Tetralogy of Fallot pathophysiology: Difference between revisions
No edit summary |
No edit summary |
||
| Line 34: | Line 34: | ||
* This defect in outlet septum in turn leads to the four characteristic features: | * This defect in outlet septum in turn leads to the four characteristic features: | ||
[[File:1024px-Tetralogy of Fallot.svg.png|500px|none|thumb|Image by Mariana Ruiz LadyofHats| https://en.wikipedia.org/wiki/File:Tetralogy_of_Fallot.svg]] | [[File:1024px-Tetralogy of Fallot.svg.png|500px|none|thumb|Image by Mariana Ruiz LadyofHats| https://en.wikipedia.org/wiki/File:Tetralogy_of_Fallot.svg]]<br /> | ||
* There is anatomic variation between the hearts of individuals with tetralogy of Fallot. The degree of right ventricular outflow tract obstruction varies between patients and is generally determines clinical symptoms and disease progression. Tetralogy of Fallot may present with other anatomical anomalies, including: | *Ventricular Septal Defect | ||
**[[Ventricular septal defect]] is a hole between the two bottom chambers ([[ventricle]]s) of the [[heart]]. The defect is centered around the outlet septum, the most superior aspect of the [[septum]], and in the majority of cases is single and large. In some cases septal [[hypertrophy]] can narrow the margins of the defect.<ref name="gatzoulis">Gatzoulis MA, Webb GD, Daubeney PE. (2005) ''Diagnosis and Management of Adult Congenital Heart Disease''. Churchill Livingstone, Philadelphia. ISBN 0443071039.</ref> | |||
*Pulmonic Stenosis | |||
**[[Pulmonic stenosis]] is a right ventricular outflow tract obstruction | |||
*** A narrowing at ([[valvular stenosis]], seen in approximately 20-25% case) or just below (infundibular stenosis, seen in around 50% of cases) the [[heart|pulmonary valve]]. | |||
*** The stenosis is mostly the result of [[hypertrophy]] of the septoparietal trabeculae,<ref name="gatzoulis" /> however the deviated outlet septum is believed to play a role. | |||
*** The stenosis is the major cause of the malformations, with the other associated malformations acting as compensatory mechanisms to the [[pulmonic stenosis]].<ref>{{cite journal |author=Bartelings M, Gittenberger-de Groot A |title=Morphogenetic considerations on congenital malformations of the outflow tract. Part 1: Common arterial trunk and tetralogy of Fallot |journal=Int. J. Cardiol. |volume=32 |issue=2 |pages=213-30 |year=1991 |pmid=1917172}}</ref> | |||
*** The degree of stenosis varies between individuals with TOF, and is the primary determinant of symptoms and severity. This malformation is infrequently described as sub-pulmonary stenosis or subpulmonary obstruction.<ref>Anderson RH, Weinberg. The clinical anatomy of tetralogy of Fallot. Cardiol Young. 2005 15;38-47. PMID 15934690.</ref> | |||
*** Tetralogy of Fallot with [[pulmonary atresia]] or pseudotruncus arteriosus is a severe variant in which there is complete obstruction of the right ventricular outflow tract and absence of the [[pulmonary trunk]]. In these individuals, there is complete [[right-to-left shunt]]ing of [[blood]]. The [[lung]]s are perfused via extensive collaterals from the systemic arteries. | |||
*Overriding Aorta | |||
**[[Overriding aorta]] is defined as when the [[aortic valve]] is not restricted to the [[left ventricle]], thus having biventricular connections. The aortic root can be moved anteriorly or override the septal defect, but it is still to the right of the root of the [[pulmonary artery]]. The degree of override is quite variable, with 5-95% of the valve being connected to the [[right ventricle]].<ref name="gatzoulis" /> | |||
*Right Ventricular Hypertrophy | |||
**The [[right ventricle]] is more muscular than normal, causing a characteristic coeur-en-sabot (boot-shaped) appearance as seen by [[chest x-ray]]. Due to the misarrangement of the external ventricular septum, the right ventricular wall increase in size to deal with the increased obstruction to the right outflow tract. This feature is now generally agreed to be a secondary anomaly, as the level of hypertrophy generally increases with age.<ref>Anderson RH, Tynan M. Tetralogy of Fallot – a centennial review. Int J Cardiol. 1988 21; 219-232. PMID 3068155.</ref> | |||
* There is anatomic variation between the hearts of individuals with tetralogy of Fallot. | |||
*The degree of right ventricular outflow tract obstruction varies between patients and is generally determines clinical symptoms and disease progression. | |||
*Tetralogy of Fallot may present with other anatomical anomalies, including: | |||
**[[pulmonic stenosis|Stenosis of the left pulmonary artery]], in 40% of patients | **[[pulmonic stenosis|Stenosis of the left pulmonary artery]], in 40% of patients | ||
** A bicuspid [[pulmonary valve]], in 40% of patients | ** A bicuspid [[pulmonary valve]], in 40% of patients | ||
Revision as of 16:29, 12 February 2020
|
Tetralogy of fallot Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
|
|
Tetralogy of Fallot pathophysiology On the Web |
|
American Roentgen Ray Society Images of Tetralogy of Fallot pathophysiology |
|
Risk calculators and risk factors for Tetralogy of Fallot pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Priyamvada Singh, M.B.B.S. [2], Keri Shafer, M.D. [3]; Omar Toubat; Assistant Editor-In-Chief: Kristin Feeney, B.S. [4]
Overview
Tetralogy of Fallot is a congenital heart lesion characterized by a constellation of four morphologic abnormalities present in the newborn heart. These features include a ventricular septal defect, overriding aorta, pulmonary stenosis, and right ventricular hypertrophy. The obstruction of right ventricular outflow in tetralogy of Fallot causes blood to shunt or flow from the right to left side of heart through the ventricular septal defect. This causes right ventricular hypertrophy and eventual right sided heart failure. There is flow of deoxygenated venous blood from the right side of the heart to the systemic circulation resulting in cyanosis.
Pathophysiology
Physiology
- Subsequent to the lateral folding and looping events that give rise to the primitive heart tube are a series of complex septation processes that will ultimately complete morphogenesis of the four chambered heart.
- The goals of cardiac septation are two-fold:
- To create four distinct cardiac chambers
- To correctly position the great vessels relative to these chambers
- Improper execution of these septation events can give rise to many congenital heart defects, such as Tetralogy of Fallot.
Pathogenesis
Morphologic Basis for Tetralogy of Fallot
- It is understood that tetralogy of fallot is the result of improper positioning of the outlet septum.[1]
- In the normal heart, the outlet septum is an indistinguishable component of the crista supraventricularis that communicates with the septomarginal trabeculae to divide the right and left ventricular cavities.[2]
- In Tetralogy of Fallot, proper ventricular septation is perturbed by anterocephalad displacement of the outlet septum relative to the septomarginal trabecula.[3]
- The direct consequence of this malalignment is an overriding aortic orifice and a ventricular septal defect, resulting in an intracardiac right to left shunt of blood.
- In addition, anterocephalad displacement of the outlet septum indirectly predisposes the pulmonary trunk to stenosis in the setting of septoparietal trabecular hypertrophy.[1]
- Together, the displacement of the outlet septum coupled with the hypertrophic arrangement of the septoparietal trabeculae account for the three anatomical cardinal defects in Tetralogy of Fallot - aortic dextroposition, interventricular communication (VSD), and pulmonary stenosis.
- The fourth defect - right ventricular hypertrophy - is a hemodynamic consequence of these three morphologic changes, as the right ventricle physiologically adapts to the increased resistance of a stenotic pulmonary trunk.[1]
Anatomy
- This defect in outlet septum in turn leads to the four characteristic features:

- Ventricular Septal Defect
- Ventricular septal defect is a hole between the two bottom chambers (ventricles) of the heart. The defect is centered around the outlet septum, the most superior aspect of the septum, and in the majority of cases is single and large. In some cases septal hypertrophy can narrow the margins of the defect.[4]
- Pulmonic Stenosis
- Pulmonic stenosis is a right ventricular outflow tract obstruction
- A narrowing at (valvular stenosis, seen in approximately 20-25% case) or just below (infundibular stenosis, seen in around 50% of cases) the pulmonary valve.
- The stenosis is mostly the result of hypertrophy of the septoparietal trabeculae,[4] however the deviated outlet septum is believed to play a role.
- The stenosis is the major cause of the malformations, with the other associated malformations acting as compensatory mechanisms to the pulmonic stenosis.[5]
- The degree of stenosis varies between individuals with TOF, and is the primary determinant of symptoms and severity. This malformation is infrequently described as sub-pulmonary stenosis or subpulmonary obstruction.[6]
- Tetralogy of Fallot with pulmonary atresia or pseudotruncus arteriosus is a severe variant in which there is complete obstruction of the right ventricular outflow tract and absence of the pulmonary trunk. In these individuals, there is complete right-to-left shunting of blood. The lungs are perfused via extensive collaterals from the systemic arteries.
- Pulmonic stenosis is a right ventricular outflow tract obstruction
- Overriding Aorta
- Overriding aorta is defined as when the aortic valve is not restricted to the left ventricle, thus having biventricular connections. The aortic root can be moved anteriorly or override the septal defect, but it is still to the right of the root of the pulmonary artery. The degree of override is quite variable, with 5-95% of the valve being connected to the right ventricle.[4]
- Right Ventricular Hypertrophy
- The right ventricle is more muscular than normal, causing a characteristic coeur-en-sabot (boot-shaped) appearance as seen by chest x-ray. Due to the misarrangement of the external ventricular septum, the right ventricular wall increase in size to deal with the increased obstruction to the right outflow tract. This feature is now generally agreed to be a secondary anomaly, as the level of hypertrophy generally increases with age.[7]
- There is anatomic variation between the hearts of individuals with tetralogy of Fallot.
- The degree of right ventricular outflow tract obstruction varies between patients and is generally determines clinical symptoms and disease progression.
- Tetralogy of Fallot may present with other anatomical anomalies, including:
- Stenosis of the left pulmonary artery, in 40% of patients
- A bicuspid pulmonary valve, in 40% of patients
- Right sided aortic arch, in 25% of patients
- Coronary artery anomalies, in 10% of patients
- An atrial septal defect, in which case the syndrome is sometimes called a pentalogy of Fallot.
- An atrioventricular septal defect
- Partially or totally anomalous pulmonary venous return
- Forked ribs and scoliosis
{{#ev:youtube|ACRfFkxow7w}}
Embrylogy
- Embryologic studies show that tetralogy of Fallot is a result of anterior malalignment of the conal septum, resulting in the clinical combination of a ventricular septal defect (VSD), pulmonary stenosis, and an overriding aorta.
- Right ventricular hypertrophy is secondary to this combination of abnormalities, which causes resistance to blood flow from the right ventricle.

- Tetralogy of Fallot results in cyanosis, (hypoxia or low oxygenation) of the blood due to mixing of deoxygenated venous blood from the right ventricle with oxygenated blood in the left ventricle through the ventricular septal defect and preferential flow of both oxygenated and deoxygenated blood from the ventricles through the aorta because of obstruction to flow through the pulmonary valve.
- This is known as a right-to-left shunt.
- If pulmonary blood flow is dramatically reduced, pulmonary blood flow may depend on a patent ductus arteriosus (PDA) or bronchial collaterals.
- If obstruction of the right ventricular outflow tract is minimal, the intracardiac shunt may be mostly from left to right, and this may result in what is termed a pink tet or pink tetralogy.
- Although cyanosis is absent on clinical exam, laboratory testing will often show systemic oxygen desaturation.
- Children with tetralogy of Fallot may develop acute severe cyanosis or hypoxic tet spells.
- The mechanism underlying these episodes is not entirely clear, but may be due to spasm of the infundibular septum and the right ventricular outflow tract.
- Whatever the mechanism, there is an increase in resistance to blood flow to the lungs with increased preferential flow of desaturated blood to the systemic circulation.
- The child will often squat during a tet spell to improve venous return to the right side of the heart.
- Squatting increases the systemic vascular resistance and thereby shunts flow to pulmonary circuit.
- These spells can be fatal, and can occur in patients who are not cyanotic.
Genetics
- The cellular processes that underlie cardiogenesis are extensively regulated in the developing heart.
- Proper cardiac development requires the complex orchestration of cardiac transcription factors and signaling pathways in a spatiotemporal specific manner.
- Traditional genetic studies have implicated mutations in numerous genes encoding cardiac transcription factors and cell signaling proteins in the development of Tetralogy of Fallot.
- Specifically, heterozygous mutations in NKX2-5, HAND1, TBX5, and GATA4 have been reported in familial forms of disease.[8][9][10]
- Many of these single gene mutations result in haploinsufficiency and suggest a dose dependent relationship between genetic expression and disease.[11]
- While the mechanistic basis of this relationship is currently poorly understood, it is hypothesized that disruption of the direct protein-protein interactions that allow these transcription factors to work synergistically impedes the activation of downstream targets and signaling pathways central to cardiac morphogenesis.[12][13]
- In addition, recent whole-exome sequencing investigations have introduced a novel role for epigenetic dysregulation in the pathogenesis of Tetralogy of Fallot.[11][14]
- Aberrant epigenetic modifications are thought to provide an alternative mechanism to perturb normal spatiotemporal expression of these essential developmental genes.
Associated Conditions
- Right aortic arch seen in 25% of patients.
- Ostium secondum seen in 15% of patients.
- Coronary artery anomalies mainly LAD from RCA or right sinus valsalve is seen.
- Associated abnormalities include cleft lip, cleft palate, hypospadias, skeletal and craniofacial abnormalities.
Gross Pathology
-
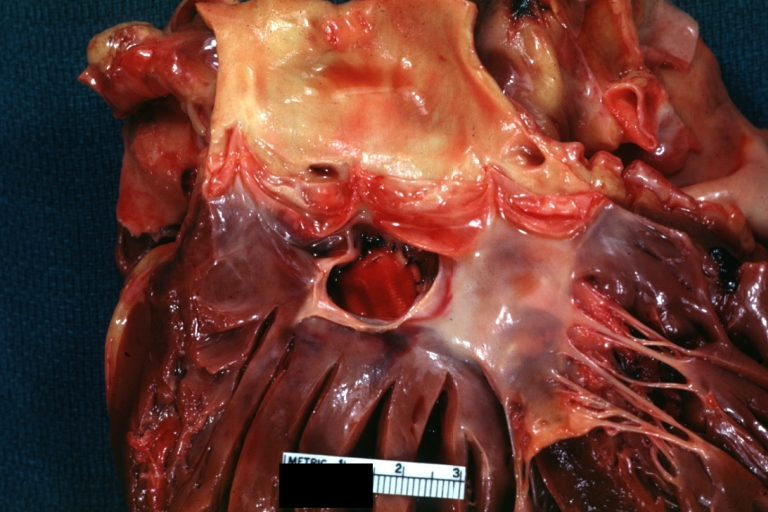
Tetralogy of Fallot: Gross, a good example of repaired perimembranous septal defect
-
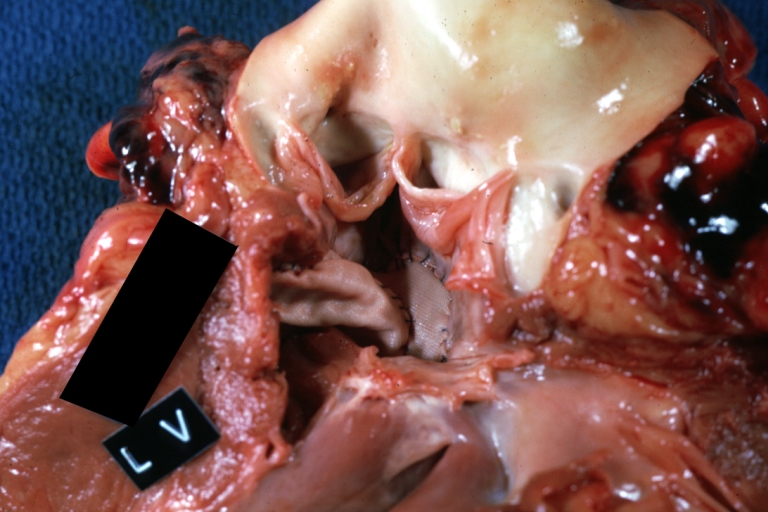
Tetralogy of Fallot: Gross, close-up of aortic valve with subvalvular septal defect with Dacron patch (very good example)


{kind=link}
Microscopic Pathology
Videos
{{#ev:youtube|b-TkE_wygT4}}
References
- ↑ 1.0 1.1 1.2 Anderson RH, Jacobs ML (2008). "The anatomy of tetralogy of Fallot with pulmonary stenosis". Cardiol Young. 18 Suppl 3: 12–21. doi:10.1017/S1047951108003259. PMID 19094375.
- ↑ Bashore TM (2007). "Adult congenital heart disease: right ventricular outflow tract lesions". Circulation. 115 (14): 1933–47. doi:10.1161/CIRCULATIONAHA.105.592345. PMID 17420363.
- ↑ Bailliard F, Anderson RH (2009). "Tetralogy of Fallot". Orphanet J Rare Dis. 4: 2. doi:10.1186/1750-1172-4-2. PMC 2651859. PMID 19144126.
- ↑ 4.0 4.1 4.2 Gatzoulis MA, Webb GD, Daubeney PE. (2005) Diagnosis and Management of Adult Congenital Heart Disease. Churchill Livingstone, Philadelphia. ISBN 0443071039.
- ↑ Bartelings M, Gittenberger-de Groot A (1991). "Morphogenetic considerations on congenital malformations of the outflow tract. Part 1: Common arterial trunk and tetralogy of Fallot". Int. J. Cardiol. 32 (2): 213–30. PMID 1917172.
- ↑ Anderson RH, Weinberg. The clinical anatomy of tetralogy of Fallot. Cardiol Young. 2005 15;38-47. PMID 15934690.
- ↑ Anderson RH, Tynan M. Tetralogy of Fallot – a centennial review. Int J Cardiol. 1988 21; 219-232. PMID 3068155.
- ↑ Olson EN (2006). "Gene regulatory networks in the evolution and development of the heart". Science. 313 (5795): 1922–7. doi:10.1126/science.1132292. PMID 17008524.
- ↑ Yang YQ, Gharibeh L, Li RG, Xin YF, Wang J, Liu ZM; et al. (2013). "GATA4 loss-of-function mutations underlie familial tetralogy of fallot". Hum Mutat. 34 (12): 1662–71. doi:10.1002/humu.22434. PMID 24000169.
- ↑ Bruneau BG (2008). "The developmental genetics of congenital heart disease". Nature. 451 (7181): 943–8. doi:10.1038/nature06801. PMID 18288184.
- ↑ 11.0 11.1 Bruneau BG, Srivastava D (2014). "Congenital heart disease: entering a new era of human genetics". Circ Res. 114 (4): 598–9. doi:10.1161/CIRCRESAHA.113.303060. PMID 24526674.
- ↑ Hiroi Y, Kudoh S, Monzen K, Ikeda Y, Yazaki Y, Nagai R; et al. (2001). "Tbx5 associates with Nkx2-5 and synergistically promotes cardiomyocyte differentiation". Nat Genet. 28 (3): 276–80. doi:10.1038/90123. PMID 11431700.
- ↑ Garg V, Kathiriya IS, Barnes R, Schluterman MK, King IN, Butler CA; et al. (2003). "GATA4 mutations cause human congenital heart defects and reveal an interaction with TBX5". Nature. 424 (6947): 443–7. doi:10.1038/nature01827. PMID 12845333.
- ↑ Sheng W, Qian Y, Wang H, Ma X, Zhang P, Diao L; et al. (2013). "DNA methylation status of NKX2-5, GATA4 and HAND1 in patients with tetralogy of fallot". BMC Med Genomics. 6: 46. doi:10.1186/1755-8794-6-46. PMC 3819647. PMID 24182332.