Ventricular tachycardia electrocardiogram: Difference between revisions
Avirupguha (talk | contribs) No edit summary |
Avirupguha (talk | contribs) No edit summary |
||
| Line 3: | Line 3: | ||
==Electrocardography(EKG)== | ==Electrocardography(EKG)== | ||
===Overview=== | ===Overview=== | ||
The diagnosis of [[Ventricular tachycardia]] almost completely depends on EKG findings. The details are illustrated below. It is important to differentiate it from other wide complex tachycardias. | The diagnosis of [[Ventricular tachycardia]] almost completely depends on EKG findings. The details are illustrated below. It is important to differentiate it from other wide complex tachycardias. | ||
===Electrocardiographic diagnostic findings=== | ===Electrocardiographic diagnostic findings<ref name='book1'> Zimetbaum PJ, Josephson ME(2009). ''Practical Clinical Electrophysiology'' (1st ed.). Philadelphia, Pa: Lippincott Williams & Wilkins.</ref>=== | ||
[[Image:Lead II rhythm ventricular tachycardia Vtach VT.jpg|500 px|center|thumb|Ventricular tachycardia in Lead II (rhythm)]] | [[Image:Lead II rhythm ventricular tachycardia Vtach VT.jpg|500 px|center|thumb|Ventricular tachycardia in Lead II (rhythm)]] | ||
| Line 89: | Line 90: | ||
==References== | ==References== | ||
{{reflist| | {{reflist|1}} | ||
[[Category: Electrophysiology]] | [[Category: Electrophysiology]] | ||
{{WH}} | {{WH}} | ||
{{WS}} | {{WS}} | ||
Revision as of 14:50, 17 October 2011
|
Ventricular tachycardia Microchapters |
|
Differentiating Ventricular Tachycardia from other Disorders |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Ventricular tachycardia electrocardiogram On the Web |
|
to Hospitals Treating Ventricular tachycardia electrocardiogram |
|
Risk calculators and risk factors for Ventricular tachycardia electrocardiogram |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-in Chief: Avirup Guha, M.B.B.S.[2]
Electrocardography(EKG)
Overview
The diagnosis of Ventricular tachycardia almost completely depends on EKG findings. The details are illustrated below. It is important to differentiate it from other wide complex tachycardias.
Electrocardiographic diagnostic findings[1]

- Abnormal and wide QRS complexes with secondary ST segment and T wave changes.
- Usual QRS duration is > 0.12 seconds, may be shorter if the ectopic focus is located in the ventricular septum.
- The secondary ST segment and T wave changes are in a direction that is opposite the major deflection of the QRS.
- A ventricular rate between 140 and 200 BPM.
- When the rate is >200 and has a sine wave appearance, it is called ventricular flutter.
- When the rate is <110 BPM it is called non-paroxysmal VT.
- A regular or slightly irregular (up to 0.03 seconds) rhythm.
- Abrupt onset and termination.
- AV dissociation.
- Atrial rate slower than ventricular rate.
- No relationship between atrial activity and ventricular activity.
- There can be VA conduction.
- The RP interval is >0.11 seconds.
- Occurs in about 50% of cases.
- Uncommon when the ventricular rate is rapid (only 1/7 when the rate was>200).
- Axis
- Northwest quadrant is almost always VT in adults.
- In someone with a normal QRS in sinus rhythm, a LBBB-like wide complex tachycardia with a right axis (+90 to +180) is always VT because activation in LBBB aberration always goes from right to left.
- Concordance
- If all the precordial leads are positive (R) or negative (QS) the rhythm is very likely VT
- V1-V2 morphology
- RBBB-morphology
- RsR' or rsR' in V1 favors SVT, whereas a monophasic R, Rr', qR, or RS favors VT.
- RBBB aberration the initial forces of the QRS are the same as in the narrow complex sinus rhythm.
- LBBB-morphology
- V1 and V2 require analysis because the initial forces in V1 are often isoelectric.
- R wave in V1 or V2 ≥40 msec favors VT.
- The time from the onset of the QRS to the nadir of the S wave in V1 or V2 is ≥70 msec, VT is likely in the absence of Na channel blocking agents.
- RBBB-morphology
- V6 morphology
- RBBB-morphology - QS or rS favors VT. Although this can be influenced by axis (it is almost always seen in VT with left axis deviation, but is seen in only approximately 50% of VT with a normal axis, even in the same patient).
- LBBB-morphology - a qR or QS is highly predictive of VT
- Capture beats.
- Occurs when a supraventricular impulse is conducted and captures the ventricle.
- They are rare.
- Fusion beats.
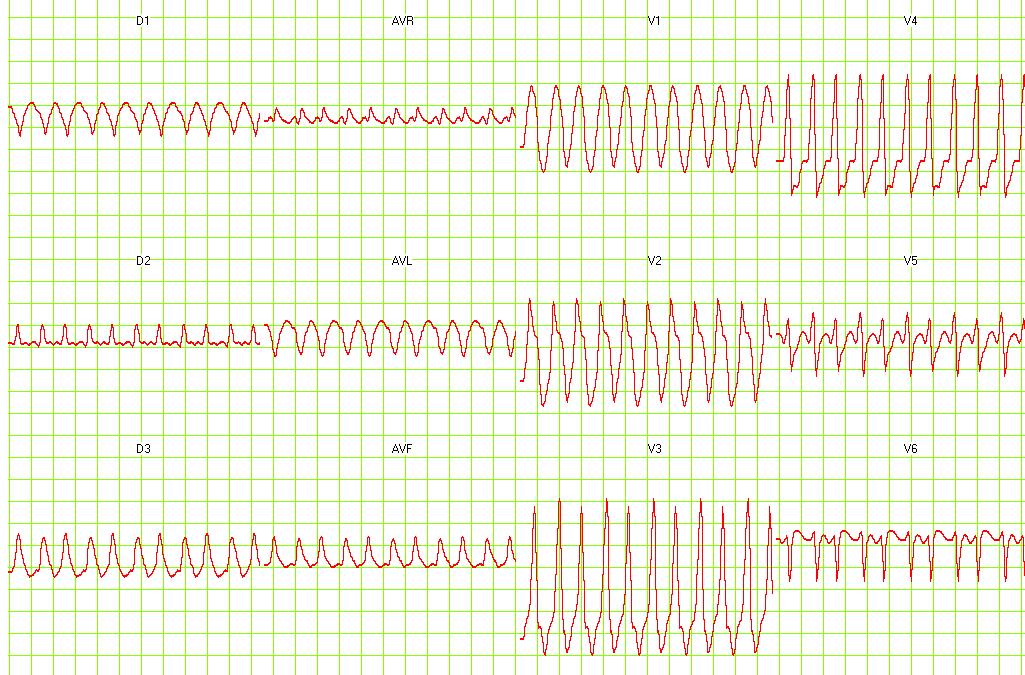
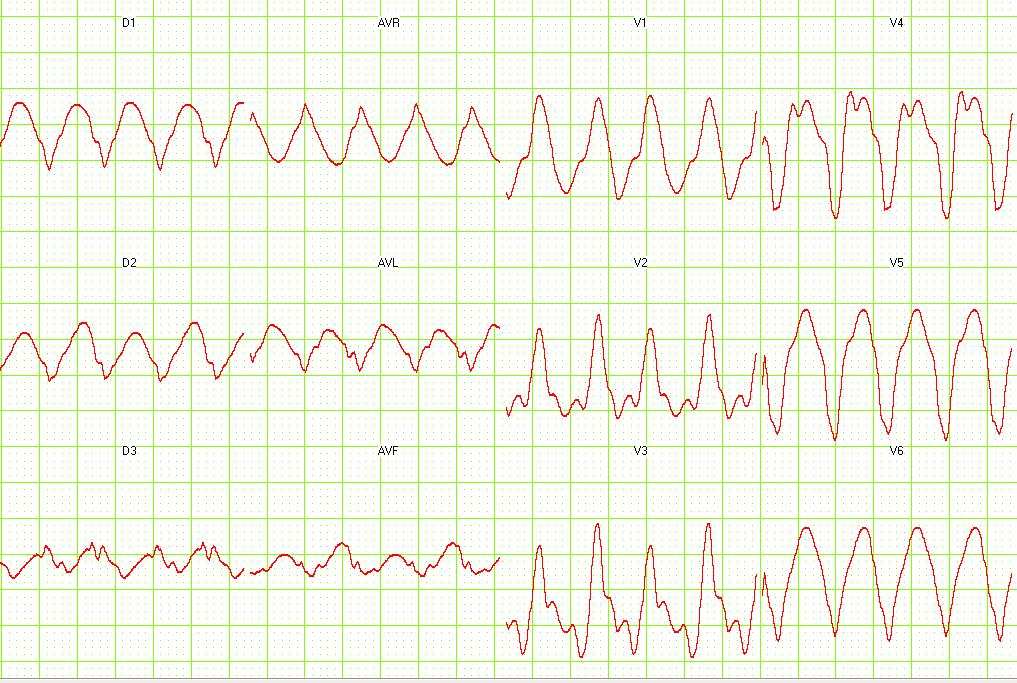
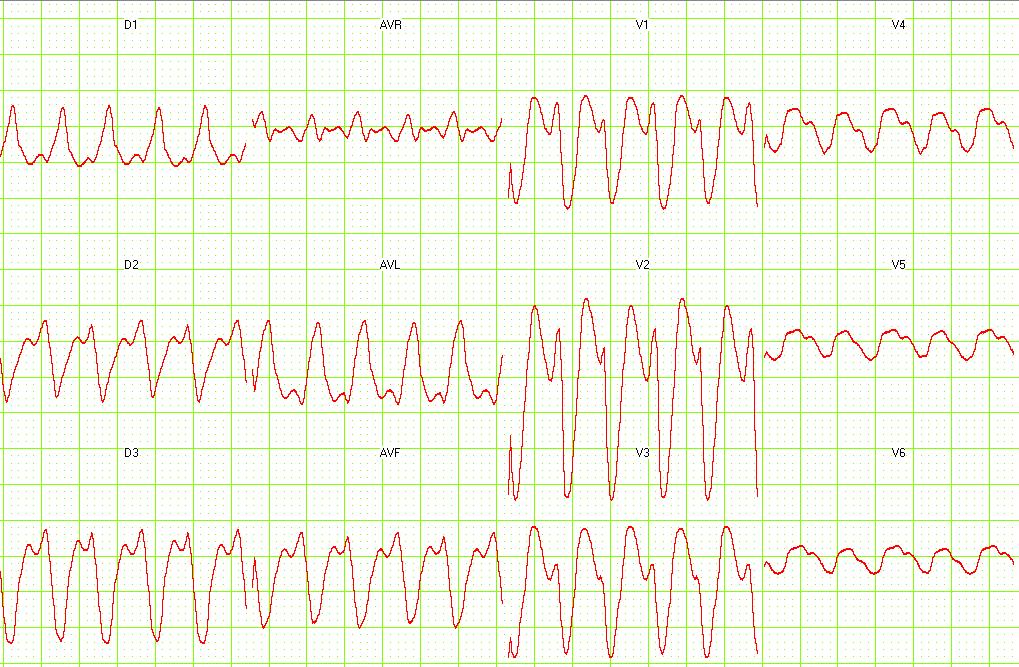
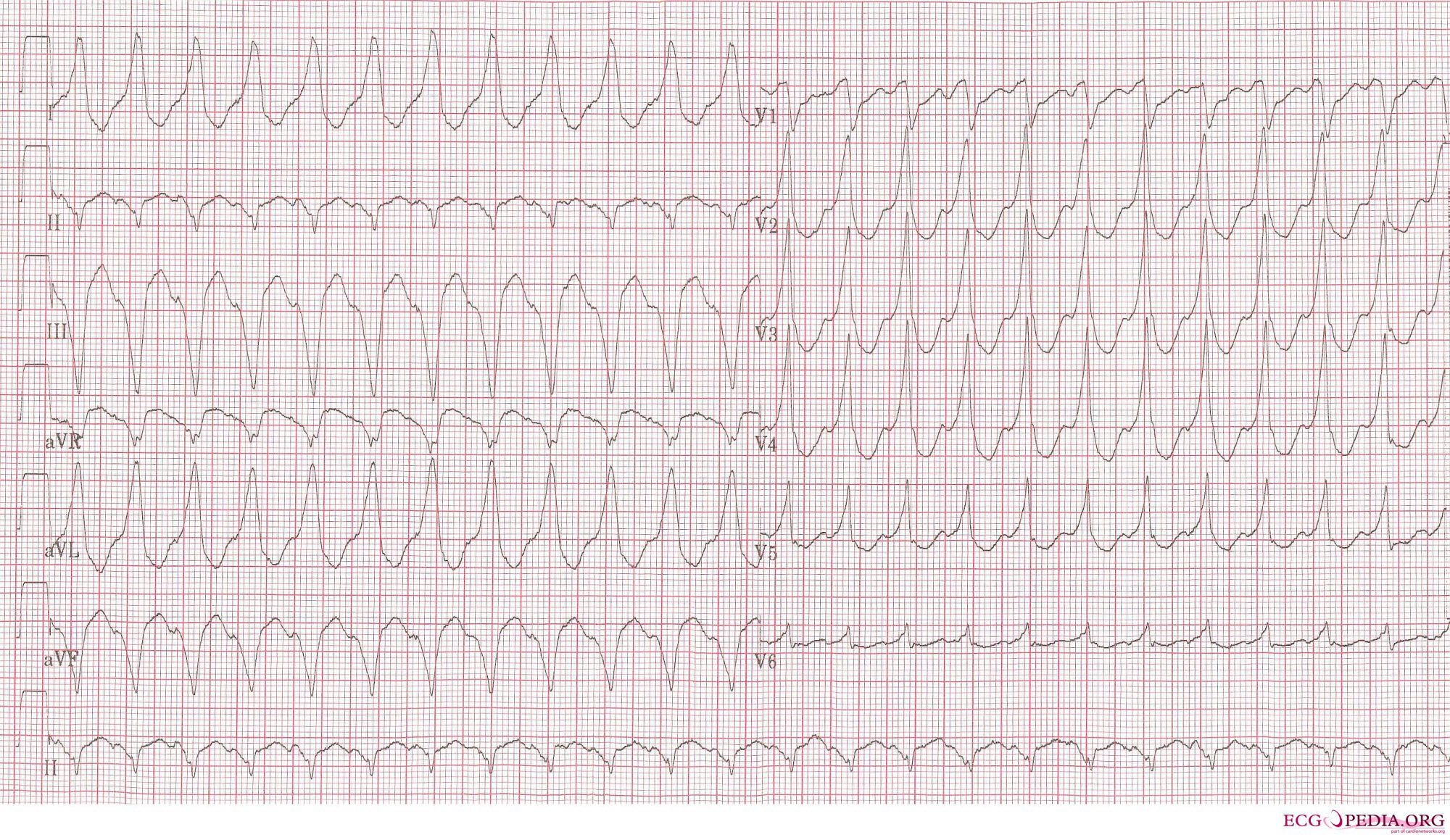
Examples of Ventricular Tachycardia:
-

12 lead EKG: Ventricular tachycardia.
-

12 lead EKG: Ventricular tachycardia. Image courtesy of Dr Jose Ganseman


-
12 lead EKG: Ventricular tachycardia. Image courtesy of Dr Jose Ganseman
-

12 lead EKG: Ventricular tachycardia. Image courtesy of Dr Jose Ganseman


-
12 lead EKG: Ventricular tachycardia. Image courtesy of Dr Jose Ganseman
-
12 lead EKG: Ventricular tachycardia. Image courtesy of Dr Jose Ganseman


-
Ventricular tachycardia of 140 bpm with a left bundle branch block pattern and left heart axis.
-
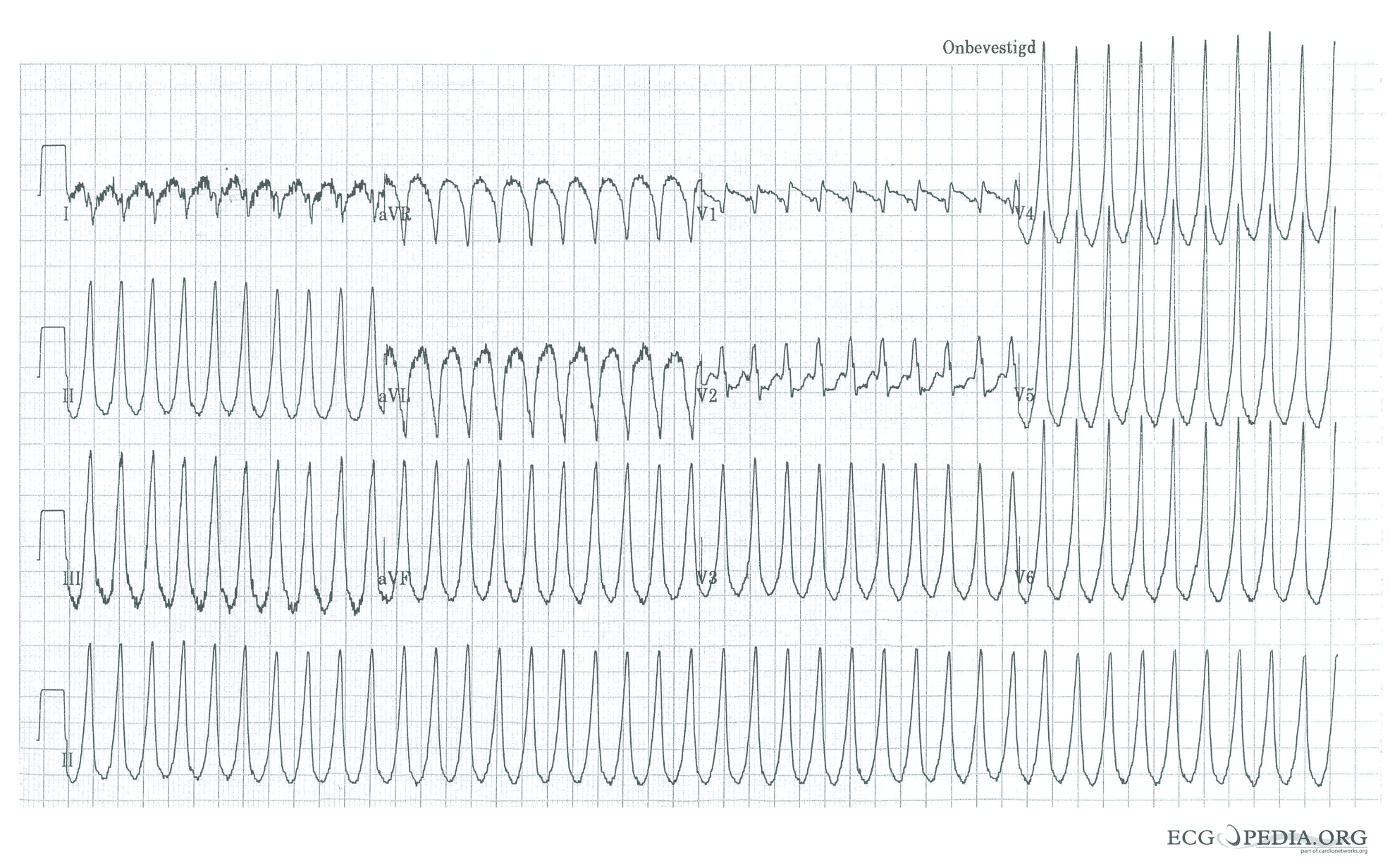
Ventricular tachycardia of 250 bpm with a right bundle branch block pattern and right heart axis.


-
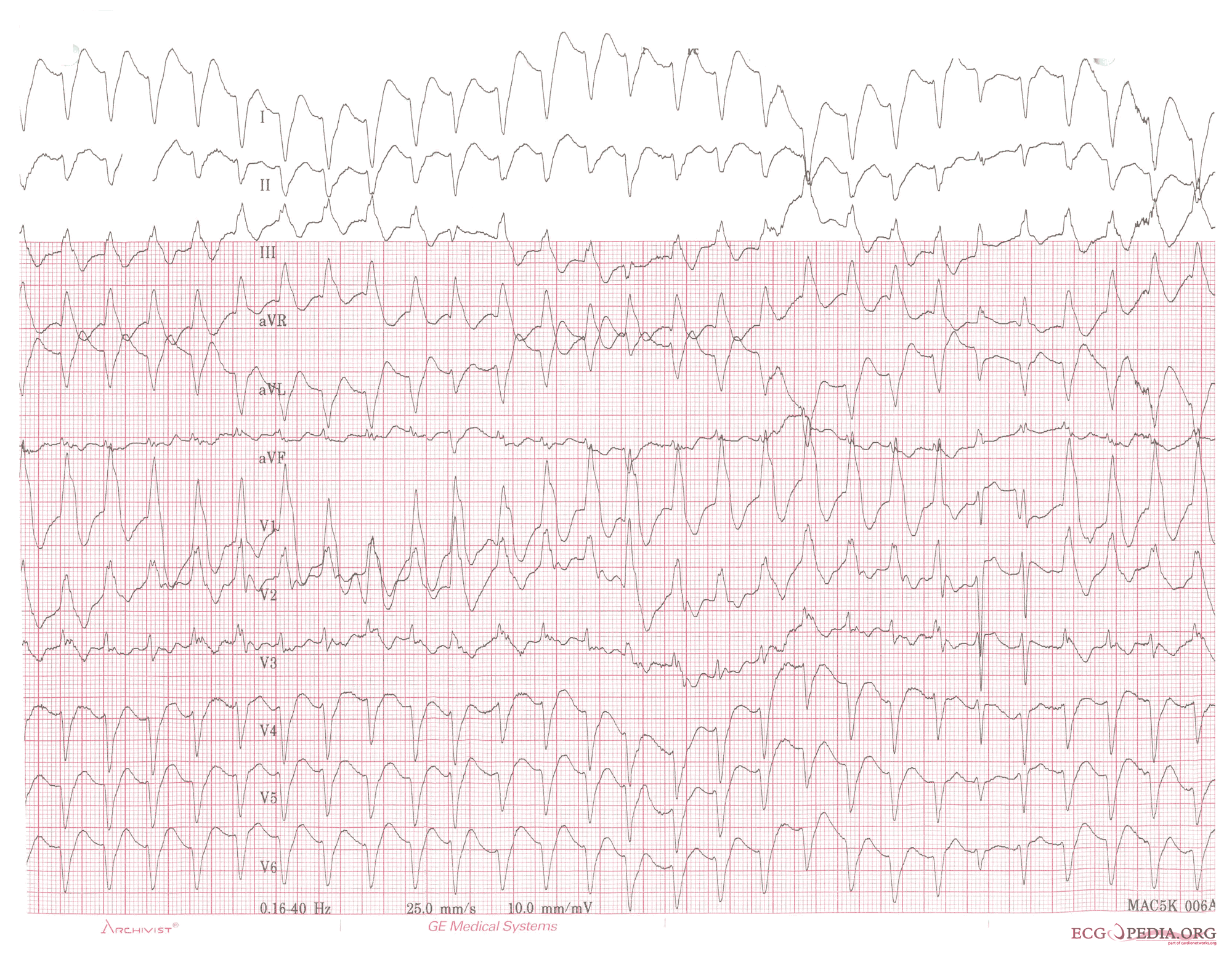
Ventricular tachycardia of 150 bpm with a right bundle branch block pattern and right heart axis. Note the 5th and 6th complex from the right side. These are fusion complexes.
-
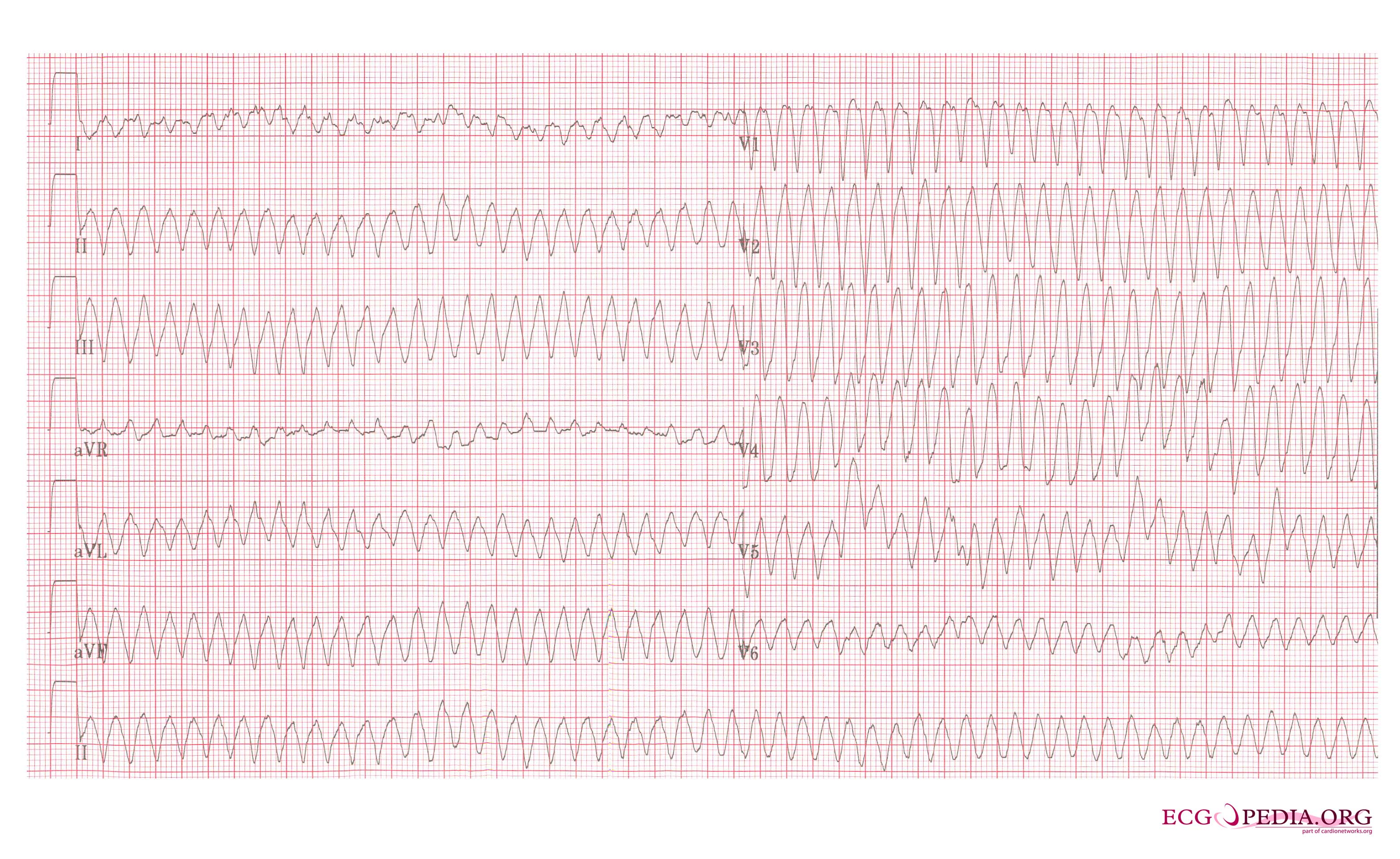
Ventricular flutter on a 12 lead ECG


References
- ↑ Zimetbaum PJ, Josephson ME(2009). Practical Clinical Electrophysiology (1st ed.). Philadelphia, Pa: Lippincott Williams & Wilkins.
- ↑ Chou's Electrocardiography in Clinical Practice Third Edition, pp. 398-409.
- ↑ Sailer, Christian, Wasner, Susanne. Differential Diagnosis Pocket. Hermosa Beach, CA: Borm Bruckmeir Publishing LLC, 2002:194 ISBN 1591032016
- ↑ Hammill S. C. Electrocardiographic diagnoses: Criteria and definitions of abnormalities, Chapter 18, MAYO Clinic, Concise Textbook of Cardiology, 3rd edition, 2007 ISBN 0-8493-9057-5