Tuberculous pericarditis pathophysiology: Difference between revisions
No edit summary |
No edit summary |
||
| (7 intermediate revisions by the same user not shown) | |||
| Line 2: | Line 2: | ||
{{Tuberculous pericarditis}} | {{Tuberculous pericarditis}} | ||
{{CMG}}; '''Associate Editor-In-Chief:''' [[Varun Kumar]], M.B.B.S.; [[Lakshmi Gopalakrishnan]], M.B.B.S. | {{CMG}}; '''Associate Editor-In-Chief:''' {{Fs}}, [[Varun Kumar]], M.B.B.S.; [[Lakshmi Gopalakrishnan]], M.B.B.S. | ||
==Overview== | ==Overview== | ||
Tuberculous pericarditis is the result of hematogenous or [[lymphatic]] spread of mycobacterium tuberculosis to the [[pericardium]]. This causes acute [[inflammation]] of the [[pericardium]] and we may have [[Polymorphonuclear cells|polymorphonuclear]] ([[PMN]]) and [[leukocytes]] infiltration in the [[pericardium]]. This may lead to [[pericardial effusion]] and [[fibrinous]] changes of the [[pericardium]]. The visceral [[pericardium]] thickens with [[fibrin]] deposition (changes of [[constrictive pericarditis]]). There are four pathologic stages of involvement: stage 1 is presence of diffuse [[fibrin]] deposition, [[granulomas]] and abundant [[mycobacterium]]. '''Stage 2 is''' development of [[serous]] or [[Serosanguineous discharge|serosanguineous]] [[pericardial effusion]] with a predominantly [[Lymphocyte|lymphocytic]] [[exudate]] with [[monocytes]] and [[foam cell]]s. Stage 3 is absorption of the effusion with organization of granulomatous [[caseation]] and thickening of [[pericardium]] secondary to deposition of [[fibrin]] and [[collagen]]. '''Stage 4 is''' development of [[constrictive pericarditis]]. The [[pericardial space]] is obliterated by dense adhesions with marked thickening of [[parietal]] layer and replacement of [[granulomas]] by [[fibrous tissue]]. Conditions associated with tuberculous pericarditis include [[pulmonary TB]], [[HIV]], [[malignancy]], [[chemotherapy]], and [[diabetes mellitus]]. On gross [[pathology]], thickened [[pericardium]], shaggy [[hemorrhage]], and [[exudate]] are characteristic findings of tuberculous pericarditis. On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis. | |||
==Pathophysiology== | ==Pathophysiology== | ||
=== Pathogenesis === | === Pathogenesis === | ||
* | * Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium.<ref name="pmid18610109">{{cite journal| author=Peel AA| title=TUBERCULOUS PERICARDITIS. | journal=Br Heart J | year= 1948 | volume= 10 | issue= 3 | pages= 195-207 | pmid=18610109 | doi= | pmc=PMC481044 | url= }} </ref><ref name="pmid4050698">{{cite journal| author=Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J| title=Primary acute pericardial disease: a prospective series of 231 consecutive patients. | journal=Am J Cardiol | year= 1985 | volume= 56 | issue= 10 | pages= 623-30 | pmid=4050698 | doi= | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=4050698 }} </ref><ref name="pmid16330703">{{cite journal| author=Mayosi BM, Burgess LJ, Doubell AF| title=Tuberculous pericarditis. | journal=Circulation | year= 2005 | volume= 112 | issue= 23 | pages= 3608-16 | pmid=16330703 | doi=10.1161/CIRCULATIONAHA.105.543066 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16330703 }} </ref><ref name="pmid14749455">{{cite journal| author=Sagristà-Sauleda J, Angel J, Sánchez A, Permanyer-Miralda G, Soler-Soler J| title=Effusive-constrictive pericarditis. | journal=N Engl J Med | year= 2004 | volume= 350 | issue= 5 | pages= 469-75 | pmid=14749455 | doi=10.1056/NEJMoa035630 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=14749455 }} </ref> | ||
* This causes acute inflammation of the [[pericardium]]. | |||
*We may have polymorphonuclear ([[PMN]]) and leukocytes infiltration in the pericardium. | |||
*Pericardial vascularization may happen as well. | |||
*This may lead to [[pericardial effusion]] and fibrinous changes of the pericardium. | |||
*[[Effusive constrictive pericarditis]] may be seen in some patients. | |||
*The visceral pericardium thickens with [[fibrin]] deposition (changes of [[constrictive pericarditis]]). | |||
*There are four pathologic stages of involvement: | |||
:'''Stage 1:''' Presence of diffuse [[fibrin]] deposition, [[granulomas]] and abundant [[mycobacterium]] | :* '''Stage 1:''' Presence of diffuse [[fibrin]] deposition, [[granulomas]] and abundant [[mycobacterium]] | ||
:'''Stage 2:''' Development of [[serous]] or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with [[monocytes]] and [[foam cell]]s | :* '''Stage 2:''' Development of [[serous]] or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with [[monocytes]] and [[foam cell]]s | ||
:'''Stage 3:''' Absorption of the effusion with organization of granulomatous [[caseation]] and thickening of [[pericardium]] secondary to deposition of [[fibrin]] and [[collagen]]. | :* '''Stage 3:''' Absorption of the effusion with organization of granulomatous [[caseation]] and thickening of [[pericardium]] secondary to deposition of [[fibrin]] and [[collagen]]. | ||
:'''Stage 4:''' Development of [[constrictive pericarditis]]. The pericardial space is obliterated by dense adhesions with marked thickening of [[parietal]] layer and replacement of [[granulomas]] by fibrous tissue | :* '''Stage 4:''' Development of [[constrictive pericarditis]]. The pericardial space is obliterated by dense adhesions with marked thickening of [[parietal]] layer and replacement of [[granulomas]] by fibrous tissue. | ||
==Genetics== | ==Genetics== | ||
The development of tuberculous pericarditis is not the result of any genetic mutation. | |||
== Associated Conditions == | == Associated Conditions == | ||
Conditions associated with tuberculous pericarditis include: | |||
* Pulmonary TB | |||
* HIV | |||
*Malignancy | |||
*Chemotherapy | |||
*Diabetes mellitus | |||
* | |||
==Gross Pathology Images== | ==Gross Pathology Images== | ||
[ | On gross [[pathology]], thickened [[pericardium]], shaggy [[hemorrhage]], and [[exudate]] are characteristic findings of tuberculous pericarditis. | ||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Pericarditis 0024.jpg| | <div align="left"><gallery heights="175" widths="175"> | ||
Image:Pericarditis 0024.jpg|[http://www.peir.net Images courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] | |||
</gallery> | </gallery> | ||
</div> | </div> | ||
==Microscopic Pathology Images== | ==Microscopic Pathology Images== | ||
[ | On microscopic histopathological analysis, [[acid fast bacilli]] is characteristic findings of tuberculous pericarditis. | ||
<div align="left"> | <div align="left"> | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
| Line 44: | Line 59: | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
<div align="left"> | <div align="left"> | ||
| Line 51: | Line 67: | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
[http://www.peir.net Images courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] | |||
==References== | ==References== | ||
Latest revision as of 15:36, 19 December 2019
|
Tuberculous pericarditis Microchapters |
|
Differentiating Tuberculous pericarditis from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Tuberculous pericarditis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Tuberculous pericarditis pathophysiology |
|
Risk calculators and risk factors for Tuberculous pericarditis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Fahimeh Shojaei, M.D., Varun Kumar, M.B.B.S.; Lakshmi Gopalakrishnan, M.B.B.S.
Overview
Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium. This causes acute inflammation of the pericardium and we may have polymorphonuclear (PMN) and leukocytes infiltration in the pericardium. This may lead to pericardial effusion and fibrinous changes of the pericardium. The visceral pericardium thickens with fibrin deposition (changes of constrictive pericarditis). There are four pathologic stages of involvement: stage 1 is presence of diffuse fibrin deposition, granulomas and abundant mycobacterium. Stage 2 is development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells. Stage 3 is absorption of the effusion with organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen. Stage 4 is development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of parietal layer and replacement of granulomas by fibrous tissue. Conditions associated with tuberculous pericarditis include pulmonary TB, HIV, malignancy, chemotherapy, and diabetes mellitus. On gross pathology, thickened pericardium, shaggy hemorrhage, and exudate are characteristic findings of tuberculous pericarditis. On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis.
Pathophysiology
Pathogenesis
- Tuberculous pericarditis is the result of hematogenous or lymphatic spread of mycobacterium tuberculosis to the pericardium.[1][2][3][4]
- This causes acute inflammation of the pericardium.
- We may have polymorphonuclear (PMN) and leukocytes infiltration in the pericardium.
- Pericardial vascularization may happen as well.
- This may lead to pericardial effusion and fibrinous changes of the pericardium.
- Effusive constrictive pericarditis may be seen in some patients.
- The visceral pericardium thickens with fibrin deposition (changes of constrictive pericarditis).
- There are four pathologic stages of involvement:
- Stage 1: Presence of diffuse fibrin deposition, granulomas and abundant mycobacterium
- Stage 2: Development of serous or serosanguineous pericardial effusion with a predominantly lymphocytic exudate with monocytes and foam cells
- Stage 3: Absorption of the effusion with organization of granulomatous caseation and thickening of pericardium secondary to deposition of fibrin and collagen.
- Stage 4: Development of constrictive pericarditis. The pericardial space is obliterated by dense adhesions with marked thickening of parietal layer and replacement of granulomas by fibrous tissue.
Genetics
The development of tuberculous pericarditis is not the result of any genetic mutation.
Associated Conditions
Conditions associated with tuberculous pericarditis include:
- Pulmonary TB
- HIV
- Malignancy
- Chemotherapy
- Diabetes mellitus
Gross Pathology Images
On gross pathology, thickened pericardium, shaggy hemorrhage, and exudate are characteristic findings of tuberculous pericarditis.

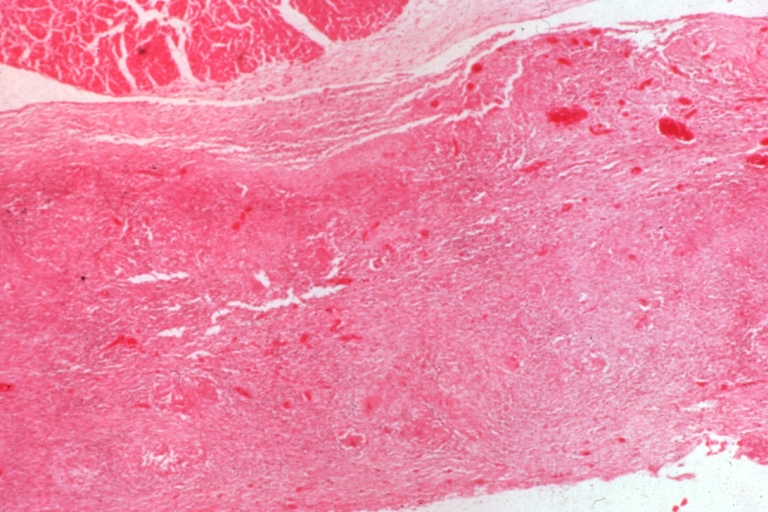
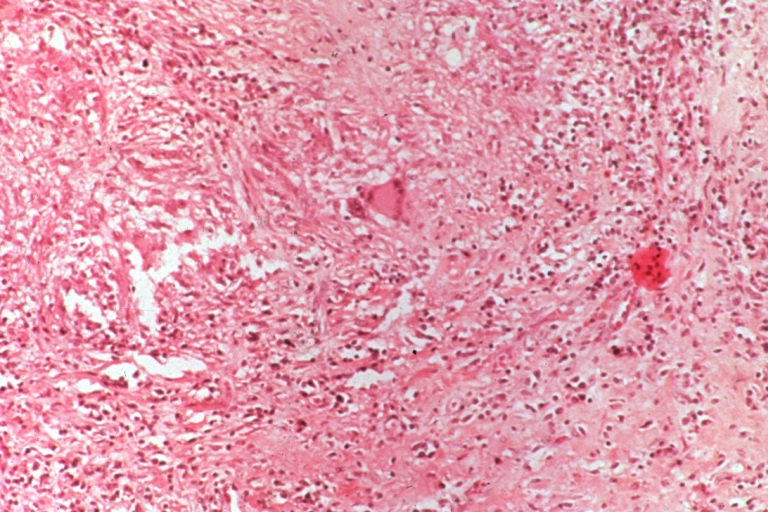
Microscopic Pathology Images
On microscopic histopathological analysis, acid fast bacilli is characteristic findings of tuberculous pericarditis.
-
Tuberculous pericarditis.
-
Tuberculous pericarditis.
-
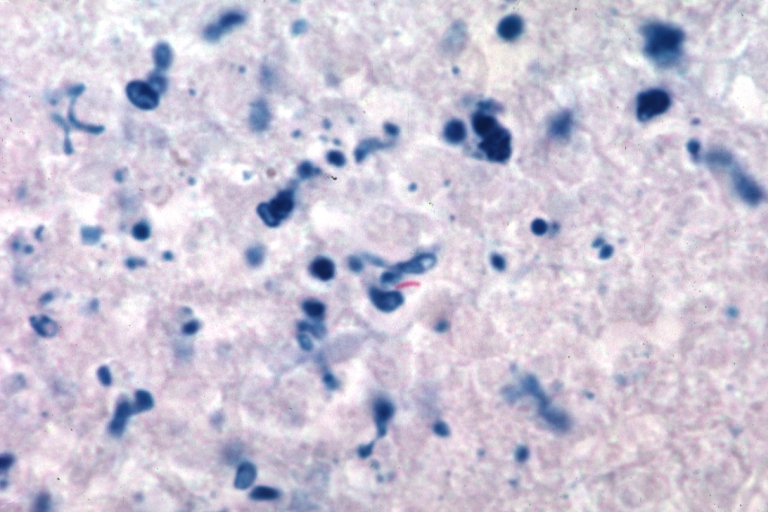
Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.



-
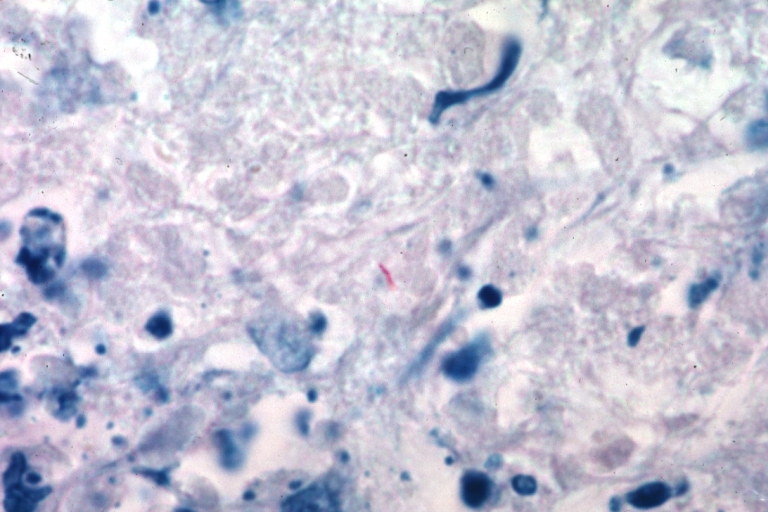
Tuberculous pericarditis: Micro oil acid fast stain. The organism easily seen.
-
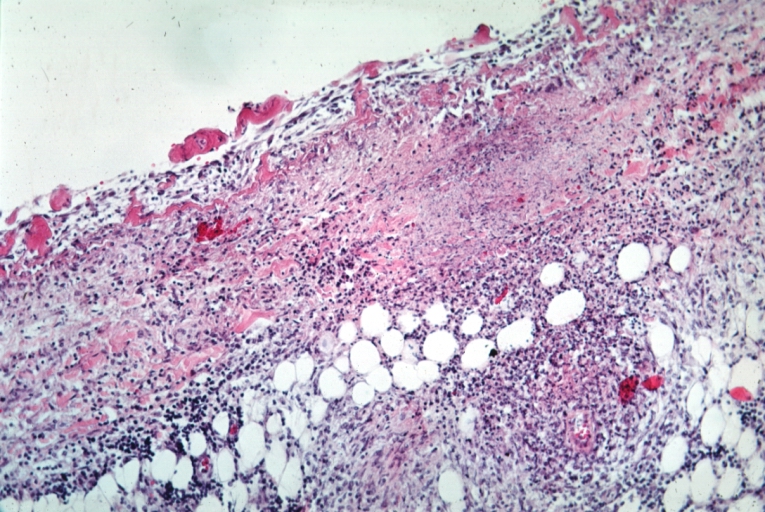
Tuberculous pericarditis: Micro med mag, H&E, a typical lesion.


References
- ↑ Peel AA (1948). "TUBERCULOUS PERICARDITIS". Br Heart J. 10 (3): 195–207. PMC 481044. PMID 18610109.
- ↑ Permanyer-Miralda G, Sagristá-Sauleda J, Soler-Soler J (1985). "Primary acute pericardial disease: a prospective series of 231 consecutive patients". Am J Cardiol. 56 (10): 623–30. PMID 4050698.
- ↑ Mayosi BM, Burgess LJ, Doubell AF (2005). "Tuberculous pericarditis". Circulation. 112 (23): 3608–16. doi:10.1161/CIRCULATIONAHA.105.543066. PMID 16330703.
- ↑ Sagristà-Sauleda J, Angel J, Sánchez A, Permanyer-Miralda G, Soler-Soler J (2004). "Effusive-constrictive pericarditis". N Engl J Med. 350 (5): 469–75. doi:10.1056/NEJMoa035630. PMID 14749455.