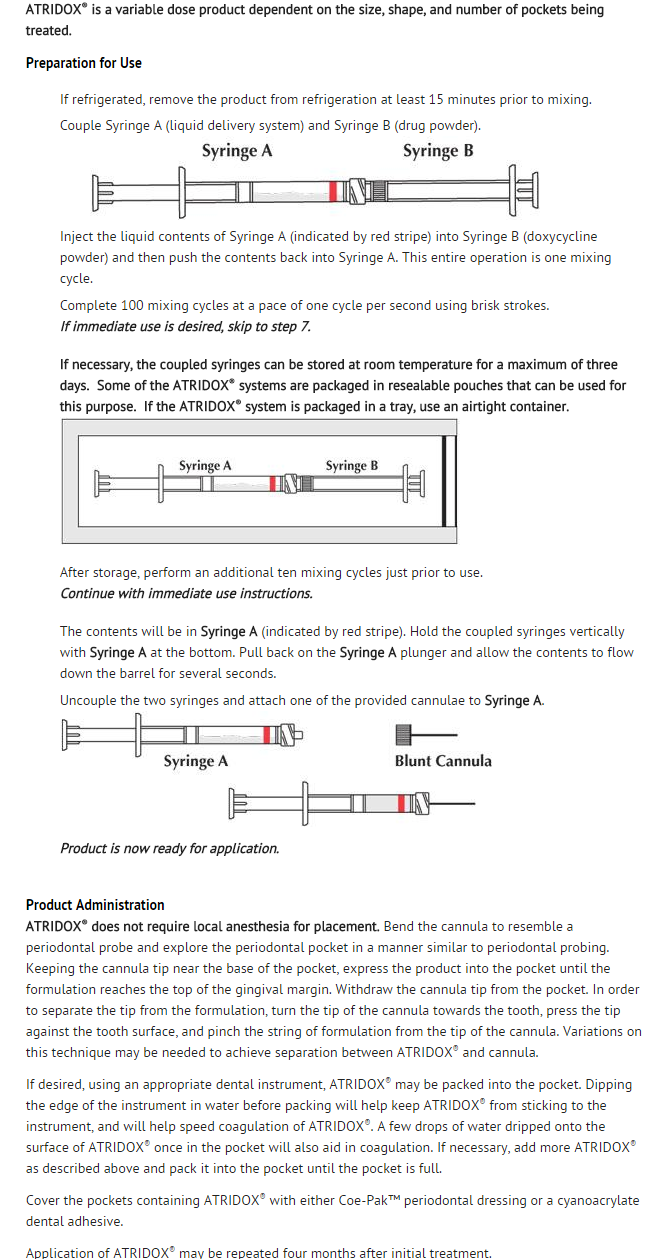
Doxycycline (subgingival)
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Doxycycline (subgingival) is an antibiotic that is FDA approved for the treatment of adult periodontitis. Common adverse reactions include anorexia,nausea,vomiting, diarrhea, dysphagia,edema, urticaria, hemolytic anaemia, neutropenia, eosinophilia.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Indication
- Doxycycline is indicated for use in the treatment of chronic adult periodontitis for a gain in clinical attachment, reduction in probing depth, and reduction in bleeding on probing.
Dosage
This image is provided by the National Library of Medicine.

Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Doxycycline (subgingival) in adult patients.
Non–Guideline-Supported Use
- Acinetobacter infection: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Acinetobacter infection: severe infections, 100 mg ORALLY every 12 hours.
- Acne vulgaris; Adjunct: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Acne vulgaris; Adjunct: severe infections, 100 mg ORALLY every 12 hours.
- Actinomycotic infection: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Actinomycotic infection: severe infections, 100 mg ORALLY every 12 hours.
- Amebic infection - Intestinal infectious disease: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Amebic infection - Intestinal infectious disease: severe infections, 100 mg ORALLY every 12 hours. (postexposure) 100 mg ORALLY every 12 hours for 60 days; in combination with 1 to 2 additional antibiotics.
- Anthrax: (cutaneous, postexposure) 100 mg ORALLY every 12 hours for 60 days; (cutaneous, naturally occurring) 100 mg every 12 hours for 7 to 10 days.
- Bartonellosis: (bacillary angiomatosis, peliosis hepatis, bacteremia, osteomyelitis in patients with HIV) 100 mg ORALLY every 12 hours for at least 3 months (guideline dosing).
- Bartonellosis: (CNS infection or severe infections in patients with HIV) 100 mg ORALLY every 12 hours, with or without rifampin 300 mg ORALLY or IV every 12 hours for 4 months.
- Bartonellosis: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses; for severe infections, 100 mg ORALLY every 12 hours.
- Brucellosis; Adjunct: 200 mg ORALLY daily for 6 weeks in combination with streptomycin (clinical trial dosing).
- Brucellosis; Adjunct: 100 mg ORALLY every 12 hours on day 1, then 100 mg ORALLY daily OR 100 mg ORALLY every 12 hours for more severe infections (manufacturer dosing).
- Chancroid: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Chancroid: severe infections, 100 mg ORALLY every 12 hours.
- Chlamydial infection: 100 mg ORALLY twice daily for 7 days.
- Cholera: 300 mg ORALLY as a single dose or 100 mg ORALLY twice a day for 3 days.
- Clostridial infection: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Clostridial infection: severe infections, 100 mg ORALLY every 12 hours.
- Epididymitis: 100 mg ORALLY every twice daily for 10 days plus ceftriaxone 250 mg IM as a single dose.
- Gonorrhea, Uncomplicated: (infection of the cervix, urethra, or rectum) 100 mg ORALLY twice daily for 7 days plus a single dose of either IM ceftriaxone 250 mg or ORAL cefixime 400 mg.
- Gonorrhea, Uncomplicated: (infection of the pharynx) 100 mg ORALLY twice daily for 7 days plus a single dose of ceftriaxone 250 mg IM.
- Gonorrhea, Uncomplicated: (except anorectal infections in men) 100 mg ORALLY every 12 hours for 7 days or 300 mg single dose followed in 1 hour by another 300 mg single dose (manufacturer dosing)
- Granuloma inguinale: 100 mg ORALLY twice daily for at least 21 days and lesions are healed completely.
- Human anaplasmosis: 100 mg twice daily ORALLY for 10 days for human granulocytic anaplasmosis alone or concomitant Lyme disease.
- Inclusion conjunctivitis: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Inclusion conjunctivitis: severe infections, 100 mg ORALLY every 12 hours.
- Infection by Campylobacter fetus: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Infection by Campylobacter fetus: severe infections, 100 mg ORALLY every 12 hours.
- Infection due to Enterobacteriaceae: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Infection due to Enterobacteriaceae: severe infections, 100 mg ORALLY every 12 hours.
- Infection due to Escherichia coli: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Infection due to Escherichia coli: severe infections, 100 mg ORALLY every 12 hours.
- Infection of skin AND/OR subcutaneous tissue: (methicillin-susceptible Staphylococcus aureus or MRSA) 100 mg ORALLY twice daily (guideline dosing).
- Infective endocarditis: (documented Bartonella endocarditis, culture positive) 100 mg ORALLY every 12 hours for 6 weeks AND gentamicin sulfate 1 mg/kg IV/IM every 8 hours for 2 weeks.
- Infective endocarditis: (suspected Bartonella endocarditis, culture negative) 100 mg ORALLY every 12 hours for 6 weeks, in combination with ceftriaxone sodium 2 g IV/IM every 24 hours for 6 weeks AND gentamicin sulfate 1 mg/kg IV/IM every 8 hours for 2 weeks.
- Infective proctitis: 100 mg ORALLY twice daily for 7 days plus ceftriaxone 250 mg IM as a single dose .
- Inhalational anthrax, Postexposure; Prophylaxis: 100 mg ORALLY every 12 hours for at least 60 days.
- Late latent syphilis, or latent syphilis of unknown duration; Penicillin allergy: 100 mg ORALLY twice daily for 28 days.
- Listeriosis: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Listeriosis: severe infections, 100 mg ORALLY every 12 hours.
- Lyme disease: 100 mg twice daily ORALLY for 14 days (range, 10 to 21 days) in early localized or early disseminated Lyme disease associated with erythema migrans; for 14 days (range, 14 to 21 days) in Lyme carditis to complete a course of therapy or to treat ambulatory patients; for 14 days (range, 14 to 21 days) for seventh cranial-nerve palsy with no CNS involvement; for 28 days for Lyme arthritis without neurological involvement; for 14 days (range, 10 to 21 days) for borrelial lymphocytoma; for 21 days for acrodermatitis chronica atrophicans.
- Lyme disease: (intolerant of beta-lactam agents) 200 to 400 mg/day ORALLY in 2 divided doses for 14 days (range, 10 to 28 days) for Lyme meningitis or seventh-cranial-nerve palsy with CNS involvement; for 14 days (range, 14 to 21 days) for Lyme carditis for the initial treatment of hospitalized patients.
- Lyme disease; Prophylaxis: 200 mg ORALLY as a single dose .
- Lymphogranuloma venereum: 100 mg ORALLY twice daily for 21 days.
- Malaria; Adjunct: (uncomplicated) 100 mg ORALLY twice daily for 7 days; give in combination with quinine sulfate 650 mg ORALLY 3 times daily for 3 days (or 7 days if infection is acquired in Southeast Asia) (guideline dosing).
- Malaria; Adjunct: (severe) 100 mg ORALLY twice daily for 7 days; give in combination with quinidine gluconate 10 mg/kg IV loading dose over 1 to 2 hours then 0.02 mg/kg/min IV continuous infusion for at least 24 hours, and continue for 3 days if infection acquired in Africa or South America or 7 days if infection is acquired in Southeast Asia; may switch to oral quinine once parasite density is less than 1% (guideline dosing).
- Malaria; Prophylaxis: 100 mg ORALLY once a day beginning 1 to 2 days prior to travel, continued during travel, and for 4 weeks after travel to malarious area .
- Nongonococcal cervicitis: 100 mg ORALLY twice daily for 7 days.
- Nongonococcal urethritis: 100 mg ORALLY twice daily for 7 days.
- Operative procedure on female genital system including obstetrics - Postoperative infection;
- Prophylaxis: (hysterosalpingography or chromotubation) 100 mg ORALLY twice daily for 5 days.
- Operative procedure on female genital system including obstetrics - Postoperative infection; Prophylaxis: (surgical abortion) 100 mg ORALLY 1 hour prior and 200 mg after procedure.
- Pelvic inflammatory disease: 100 mg ORALLY every 12 hours in combination with cefoxitin 2 g IV every 6 hours or cefotetan 2 g IV every 12 hours (recommended) or ampicillin/sulbactam 3 g IV every 6 hours (alternative); other alternative is doxycycline 100 mg ORALLY twice daily with or without metronidazole 500 mg ORALLY twice daily for 14 days plus a single IM dose of either ceftriaxone 250 mg or cefoxitin 2 g (for cefoxitin, also give probenecid 1 g orally as a single dose).
- Plague: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Plague: severe infections, 100 mg ORALLY every 12 hours.
- Psittacosis: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Psittacosis: severe infections, 100 mg ORALLY every 12 hours.
- Q fever: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Q fever: severe infections, 100 mg ORALLY every 12 hours.
- Relapsing fever: 100 mg ORALLY twice a day for a total of 5 to 10 days.
- Respiratory tract infection: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses; severe infections, 100 mg ORALLY every 12 hours.
- Respiratory tract infection: (acute uncomplicated bacterial rhinosinusitis; initial empiric therapy alternative) 100 mg ORALLY twice daily OR 200 mg ORALLY daily for 5 to 7 days (guideline dosing).
- Rocky Mountain spotted fever: 100 mg ORALLY every 12 hours; treat for at least 3 days following resolution of fever and until clinical improvement is observed; total duration is typically 7 to 14 days OR 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses; for more severe infections, 100 mg ORALLY every 12 hours.
- Rosacea, inflammatory lesions (papules and pustules): 40 mg ORALLY once daily in the morning (1 hour before or 2 hours after a meal).
- Sexually transmitted infectious disease; Prophylaxis - Victim of sexual aggression: 100 mg ORALLY twice daily for 7 days plus metronidazole 2 g ORALLY as a single dose plus either ceftriaxone 250 mg IM or cefixime 400 mg orally as a single dose.
- Shigellosis: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Shigellosis: severe infections, 100 mg ORALLY every 12 hours.
- Spotted fevers: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Spotted fevers: severe infections, 100 mg ORALLY every 12 hours.
- Staphylococcal infection of skin: (tablet) 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses.
- Staphylococcal infection of skin: (tablet) severe infections, 100 mg ORALLY every 12 hours, including for MRSA-associated purulent cellulitis
- Syphilis, Primary, secondary, or early latent; Penicillin allergy: early, 100 mg ORALLY twice daily for 14 days
- Syphilis, Primary, secondary, or early latent; Penicillin allergy: infection of over one year's duration, 100 mg ORALLY every 12 hours for 4 weeks
- Tularemia, Postexposure: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses
- Tularemia, Postexposure: severe infections, 100 mg ORALLY every 12 hours
- Typhus group rickettsial disease: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses
- Typhus group rickettsial disease: severe infections, 100 mg ORALLY every 12 hours
- Urinary tract infectious disease: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses
- Urinary tract infectious disease: severe infections, 100 mg ORALLY every 12 hours [3]
- Vincent's infection: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses
- Vincent's infection: severe infections, 100 mg ORALLY every 12 hours
- Yaws: 100 mg ORALLY every 12 hours on day 1, then 100 mg/day ORALLY in 1 to 2 divided doses
- Yaws: severe infections, 100 mg ORALLY every 12 hours.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Doxycycline (subgingival) in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Doxycycline (subgingival) in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Doxycycline (subgingival) in pediatric patients.
Contraindications
There is limited information regarding Doxycycline (subgingival) Contraindications in the drug label.
Warnings
- THE USE OF DRUGS OF THE TETRACYCLINE CLASS DURING TOOTH DEVELOPMENT (LAST HALF OF PREGNANCY, INFANCY, AND CHILDHOOD TO THE AGE OF EIGHT YEARS) MAY CAUSE PERMANENT DISCOLORATION OF THE TEETH. This adverse reaction is more common during long-term use of the drugs, but has been observed following repeated short-term courses. Enamel hypoplasia has also been reported. TETRACYCLINE DRUGS, THEREFORE, SHOULD NOT BE USED IN THIS AGE GROUP, OR IN PREGNANT WOMEN, UNLESS OTHER DRUGS ARE NOT LIKELY TO BE EFFECTIVE OR ARE CONTRAINDICATED. Results of animal studies indicate that tetracyclines cross the placenta, are found in fetal tissues, and can have toxic effects on the developing fetus (often related to skeletal development).
- Evidence of embryotoxicity has also been noted in animals treated early in pregnancy. If any tetracycline is used during pregnancy, the patient should be apprised of the potential hazard to the fetus.
- Photosensitivity manifested by an exaggerated sunburn reaction has been observed in some individuals taking doxycycline or other tetracyclines. Patients apt to be exposed to direct sunlight or ultraviolet light should be advised that this reaction can occur with tetracycline drugs.
Adverse Reactions
Clinical Trials Experience
- In clinical trials involving a total of 1436 patients, adverse experiences from all causalities were monitored across treatment groups.
- In the Circulatory System category, 10 subjects (1.6%) in the Doxycycline group were reported as having "unspecified essential hypertension." Only 1 subject (0.2%) in the Vehicle group, and none in the Scaling and Root Planing or Oral Hygiene groups were reported to have "unspecified essential hypertension." In all cases, the event occurred anywhere from 13 to 134 days post treatment. There is no known association of oral administration of doxycycline with essential hypertension.
- Two patients in the polymer vehicle group and none in the Doxycycline group (0.2% for both groups combined) reported adverse events consistent with a localized allergic response.
- Sex, age, race and smoking status did not appear to be correlated with adverse events.
- The following table lists the incidence of treatment-emergent adverse events from all causalities, across all treatment groups, occurring in ≥1% of the entire study population.

This image is provided by the National Library of Medicine.

Postmarketing Experience
There is limited information regarding Postmarketing Experience of Doxycycline (subgingival) in the drug label.
Drug Interactions
There is limited information regarding Doxycycline (subgingival) Drug Interactions in the drug label.
Use in Specific Populations
Pregnancy
- Pregnancy Category
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Doxycycline (subgingival) in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Doxycycline (subgingival) during labor and delivery.
Nursing Mothers
- Tetracyclines appear in breast milk following oral administration. It is not known whether doxycycline is excreted in human milk following use of Doxycycline. Because of the potential for serious adverse reactions in nursing infants from doxycycline, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
There is no FDA guidance on the use of Doxycycline (subgingival) with respect to pediatric patients.
Geriatic Use
There is no FDA guidance on the use of Doxycycline (subgingival) with respect to geriatric patients.
Gender
There is no FDA guidance on the use of Doxycycline (subgingival) with respect to specific gender populations.
Race
There is no FDA guidance on the use of Doxycycline (subgingival) with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Doxycycline (subgingival) in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Doxycycline (subgingival) in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Doxycycline (subgingival) in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Doxycycline (subgingival) in patients who are immunocompromised.
Administration and Monitoring
Administration
Monitoring
There is limited information regarding Monitoring of Doxycycline (subgingival) in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Doxycycline (subgingival) in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- Description
Management
- Description
Chronic Overdose
There is limited information regarding Chronic Overdose of Doxycycline (subgingival) in the drug label.
Pharmacology


Mechanism of Action
- Doxycycline is a broad-spectrum semisynthetic tetracycline.1 Doxycycline is bacteriostatic, inhibiting bacterial protein synthesis due to disruption of transfer RNA and messenger RNA at ribosomal sites.1In vitro testing has shown that Porphyromonas gingivalis, Prevotella intermedia, Campylobacter rectus, and Fusobacterium nucleatum, which are associated with periodontal disease, are susceptible to doxycycline at concentrations ≤ 6.0 µg/mL.2 A single-center, single-blind, randomized, clinical study in 45 subjects with periodontal disease demonstrated that a single treatment with Doxycycline resulted in the reduction in the numbers of P. gingivalis, P. intermedia, C. rectus, F. nucleatum, Bacteroides forsythus, and E. corrodens in subgingival plaque samples. Levels of aerobic and anaerobic bacteria were also reduced after treatment with Doxycycline. The clinical significance of these findings, however, is not known. During these studies, no overgrowth of opportunistic organisms such as Gram-negative bacilli and yeast were observed. However, as with other antibiotic preparations, Doxycycline therapy may result in the overgrowth of nonsusceptible organisms including fungi.
Structure
There is limited information regarding Doxycycline (subgingival) Structure in the drug label.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Doxycycline (subgingival) in the drug label.
Pharmacokinetics
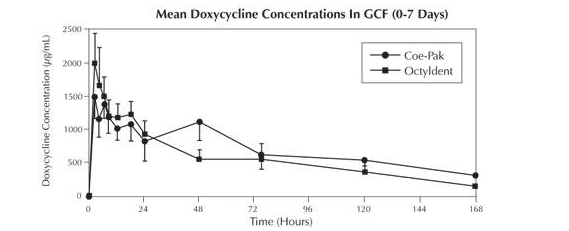
- In a clinical pharmacokinetic study, subjects were randomized to receive either Doxycycline covered with Coe-Pak™ periodontal dressing (n=13), Doxycycline covered with Octyldent™ periodontal adhesive (n=13), or oral doxycycline (n=5) (according to package dosing instructions). The doxycycline release characteristics in gingival crevicular fluid (GCF), saliva, and serum were evaluated.
- Doxycycline levels in GCF peaked (~1,500 µg/mL and ~2000 µg/mL for Coe-Pak™ and Octyldent™ groups, respectively) 2 hours following treatment with Doxycycline. These levels remained above 1000 µg/mL through 18 hours, at which time the levels began to decline gradually. However, local levels of doxycycline remained well above the minimum inhibitory concentration (MIC90) for periodontal pathogens (≤ 6.0 µg/mL)2 through Day 7. In contrast, subjects receiving oral doxycycline had peak GCF levels of ~2.5 µg/mL at 12 hours following the initial oral dosing with levels declining to ~0.2 µg/mL by Day 7. High variability was observed for doxycycline levels in GCF for both oral and Doxycycline treatment groups.
This image is provided by the National Library of Medicine.

Nonclinical Toxicology
There is limited information regarding Nonclinical Toxicology of Doxycycline (subgingival) in the drug label.
Clinical Studies
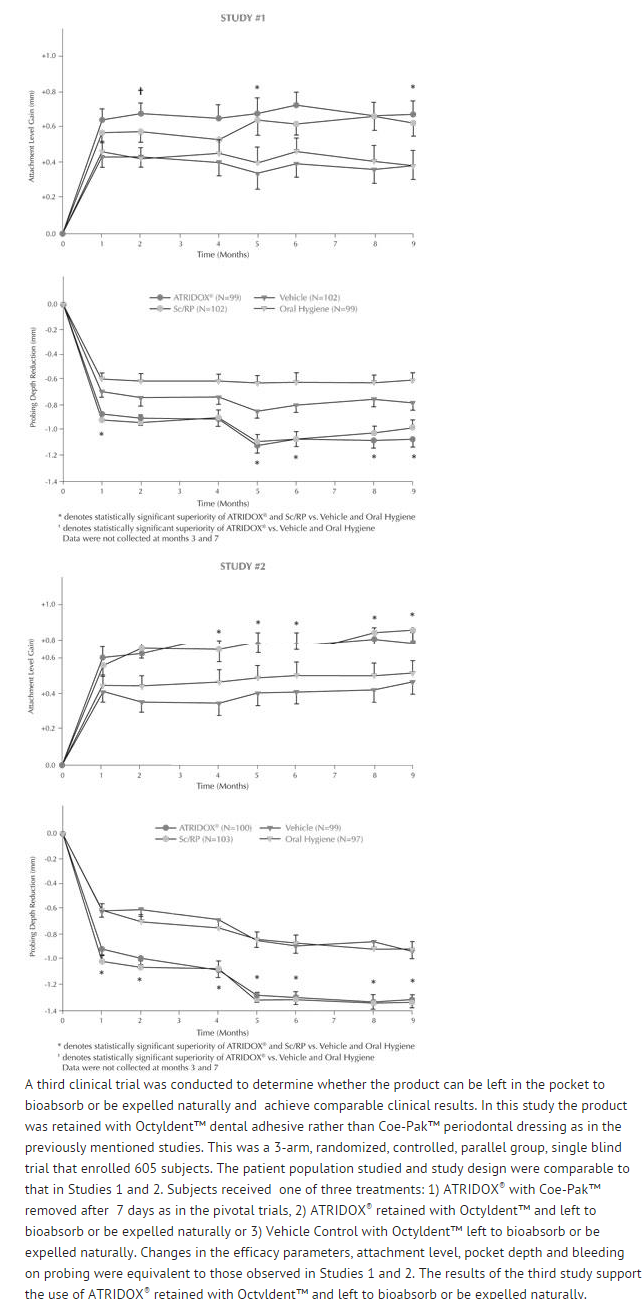
- In two well-controlled, multicenter, parallel-design, nine-month clinical trials, 831 patients (Study 1=411; Study 2=420) with chronic adult periodontitis characterized by a mean probing depth of 5.9 to 6.0 mm were enrolled. Subjects received one of four treatments: 1) Doxycycline, 2) Scaling and Root Planing, 3) Vehicle Control, or 4) Oral Hygiene. Treatment was administered to sites with probing depths 5 mm or greater that bled on probing. Subjects with detectable subgingival calculus on greater than 80% of all tooth surfaces were excluded from enrollment. All subjects received a second administration of the initially randomized treatment four months after their Baseline treatment. Changes in the efficacy parameters, attachment level, pocket depth, and bleeding on probing, between Baseline and Month 9 showed that: 1) Doxycycline was superior to Vehicle Control and Oral Hygiene, and 2) Doxycycline met the decision rule of being at least 75% as good as Scaling and Root Planing (SRP) (the standard of at least 75% as good as SRP is required for any product approved as a stand alone therapy for periodontitis). Clinicians should note that the studies were of nine months duration. Additional research would be necessary to establish long term comparability to SRP. The results of Studies #1 and 2 for efficacy parameters of attachment level gain and probing depth reduction are included in the following graphs.
This image is provided by the National Library of Medicine.

How Supplied
- The final blended product is 500 mg of formulation containing 50 mg of doxycycline hyclate (doxycycline hyclate, 10%).
- ATRIDOX® is available as a tray or pouch containing a doxycycline hyclate syringe (50 mg), an ATRIGEL® Delivery System syringe (450 mg), and a blunt cannula. The pouched product is available in a box of six (NDC 63646-191-00), or box of two (NDC 63646-191-02), or a professional sample pouch (NDC 63646-191-01). The trayed product is available in a box of six (NDC 63646-191-05), a box of four (NDC 63646-191-04), or a professional sample box of two (NDC 63646-191-03).
- Each doxycycline syringe system is intended for use in only one patient. Do not use if packaging has been previously opened or damaged.
Storage
- Store at 2°-30°C (36°-86°F).
Images
Drug Images
{{#ask: Page Name::Doxycycline (subgingival) |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel













{{#ask: Label Page::Doxycycline (subgingival) |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Doxycycline (subgingival) in the drug label.
Precautions with Alcohol
- Alcohol-Doxycycline (subgingival) interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- ATRIDOX®[1]
Look-Alike Drug Names
There is limited information regarding Doxycycline (subgingival) Look-Alike Drug Names in the drug label.
Price
References
The contents of this FDA label are provided by the National Library of Medicine.