Superior oblique muscle
Template:Muscle infobox Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
For the abdominal muscle see: External oblique muscle
Overview
The superior oblique muscle, or obliquus oculi superior, is a fusiform muscle in the upper, medial side of the orbit whose primary action is intorsion and whose secondary actions are to abduct (laterally rotate) and depress the eyeball (i.e. it makes the eye move outward and downward). One of the extraocular muscles, the superior oblique is the only muscle innervated by the trochlear nerve.
The primary action of the superior oblique muscle is intorsion; the secondary action is depression (primarily in the adducted position); the tertiary action is abduction. A brief survey of neurology and physiology texts and websites reveals much confusion about the role of the superior oblique muscle, with many sources claiming that its role is to move the eye towards the nose. In fact, because of its positioning, it is able to rotate the eye away from the nose so that when the eye is already adducted (looking directly "inwards") its rotational action turns the pupil downwards to look towards the mouth, which many texts misinterpret as its primary action.
Usually the eye muscles do not work alone, which leads to the confusion of the primary actions. The superior oblique intorts, depresses, abducts the eye if it were to work by itself. Normally, the superior oblique, in conjunction with the medial rectus, causes the eye to ADduct.
The origin for the superior oblique is the annulus of Zinn at the orbital apex. It loops through a pulley like structure (the trochlea of superior oblique) and inserts on the posterotemporal surface of the eyeball.
It arises immediately above the margin of the optic foramen, above and medial to the origin of the superior rectus, and, passing forward, ends in a rounded tendon, which plays in a fibrocartilaginous ring or pulley attached to the trochlear fovea of the frontal bone.
The contiguous surfaces of the tendon and ring are lined by a delicate mucous sheath, and enclosed in a thin fibrous investment.
The tendon is reflected backward, lateralward, and downward beneath the superior rectus to the lateral part of the bulb of the eye, and is inserted onto the scleral surface, behind the equator of the eyeball, the insertion of the muscle lying between the superior rectus and Rectus lateralis.
Clinical significance
Superior oblique palsy is a common complication of closed head trauma. Restriction of superior oblique movement is found in Brown syndrome, leading to difficulty elevating the eye in the adducted position.
Superior oblique myokymia is an uncommon neurological condition caused by vascular compression of the trochlear nerve resulting in repeated, brief, involuntary episodes of movement of the eye.
Operations of the superior oblique include tenotomy, recession, silicone expander lengthening, split tendon lengthening, tucking, and the Harada-Ito procedure.
Additional images
-
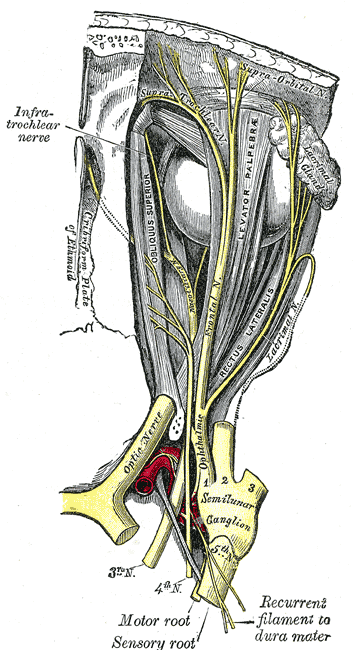
Nerves of the orbit. Seen from above.
-
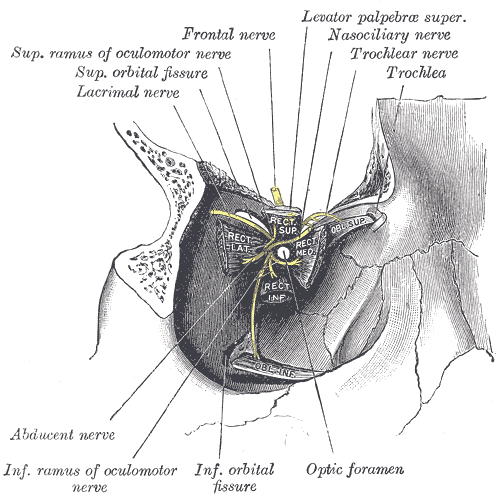
Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure.


External links
{kind=link}
Template:Gray's
Template:Muscles of head
hu:Musculus obliquus superior bulbi
nl:Musculus obliquus superior