Pubic symphysis
|
WikiDoc Resources for Pubic symphysis |
|
Articles |
|---|
|
Most recent articles on Pubic symphysis Most cited articles on Pubic symphysis |
|
Media |
|
Powerpoint slides on Pubic symphysis |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Pubic symphysis at Clinical Trials.gov Trial results on Pubic symphysis Clinical Trials on Pubic symphysis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Pubic symphysis NICE Guidance on Pubic symphysis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Pubic symphysis Discussion groups on Pubic symphysis Patient Handouts on Pubic symphysis Directions to Hospitals Treating Pubic symphysis Risk calculators and risk factors for Pubic symphysis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Pubic symphysis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
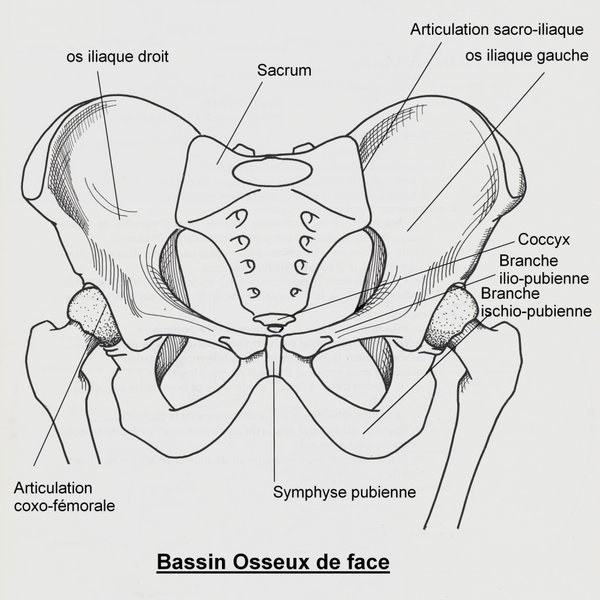
The pubic symphysis is the midline cartilaginous joint uniting the superior rami of the left and right pubic bones (pubis). It is located anterior to the urinary bladder and superior to the external genitalia; for females it is above the vulva and for males it is above the penis. In males, the suspensory ligament of the penis attaches to the pubic symphysis. In females, the pubic symphysis is intimately close to the clitoris.
Anatomy
Symphysis pubis is a non-synovial amphiarthrodial joint and comes from the Greek word "symphysis" meaning growing together. The anterior width of the symphysis pubis is 3-5 mm greater than its intrapelvic posterior width. This joint is connected by fibrocartilage and may contain a fluid filled cavity, the center is avascular; possibly due to the nature of the compressive forces passing through this joint which may lead to harmful vascular disease.[1] The ends of both pubic bones are covered by a thin layer of hyaline cartilage which is attached to the fibrocartilage. The fibrocartilaginous disk is reinforced by a series of ligaments. These ligaments cling to the fibrocartilaginous disk to the point that fibers intermix with it.
Two such ligaments are the superior and inferior, these being the ligaments that provide the most stability; the posterior and anterior ligaments are weaker. The strong and thicker superior ligament is reinforced by the tendons of the rectus abdominis, obliques externus, gracilis and thigh adductors muscles. The inferior ligament in the pubic arch is known as the arcuate pubic ligament.
At the time of birth the symphysis pubis is 9-10mm in width, with thick cartilaginous end-plates. By mid-adolescence the adult size is achieved. During adulthood the end-plates decrease in width to a thinner layer. Degeneration of the symphysis pubis accompanies aging and postpartum. Women have a greater thickness of this pubic disc which allows more mobility of the pelvic bones, hence providing a greater diameter of pelvic cavity during childbirth.
Fibrocartilage
Fibrocartilage is composed of small chained bundles of thick clearly defined type I collagenfibers. This fibrous connective tissue bundles have cartilage cells between them, these cells to a certain extent resemble tendon cells. The collagenous fibers are usually place in an orderly arrangement parallel to tension on the tissue. It has a low content of glycosaminoglycans (2% of dry weight). Glycosaminoglycans are long unbranched polysaccharides (relatively complex carbohydrates) consisting of a repeating disaccharide unit. Disaccharide a sugar (a carbohydrate) is composed of two monosaccharides. The two monosaccharides are bonded via a dehydration reaction that leads to the loss of a molecule of water. Fibrocartilage does not have a surrounding perichondrium. Perichondrium surrounds the cartilage of developing bone, it has a layer of dense irregular connective tissue and functions in the growth and repair of cartilage.
Hyaline cartilage
Hyaline cartilage is the white shiny gristle at the end of long bones. This cartilage has very poor healing potential, and efforts to get it to repair itself frequently end up with a similar, but poorer fibrocartilage.
Pregnancy
During pregnancy in the human, hormones such as relaxin remodells this cartilage allowing the pelvic bones to be more flexible for delivery. The non-pregnant gap of the symphysis pubis is 4-5mm but in pregnancy there will be an increase of at least 2-3mm, therefore, it is considered that a total width of up to 9mm between the two bones is normal for a pregnant woman. The symphysis pubis separates to some degree during the birthing process in some women this separation can become a diastasis of the symphysis pubis. The diastasis could be the result of a rapid birth [2] or a forceps delivery[3] or maybe even prenatal.[4]. A diastasis of the symphysis pubis is a symptom of pelvic girdle pain(PGP). PGP has a reported rate of occurrence of 1 in 37 women[5].
Symphysiotomy
Historically, when labor failed to progress because of the head of the fetus was too large, the mother's symphysis pubis was cut and the fetus' skull was crushed. The Caesarean section has allowed for the - largely safe - delivery of these infants (see Hope Langer, MD; NY Times Review of Books, Oct. 22, 2006)
In remote, isolated tropical areas women presenting with a large baby and small pelvis travelled for great distances for medical help; a symphysiotomy has been suggested [6]. This practise was carried out in Europe before the introduction of the Caesarean Section. It is still considered as an option in Third World countries [7].
Diseases of the Symphysis Pubis
Metabolic disease, such as renal osteodystrophy, produces widening, while ochronosis results in calcific deposits in the symphysis. Inflammatory disease, such as ankylosing spondylitis, results in bony fusion of the symphysis. Osteitis pubis, the most common inflammatory disease, is treated with anti-inflammatory medication and rest. Degenerative joint disease of the symphysis, which can cause groin pain, results from instability or from abnormal pelvic mechanics [8]
Use in forensic anthropology
The pubic symphysis have importance in the field of forensic anthropology, as they can be used to estimate the age of adult skeletons. Throughout life, the surfaces of the pubic symphysis are worn at a more or less predictable rate. By examining the wear of the pubic symphysis, it is possible to estimate the age of the person at death.[9]
Additional images
-
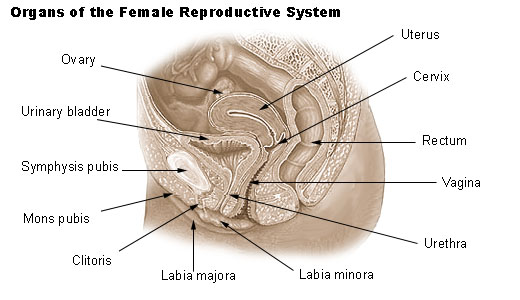
Organs of the female reproductive system.
-
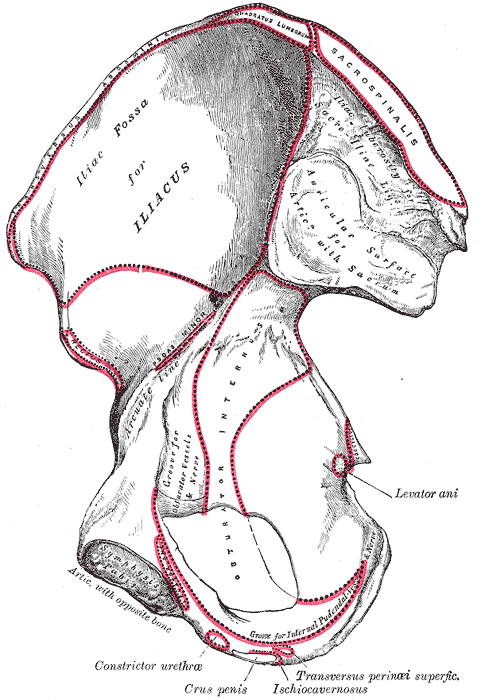
Right hip bone. Internal surface.
-
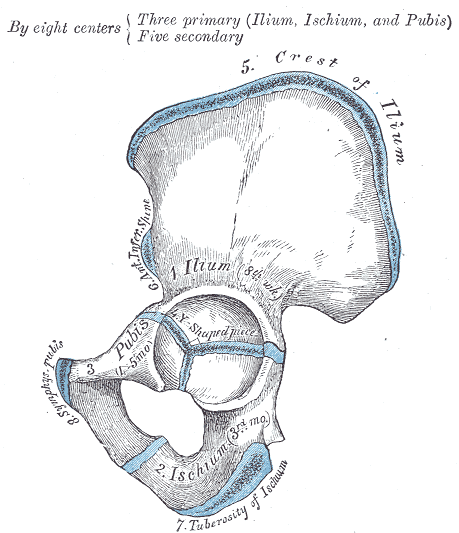
Plan of ossification of the hip bone.
-
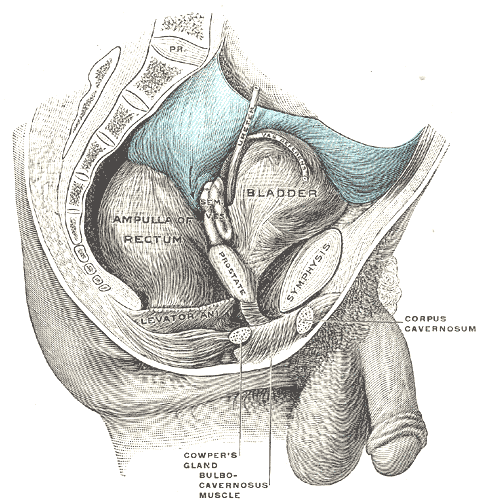
Male pelvic organs seen from right side.
-
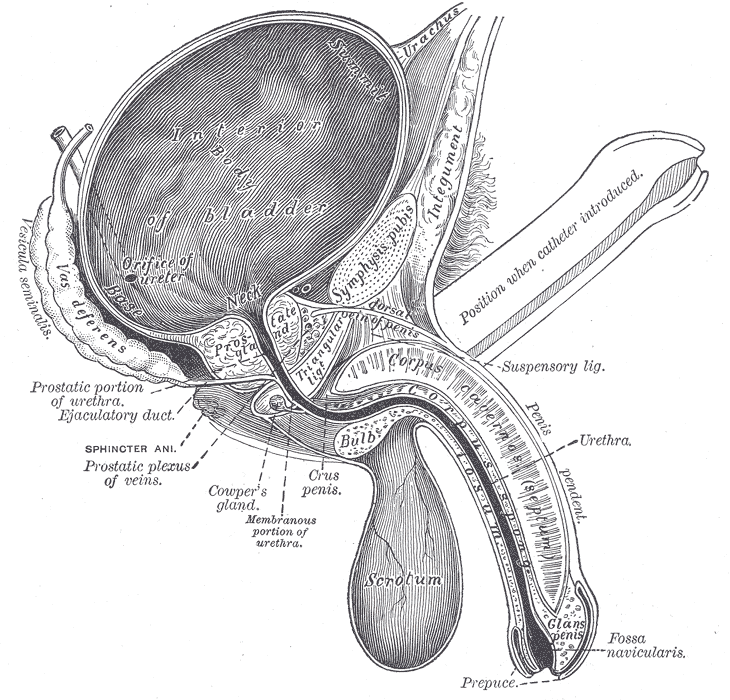
Vertical section of bladder, penis, and urethra.
-
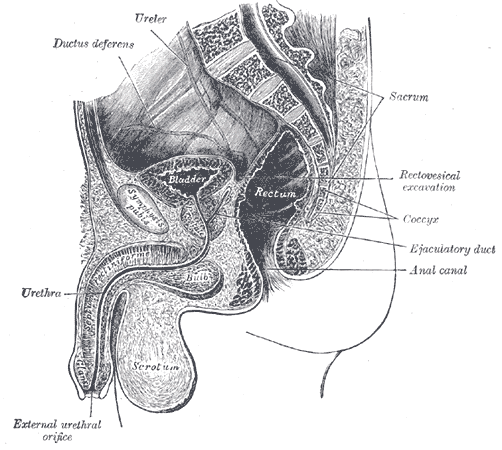
Median sagittal section of male pelvis.
-
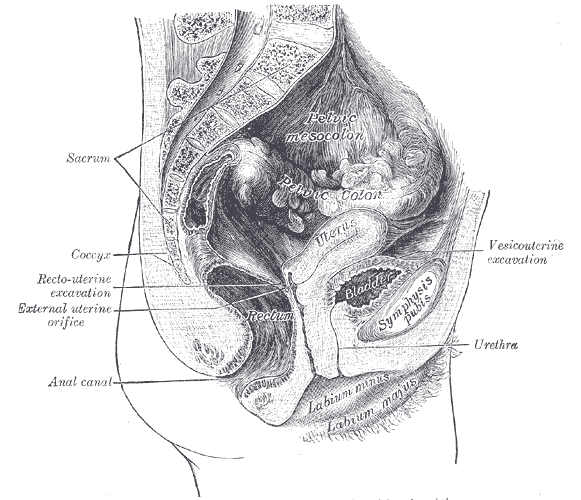
Median sagittal section of female pelvis.
-








References
- ↑ Nutrition pathways to the symphysis pubis J Anat. 2004 March; 204(3): 209–215. doi: 10.1111/j.0021-8782.2004.00271.x. Rodrigo Carvalho Gonçalves da Rocha, Renato Paulo Chopard.
- ↑ Pubic symphysis separation. Fetal and Maternal Medicine Review (2002), 13: 141-155Kelly Owens, Anne Pearson, Gerald Mason.
- ↑ Pubic Symphysial Diastasis During Normal Vaginal Delivery J Obste India Vol.55 No.4 July/August 2005 pgs:365-366 http://medind.nic.in/jaq/t05/i4/jaqt05i4p365.pdf
- ↑ Epidural analgesia for acute symphysis pubis dysfunction in the second trimester. Int J Obstet Anesth. 2004 Jan;13(1):50-2. Scicluna JK, Alderson JD, Webster VJ, Whiting P.
- ↑ Symphysis Pubis Dysfunction-A Cause of Significant Obstetric Morbidity. Eur J Obstet Gynecol Reprod Biol. 2002 Nov 15;105(2):143-6.Owens K, Pearson A, Mason
- ↑ Obstetrics and Gynaecology in The Tropics and Developing Countries. JB Lawson, Professor of Obstetrics and Gynaecology, University of Ibadan, Nigeria; DB Stewart, Professor of Obstetrics and Gynaecology, University of The West Indies, Jamaica
- ↑ Symphysiotomy. A thought-provoking example of appropriate technique in the Third World. Tidsskr Nor Laegeforen 1997 Apr 10; 117(9): 1301-3Institutt for Internasjonal helse, Blindern, Oslo. HL Ersdal, S Bergstrom
- ↑ The Symphysis Pubis: Anatomic and Pathologic Considerations . Clinical Orthopaedics and Related Research 1986 Feb; No. 203; 261-272 JG Gamble MD,SC Simmons.
- ↑ Three dimensional Quantitative Analyses of Human Pubic Symphyseal Morphology: Can Current Limitations of Skeletal Aging Methods be Resolved. MW Tocheri, A Razdan, TL Dupras, M Bae, D Liu.[1]
See also
External links
- Template:EMedicineDictionary
- Template:SUNYAnatomyLabs - "Major Joints of the Lower Extremity - hip and sacrum (anterior view)"
- Template:SUNYAnatomyLabs - "The Male Pelvis: Hemisection of the Male Pelvis"
- Template:ViennaCrossSection