Osimertinib: Difference between revisions
No edit summary |
No edit summary |
||
| Line 5: | Line 5: | ||
|drugClass=kinase inhibitor of the epidermal growth factor receptor (EGFR) | |drugClass=kinase inhibitor of the epidermal growth factor receptor (EGFR) | ||
|indicationType=treatment | |indicationType=treatment | ||
|indication=Osimertinib is indicated for the treatment of patients with metastatic epidermal growth factor receptor (EGFR) T790M mutation-positive non-small cell lung cancer (NSCLC), as detected by an FDA-approved test, who have progressed on or after EGFR tyrosine kinase inhibitor (TKI) therapy. | |indication=Osimertinib is indicated for the treatment of patients with metastatic [[epidermal growth factor receptor (EGFR)]] T790M mutation-positive [[non-small cell lung cancer]] (NSCLC), as detected by an FDA-approved test, who have progressed on or after [[EGFR]] [[tyrosine kinase inhibitor]] (TKI) therapy. | ||
This indication is approved under accelerated approval based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. | This indication is approved under accelerated approval based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. | ||
|adverseReactions= | |adverseReactions=The most common (>20%) adverse reactions (all grades) observed in Osimertinib-treated patients were [[diarrhea]] (42%), [[rash]] (41%), dry [[skin]] (31%), and nail toxicity (25%). | ||
|blackBoxWarningTitle='''<span style="color:#FF0000;">TITLE</span>''' | |blackBoxWarningTitle='''<span style="color:#FF0000;">TITLE</span>''' | ||
|blackBoxWarningBody=''<span style="color:#FF0000;">Condition Name:</span>'' (Content) | |blackBoxWarningBody=''<span style="color:#FF0000;">Condition Name:</span>'' (Content) | ||
|fdaLIADAdult=Osimertinib | |fdaLIADAdult=Osimertinib | ||
Patient Selection | '''Patient Selection''' | ||
Confirm the presence of a T790M EGFR mutation in tumor or, in the absence of tumor, plasma specimens prior to initiation of treatment with Osimertinib. Testing for the presence of the mutation in plasma specimens is recommended only in patients for whom a tumor biopsy cannot be obtained. If this mutation is not detected in a plasma specimen, re-evaluate the feasibility of biopsy for tumor tissue testing. Information on FDA-approved tests for the detection of T790M mutations is available at HTTP://WWW.FDA.GOV/COMPANIONDIAGNOSTICS. | *Confirm the presence of a T790M [[EGFR]] [[mutation]] in [[tumor]] or, in the absence of tumor, [[plasma]] specimens prior to initiation of treatment with Osimertinib. Testing for the presence of the [[mutation]] in [[plasma]] specimens is recommended only in patients for whom a tumor biopsy cannot be obtained. If this [[mutation]] is not detected in a plasma specimen, re-evaluate the feasibility of [[biopsy]] for tumor tissue testing. Information on FDA-approved tests for the detection of T790M mutations is available at HTTP://WWW.FDA.GOV/COMPANIONDIAGNOSTICS. | ||
Recommended Dosage Regimen | '''Recommended Dosage Regimen''' | ||
The recommended dose of Osimertinib is 80 mg tablet once a day until disease progression or unacceptable toxicity. Osimertinib can be taken with or without food. | *The recommended dose of Osimertinib is 80 mg tablet once a day until disease progression or unacceptable toxicity. Osimertinib can be taken with or without food. | ||
If a dose of Osimertinib is missed, do not make up the missed dose and take the next dose as scheduled. | *If a dose of Osimertinib is missed, do not make up the missed dose and take the next dose as scheduled. | ||
Administration to Patients Who Have Difficulty Swallowing Solids | '''Administration to Patients Who Have Difficulty Swallowing Solids''' | ||
Disperse tablet in 60 mL (2 ounces) of non-carbonated water only. Stir until tablet is dispersed into small pieces (the tablet will not completely dissolve) and swallow immediately. Do not crush, heat, or ultrasonicate during preparation. Rinse the container with 120 mL to 240 mL (4 to 8 ounces) of water and immediately drink. | *Disperse [[tablet]] in 60 mL (2 ounces) of non-carbonated water only. Stir until tablet is dispersed into small pieces (the tablet will not completely dissolve) and swallow immediately. Do not crush, heat, or ultrasonicate during preparation. Rinse the container with 120 mL to 240 mL (4 to 8 ounces) of water and immediately drink. | ||
If administration via naso-gastric tube is required, disperse the tablet as above in 15 mL of non-carbonated water, and then use an additional 15 mL of water to transfer any residues to the syringe. The resulting 30 mL liquid should be administered as per the nasogastric tube instructions with appropriate water flushes (approximately 30 mL). | *If administration via naso-gastric tube is required, disperse the tablet as above in 15 mL of non-carbonated water, and then use an additional 15 mL of water to transfer any residues to the syringe. The resulting 30 mL liquid should be administered as per the nasogastric tube instructions with appropriate water flushes (approximately 30 mL). | ||
'''Dosage Modification''' | |||
[[File:Recommended dose modifications ose.png]] | [[File:Recommended dose modifications ose.png]] | ||
|offLabelAdultGuideSupport=There is limited information regarding ''Off-Label Guideline-Supported Use'' of Osimertinib in adult patients. | |offLabelAdultGuideSupport=There is limited information regarding ''Off-Label Guideline-Supported Use'' of Osimertinib in adult patients. | ||
|offLabelAdultNoGuideSupport=There is limited information regarding ''Off-Label Non–Guideline-Supported Use'' of Osimertinib in adult patients. | |offLabelAdultNoGuideSupport=There is limited information regarding ''Off-Label Non–Guideline-Supported Use'' of Osimertinib in adult patients. | ||
|fdaLIADPed=The safety and effectiveness of Osimertinib in pediatric patients have not been established. | |fdaLIADPed=* The safety and effectiveness of Osimertinib in pediatric patients have not been established. | ||
|offLabelPedGuideSupport=There is limited information regarding ''Off-Label Guideline-Supported Use'' of Osimertinib in pediatric patients. | |offLabelPedGuideSupport=There is limited information regarding ''Off-Label Guideline-Supported Use'' of Osimertinib in pediatric patients. | ||
|offLabelPedNoGuideSupport=There is limited information regarding ''Off-Label Non–Guideline-Supported Use'' of Osimertinib in pediatric patients. | |offLabelPedNoGuideSupport=There is limited information regarding ''Off-Label Non–Guideline-Supported Use'' of Osimertinib in pediatric patients. | ||
|contraindications=None | |contraindications=*None | ||
|warnings=Interstitial Lung Disease/Pneumonitis | |warnings='''Interstitial Lung Disease/Pneumonitis''' | ||
Across clinical trials, interstitial lung disease (ILD)/pneumonitis occurred in 3.3% (n=27) of Osimertinib treated patients (n=813); 0.5% (n=4) were fatal | * Across clinical trials, [[interstitial lung disease]] (ILD)/[[pneumonitis]] occurred in 3.3% (n=27) of Osimertinib treated patients (n=813); 0.5% (n=4) were fatal. | ||
*Withhold Osimertinib and promptly investigate for ILD in any patient who presents with worsening of respiratory symptoms which may be indicative of ILD (e.g., [[dyspnea]], [[cough]] and [[fever]]). Permanently discontinue Osimertinib if ILD is confirmed. | |||
'''QTc Interval Prolongation''' | |||
*The heart rate-corrected [[QT]] ([[QTc]]) interval prolongation occurs in patients treated with Osimertinib. Of the 411 patients in Study 1 and Study 2, one patient (0.2%) was found to have a [[QTc]] greater than 500 msec, and 11 patients (2.7%) had an increase from baseline [[QTc]] greater than 60 msec. | |||
*In Study 1 and 2, patients with baseline [[QTc]] of 470 msec or greater were excluded. Conduct periodic monitoring with [[ECGs]] and [[electrolytes]] in patients with congenital [[long QTc syndrome]], [[congestive heart failure]], electrolyte abnormalities, or those who are taking medications known to prolong the [[QTc interval]]. Permanently discontinue Osimertinib in patients who develop [[QTc interval]]prolongation with signs/symptoms of life-threatening [[arrhythmia]]. | |||
'''Cardiomyopathy''' | |||
*Across clinical trials, [[cardiomyopathy]] (defined as [[cardiac failure]], [[pulmonary edema]], [[ejection fraction]] decreased or [[stress cardiomyopathy]]) occurred in 1.4% (n=11) of Osimertinib treated patients (n=813); 0.2% (n=2) were fatal. | |||
*In Study 1 and Study 2, [[Left Ventricular]] [[Ejection Fraction]] (LVEF) decline >10% and a drop to <50% occurred in 2.4% (9/375) of patients who had baseline and at least one follow-up [[LVEF]] assessment. | |||
*Assess LVEF by [[echocardiogram]] or multigated acquisition ([[MUGA]]) scan before initiation of Osimertinib and then at 3 month intervals while on treatment. Withhold treatment with Osimertinib if [[ejection fraction]] decreases by 10% from pretreatment values and is less than 50%. For symptomatic [[congestive heart failure]] or persistent, asymptomatic [[LV dysfunction]] that does not resolve within 4 weeks, permanently discontinue Osimertinib. | |||
'''Embryo-Fetal Toxicity''' | |||
*Based on data from animal studies and its mechanism of action, Osimertinib can cause [[fetal]] harm when administered to a [[pregnant]] woman. In animal reproduction studies, osimertinib caused post-[[implantation]] [[fetal]] loss when administered during early development at a dose exposure 1.5 times the exposure at the recommended human dose. When males were treated prior to mating with untreated females, there was an increase in preimplantation [[embryonic]] loss at [[plasma]] exposures of approximately 0.5-times those observed in patients at the 80 mg dose level. | |||
Advise females of reproductive potential to use effective contraception during treatment with Osimertinib and for 6 weeks after the final dose. Advise males with female partners of reproductive potential to use effective contraception for 4 months after the final dose | '''Advise pregnant women of the potential risk to a fetus.''' | ||
|clinicalTrials=Clinical Trials Experience | *Advise females of reproductive potential to use effective [[contraception]] during treatment with Osimertinib and for 6 weeks after the final dose. Advise males with female partners of [[reproductive]] potential to use effective [[contraception]] for 4 months after the final dose | ||
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. | |clinicalTrials='''Clinical Trials Experience''' | ||
*Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. | |||
The data described below reflect exposure to Osimertinib(80 mg daily) in 411 patients with EGFR T790M mutation-positive non-small cell lung cancer who received prior EGFR TKI therapy, in two single-arm studies, Study 1 and Study 2. Patients with a past medical history of ILD or radiation pneumonitis that required steroid treatment, serious arrhythmia or baseline QTc interval greater than 470 ms were excluded from Study 1 and Study 2. Baseline patient and disease characteristics were: median age 63 years, 13% of patients were ≥75 years old, female (68%), White (36%), Asian (60%), metastatic (96%), sites of brain metastases (39%), World Health Organization (WHO) performance status of 0 (37%) or 1 (63%), 1 prior line of therapy [EGFR-TKI treatment only, second line, chemotherapy-naïve (31%)], 2 or more prior lines of therapy (69%). Of the 411 patients, 333 patients were exposed to Osimertinib for at least 6 months; 97 patients were exposed for at least 9 months; however, no patient was exposed to Osimertinib for 12 months. | *The data described below reflect exposure to Osimertinib(80 mg daily) in 411 patients with [[EGFR]] T790M mutation-positive non-small cell lung cancer who received prior [[EGFR]] TKI therapy, in two single-arm studies, Study 1 and Study 2. Patients with a past medical history of ILD or [[radiation pneumonitis]] that required [[steroid]] treatment, serious [[arrhythmia]] or baseline [[QTc interval]] greater than 470 ms were excluded from Study 1 and Study 2. Baseline patient and disease characteristics were: [[median]] age 63 years, 13% of patients were ≥75 years old, female (68%), White (36%), Asian (60%), metastatic (96%), sites of [[brain metastases]] (39%), World Health Organization (WHO) performance status of 0 (37%) or 1 (63%), 1 prior line of therapy [EGFR-TKI treatment only, second line, chemotherapy-naïve (31%)], 2 or more prior lines of therapy (69%). Of the 411 patients, 333 patients were exposed to Osimertinib for at least 6 months; 97 patients were exposed for at least 9 months; however, no patient was exposed to Osimertinib for 12 months. | ||
In Studies 1 and 2, the most common (>20%) adverse reactions (all grades) observed in Osimertinib-treated patients were diarrhea (42%), rash (41%), dry skin (31%), and nail toxicity (25%). Dose reductions occurred in 4.4% of patients treated with Osimertinib. The most frequent adverse reactions that led to dose reductions or interruptions were: electrocardiogram QTc prolonged (2.2%) and neutropenia (1.9%). Serious adverse reactions reported in 2% or more patients were pneumonia and pulmonary embolus. There were 4 patients (1%) treated with Osimertinib who developed fatal adverse reactions of ILD/pneumonitis. Other fatal adverse reactions occurring in more than 1 patient included pneumonia (4 patients) and CVA/cerebral hemorrhage (2 patients). Discontinuation of therapy due to adverse reactions occurred in 5.6% of patients treated with Osimertinib. The most frequent adverse reactions that led to discontinuation were ILD/pneumonitis and cerebrovascular accidents/infarctions. | *In Studies 1 and 2, the most common (>20%) adverse reactions (all grades) observed in Osimertinib-treated patients were [[diarrhea]] (42%), [[rash]] (41%), dry skin (31%), and nail toxicity (25%). Dose reductions occurred in 4.4% of patients treated with Osimertinib. The most frequent adverse reactions that led to dose reductions or interruptions were: electrocardiogram [[QTc prolonged]] (2.2%) and [[neutropenia]] (1.9%). Serious adverse reactions reported in 2% or more patients were [[pneumonia]] and [[pulmonary embolus]]. There were 4 patients (1%) treated with Osimertinib who developed fatal adverse reactions of ILD/[[pneumonitis]]. Other fatal adverse reactions occurring in more than 1 patient included [[pneumonia]] (4 patients) and [[CVA]]/[[cerebral hemorrhage]] (2 patients). Discontinuation of therapy due to adverse reactions occurred in 5.6% of patients treated with Osimertinib. The most frequent adverse reactions that led to discontinuation were ILD/[[pneumonitis]] and cerebrovascular accidents/infarctions. | ||
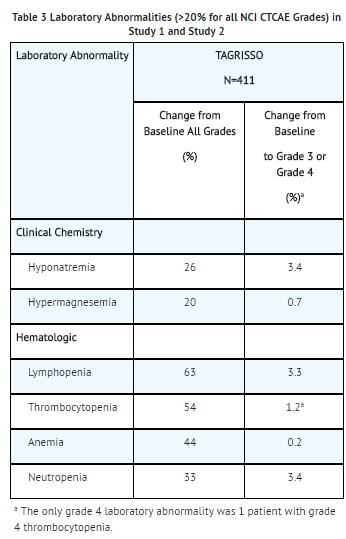
Tables 2 and 3 summarize the common adverse reactions and laboratory abnormalities observed in Osimertinib-treated patients. | Tables 2 and 3 summarize the common adverse reactions and laboratory abnormalities observed in Osimertinib-treated patients. | ||
[[File:Adverse reactions ose.png]][[File:Laboraory abnomralities ose.png]] | '''Adverse reactions''' | ||
|drugInteractions= | [[File:Adverse reactions ose.png]] | ||
Strong CYP3A Inducers | '''Laboratory abormalities''' | ||
[[File:Laboraory abnomralities ose.png]] | |||
Coadministering Osimertinib with a strong CYP3A4 inducer decreased the exposure of osimertinib compared to administering Osimertinib alone | |drugInteractions='''Effect of Other Drugs on Osimertinib''' | ||
*Strong [[CYP3A]] Inducers | |||
Coadministering Osimertinib with a strong [[CYP3A4]] inducer decreased the exposure of osimertinib compared to administering Osimertinib alone. Decreased osimertinib exposure may lead to reduced efficacy. | |||
*Avoid coadministering Osimertinib with strong [[CYP3A]] inducers (e.g., [[phenytoin]], [[rifampin]], [[carbamazepine]], [[St. John’s Wort]]) [note: effect of St. John’s Wort varies widely and is preparation-dependent]. Increase the Osimertinib dosage when coadministering with a strong [[CYP3A4]] inducer if concurrent use is unavoidable. No dose adjustments are required when Osimertinib is used with moderate and/or weak CYP3A inducers. | |||
''' | |||
Effect of Osimertinib on Other Drugs''' | |||
*Coadministering Osimertinib with a BCRP substrate increased the exposure of the BCRP substrate compared to administering the BCRP substrate alone. Increased BCRP substrate exposure may increase the risk of exposure-related toxicity. | |||
Effect of Other Drugs on Osimertinib in Clinical Pharmacokinetic Studies | *Monitor for adverse reactions of the BCRP substrate (e.g., [[rosuvastatin]], [[sulfasalazine]], [[topotecan]]), unless otherwise instructed in its approved labeling, when coadministered with Osimertinib. | ||
''' | |||
Drug Interactions''' | |||
''' | |||
Effect of Other Drugs on Osimertinib in Clinical Pharmacokinetic Studies''' | |||
Strong CYP3A Inducers | '''Strong CYP3A Inducers''' | ||
*The steady-state AUC of osimertinib was reduced by 78% in patients when coadministered with [[rifampin]] (600 mg daily for 21 days) in a clinical pharmacokinetic study. | |||
Strong CYP3A Inhibitors: Coadministering Osimertinib with 200 mg itraconazole twice daily (a strong CYP3A4 inhibitor) had no clinically significant effect on the exposure of osimertinib (AUC increased by 24% and Cmax decreased by 20%). | '''Strong CYP3A Inhibitors''': | ||
*Coadministering Osimertinib with 200 mg itraconazole twice daily (a strong CYP3A4 inhibitor) had no clinically significant effect on the exposure of osimertinib (AUC increased by 24% and Cmax decreased by 20%). | |||
Gastric Acid Reducing Agents: The exposure of osimertinib was not affected by concurrent administration of a single 80 mg Osimertinib tablet following 40 mg omeprazole administration for 5 days. | Gastric Acid Reducing Agents: The exposure of osimertinib was not affected by concurrent administration of a single 80 mg Osimertinib tablet following 40 mg omeprazole administration for 5 days. | ||
Revision as of 15:08, 16 February 2017
{{DrugProjectFormSinglePage |authorTag=Vishal Devarkonda, M.B.B.S[1] |genericName=Osimertinib |aOrAn=a |drugClass=kinase inhibitor of the epidermal growth factor receptor (EGFR) |indicationType=treatment |indication=Osimertinib is indicated for the treatment of patients with metastatic epidermal growth factor receptor (EGFR) T790M mutation-positive non-small cell lung cancer (NSCLC), as detected by an FDA-approved test, who have progressed on or after EGFR tyrosine kinase inhibitor (TKI) therapy.
This indication is approved under accelerated approval based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. |adverseReactions=The most common (>20%) adverse reactions (all grades) observed in Osimertinib-treated patients were diarrhea (42%), rash (41%), dry skin (31%), and nail toxicity (25%). |blackBoxWarningTitle=TITLE |blackBoxWarningBody=Condition Name: (Content) |fdaLIADAdult=Osimertinib Patient Selection
- Confirm the presence of a T790M EGFR mutation in tumor or, in the absence of tumor, plasma specimens prior to initiation of treatment with Osimertinib. Testing for the presence of the mutation in plasma specimens is recommended only in patients for whom a tumor biopsy cannot be obtained. If this mutation is not detected in a plasma specimen, re-evaluate the feasibility of biopsy for tumor tissue testing. Information on FDA-approved tests for the detection of T790M mutations is available at HTTP://WWW.FDA.GOV/COMPANIONDIAGNOSTICS.
Recommended Dosage Regimen
- The recommended dose of Osimertinib is 80 mg tablet once a day until disease progression or unacceptable toxicity. Osimertinib can be taken with or without food.
- If a dose of Osimertinib is missed, do not make up the missed dose and take the next dose as scheduled.
Administration to Patients Who Have Difficulty Swallowing Solids
- Disperse tablet in 60 mL (2 ounces) of non-carbonated water only. Stir until tablet is dispersed into small pieces (the tablet will not completely dissolve) and swallow immediately. Do not crush, heat, or ultrasonicate during preparation. Rinse the container with 120 mL to 240 mL (4 to 8 ounces) of water and immediately drink.
- If administration via naso-gastric tube is required, disperse the tablet as above in 15 mL of non-carbonated water, and then use an additional 15 mL of water to transfer any residues to the syringe. The resulting 30 mL liquid should be administered as per the nasogastric tube instructions with appropriate water flushes (approximately 30 mL).
Dosage Modification
 |offLabelAdultGuideSupport=There is limited information regarding Off-Label Guideline-Supported Use of Osimertinib in adult patients.
|offLabelAdultNoGuideSupport=There is limited information regarding Off-Label Non–Guideline-Supported Use of Osimertinib in adult patients.
|fdaLIADPed=* The safety and effectiveness of Osimertinib in pediatric patients have not been established.
|offLabelPedGuideSupport=There is limited information regarding Off-Label Guideline-Supported Use of Osimertinib in pediatric patients.
|offLabelPedNoGuideSupport=There is limited information regarding Off-Label Non–Guideline-Supported Use of Osimertinib in pediatric patients.
|contraindications=*None
|warnings=Interstitial Lung Disease/Pneumonitis
|offLabelAdultGuideSupport=There is limited information regarding Off-Label Guideline-Supported Use of Osimertinib in adult patients.
|offLabelAdultNoGuideSupport=There is limited information regarding Off-Label Non–Guideline-Supported Use of Osimertinib in adult patients.
|fdaLIADPed=* The safety and effectiveness of Osimertinib in pediatric patients have not been established.
|offLabelPedGuideSupport=There is limited information regarding Off-Label Guideline-Supported Use of Osimertinib in pediatric patients.
|offLabelPedNoGuideSupport=There is limited information regarding Off-Label Non–Guideline-Supported Use of Osimertinib in pediatric patients.
|contraindications=*None
|warnings=Interstitial Lung Disease/Pneumonitis
- Across clinical trials, interstitial lung disease (ILD)/pneumonitis occurred in 3.3% (n=27) of Osimertinib treated patients (n=813); 0.5% (n=4) were fatal.
- Withhold Osimertinib and promptly investigate for ILD in any patient who presents with worsening of respiratory symptoms which may be indicative of ILD (e.g., dyspnea, cough and fever). Permanently discontinue Osimertinib if ILD is confirmed.
QTc Interval Prolongation
- The heart rate-corrected QT (QTc) interval prolongation occurs in patients treated with Osimertinib. Of the 411 patients in Study 1 and Study 2, one patient (0.2%) was found to have a QTc greater than 500 msec, and 11 patients (2.7%) had an increase from baseline QTc greater than 60 msec.
- In Study 1 and 2, patients with baseline QTc of 470 msec or greater were excluded. Conduct periodic monitoring with ECGs and electrolytes in patients with congenital long QTc syndrome, congestive heart failure, electrolyte abnormalities, or those who are taking medications known to prolong the QTc interval. Permanently discontinue Osimertinib in patients who develop QTc intervalprolongation with signs/symptoms of life-threatening arrhythmia.
Cardiomyopathy
- Across clinical trials, cardiomyopathy (defined as cardiac failure, pulmonary edema, ejection fraction decreased or stress cardiomyopathy) occurred in 1.4% (n=11) of Osimertinib treated patients (n=813); 0.2% (n=2) were fatal.
- In Study 1 and Study 2, Left Ventricular Ejection Fraction (LVEF) decline >10% and a drop to <50% occurred in 2.4% (9/375) of patients who had baseline and at least one follow-up LVEF assessment.
- Assess LVEF by echocardiogram or multigated acquisition (MUGA) scan before initiation of Osimertinib and then at 3 month intervals while on treatment. Withhold treatment with Osimertinib if ejection fraction decreases by 10% from pretreatment values and is less than 50%. For symptomatic congestive heart failure or persistent, asymptomatic LV dysfunction that does not resolve within 4 weeks, permanently discontinue Osimertinib.
Embryo-Fetal Toxicity
- Based on data from animal studies and its mechanism of action, Osimertinib can cause fetal harm when administered to a pregnant woman. In animal reproduction studies, osimertinib caused post-implantation fetal loss when administered during early development at a dose exposure 1.5 times the exposure at the recommended human dose. When males were treated prior to mating with untreated females, there was an increase in preimplantation embryonic loss at plasma exposures of approximately 0.5-times those observed in patients at the 80 mg dose level.
Advise pregnant women of the potential risk to a fetus.
- Advise females of reproductive potential to use effective contraception during treatment with Osimertinib and for 6 weeks after the final dose. Advise males with female partners of reproductive potential to use effective contraception for 4 months after the final dose
|clinicalTrials=Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
- The data described below reflect exposure to Osimertinib(80 mg daily) in 411 patients with EGFR T790M mutation-positive non-small cell lung cancer who received prior EGFR TKI therapy, in two single-arm studies, Study 1 and Study 2. Patients with a past medical history of ILD or radiation pneumonitis that required steroid treatment, serious arrhythmia or baseline QTc interval greater than 470 ms were excluded from Study 1 and Study 2. Baseline patient and disease characteristics were: median age 63 years, 13% of patients were ≥75 years old, female (68%), White (36%), Asian (60%), metastatic (96%), sites of brain metastases (39%), World Health Organization (WHO) performance status of 0 (37%) or 1 (63%), 1 prior line of therapy [EGFR-TKI treatment only, second line, chemotherapy-naïve (31%)], 2 or more prior lines of therapy (69%). Of the 411 patients, 333 patients were exposed to Osimertinib for at least 6 months; 97 patients were exposed for at least 9 months; however, no patient was exposed to Osimertinib for 12 months.
- In Studies 1 and 2, the most common (>20%) adverse reactions (all grades) observed in Osimertinib-treated patients were diarrhea (42%), rash (41%), dry skin (31%), and nail toxicity (25%). Dose reductions occurred in 4.4% of patients treated with Osimertinib. The most frequent adverse reactions that led to dose reductions or interruptions were: electrocardiogram QTc prolonged (2.2%) and neutropenia (1.9%). Serious adverse reactions reported in 2% or more patients were pneumonia and pulmonary embolus. There were 4 patients (1%) treated with Osimertinib who developed fatal adverse reactions of ILD/pneumonitis. Other fatal adverse reactions occurring in more than 1 patient included pneumonia (4 patients) and CVA/cerebral hemorrhage (2 patients). Discontinuation of therapy due to adverse reactions occurred in 5.6% of patients treated with Osimertinib. The most frequent adverse reactions that led to discontinuation were ILD/pneumonitis and cerebrovascular accidents/infarctions.
Tables 2 and 3 summarize the common adverse reactions and laboratory abnormalities observed in Osimertinib-treated patients.
Adverse reactions
 Laboratory abormalities
Laboratory abormalities

|drugInteractions=Effect of Other Drugs on Osimertinib
- Strong CYP3A Inducers
Coadministering Osimertinib with a strong CYP3A4 inducer decreased the exposure of osimertinib compared to administering Osimertinib alone. Decreased osimertinib exposure may lead to reduced efficacy.
- Avoid coadministering Osimertinib with strong CYP3A inducers (e.g., phenytoin, rifampin, carbamazepine, St. John’s Wort) [note: effect of St. John’s Wort varies widely and is preparation-dependent]. Increase the Osimertinib dosage when coadministering with a strong CYP3A4 inducer if concurrent use is unavoidable. No dose adjustments are required when Osimertinib is used with moderate and/or weak CYP3A inducers.
Effect of Osimertinib on Other Drugs
- Coadministering Osimertinib with a BCRP substrate increased the exposure of the BCRP substrate compared to administering the BCRP substrate alone. Increased BCRP substrate exposure may increase the risk of exposure-related toxicity.
- Monitor for adverse reactions of the BCRP substrate (e.g., rosuvastatin, sulfasalazine, topotecan), unless otherwise instructed in its approved labeling, when coadministered with Osimertinib.
Drug Interactions Effect of Other Drugs on Osimertinib in Clinical Pharmacokinetic Studies
Strong CYP3A Inducers
- The steady-state AUC of osimertinib was reduced by 78% in patients when coadministered with rifampin (600 mg daily for 21 days) in a clinical pharmacokinetic study.
Strong CYP3A Inhibitors:
- Coadministering Osimertinib with 200 mg itraconazole twice daily (a strong CYP3A4 inhibitor) had no clinically significant effect on the exposure of osimertinib (AUC increased by 24% and Cmax decreased by 20%).
Gastric Acid Reducing Agents: The exposure of osimertinib was not affected by concurrent administration of a single 80 mg Osimertinib tablet following 40 mg omeprazole administration for 5 days.
Effect of Osimertinib on Other Drugs in Clinical Pharmacokinetic Studies
BCRP substrates: Coadministering Osimertinib with rosuvastatin (a BCRP substrate) increased rosuvastatin AUC by 35% and Cmax by 72% in a clinical pharmacokinetic study [see DRUG INTERACTIONS (7.2)].
CYP3A4 substrates: Coadministering Osimertinib with simvastatin (a CYP3A4 substrate) had no clinically significant effect on the exposure of simvastatin in a clinical pharmacokinetic study.
In Vitro Studies
CYP450 Metabolic Pathways: Osimertinib does not inhibit CYP1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6 and 2E1. Osimertinib induced CYP1A2 enzymes.
Transporter Systems: Osimertinib is a substrate of P-glycoprotein and BCRP and is not a substrate of OATP1B1 and OATP1B3. Osimertinib is an inhibitor of BCRP and does not inhibit P-glycoprotein, OAT1, OAT3, OATP1B1, OATP1B3, MATE1, MATE2K and OCT2. |useInPregnancyFDA=Pregnancy Risk Summary
Based on data from animal studies and its mechanism of action, Osimertinib can cause fetal harm when administered to a pregnant woman. There are no available data on Osimertinib use in pregnant women. Administration of osimertinib to pregnant rats was associated with embryolethality and reduced fetal growth at plasma exposures 1.5 times the exposure at the recommended human dose [see DATA]. Advise pregnant women of the potential risk to a fetus.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically-recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
When administered to pregnant rats prior to embryonic implantation through the end of organogenesis (gestation days 2-20) at a dose of 20 mg/kg/day, which produced plasma exposures of approximately 1.5 times the clinical exposure, osimertinib caused post-implantation loss and early embryonic death. When administered to pregnant rats from implantation through the closure of the hard palate (gestation days 6 to 16) at doses of 1 mg/kg/day and above (0.1-times the AUC observed in patients at the recommended dose of 80 mg), an equivocal increase in the rate of fetal malformations and variations was observed in treated litters relative to those of concurrent controls. When administered to pregnant dams at doses of 30 mg/kg/day during organogenesis through lactation Day 6, osimertinib caused an increase in total litter loss and postnatal death. At a dose of 20 mg/kg/day, osimertinib administration during the same period resulted in increased postnatal death as well as a slight reduction in mean pup weight at birth that increased in magnitude between lactation days 4 and 6. |useInPed=The safety and effectiveness of Osimertinib in pediatric patients have not been established. |useInGeri=Geriatric Use One hundred eighty-seven (45%) of the 411 patients in clinical trials of Osimertinib were 65 years of age and older, and 54 patients (13%) were 75 years of age and older. No overall differences in effectiveness were observed based on age. Exploratory analysis suggests a higher incidence of Grade 3 and 4 adverse reactions (32% versus 25%) and more frequent dose modifications for adverse reactions (23% versus 17%) in patients 65 years or older as compared to those younger than 65 years. |useInRenalImpair=Renal Impairment No dose adjustment is recommended in patients with mild [creatinine clearance (CLcr) 60-89 mL/min, as estimated by the Cockcroft Gault method (C-G)] or moderate (CLcr 30-59 mL/min, as estimated by C-G) renal impairment. There is no recommended dose of Osimertinib for patients with severe renal impairment (CLcr <30 mL/min) or end-stage renal disease |useInHepaticImpair=Hepatic Impairment No dose adjustment is recommended in patients with mild hepatic impairment [total bilirubin less than or equal to upper limit of normal (ULN) and AST greater than ULN or total bilirubin between 1.0 to 1.5 times ULN and any AST]. There is no recommended dose for Osimertinib for patients with moderate or severe hepatic impairment |useInReproPotential=Females and Males of Reproductive Potential Contraception
Females
Advise females of reproductive potential to use effective contraception during treatment with Osimertinib and for 6 weeks after the final dose.
Males
Advise male patients with female partners of reproductive potential to use effective contraception during and for 4 months following the final dose of Osimertinib.
Infertility
Based on animal studies, Osimertinib may impair fertility in females and males of reproductive potential. The effects on female fertility showed a trend toward reversibility. It is not known whether the effects on male fertility are reversible. |othersTitle=Lactation |useInOthers=There are no data on the presence of osimertinib in human milk, the effects of osimertinib on the breastfed infant or on milk production. Administration to rats during gestation and early lactation was associated with adverse effects, including reduced growth rates and neonatal death [see USE IN SPECIFIC POPULATIONS (8.1)]. Because of the potential for serious adverse reactions in breastfed infants from osimertinib, advise a lactating woman not to breastfeed during treatment with Osimertinib and for 2 weeks after the final dose. |administration=The recommended dose of Osimertinib is 80 mg tablet once a day until disease progression or unacceptable toxicity. Osimertinib can be taken with or without food.
If a dose of Osimertinib is missed, do not make up the missed dose and take the next dose as scheduled. |drugBox={{Drugbox2 | verifiedrevid = | IUPAC_name = N-(2-{2-dimethylaminoethyl-methylamino}-4-methoxy-5-{[4-(1-methylindol-3-yl)pyrimidin-2-yl]amino}phenyl)prop-2-enamide | image = Osimertinib.svg | width = 250
| tradename = Tagrisso, Tagrix | Drugs.com = tagrisso | MedlinePlus = | licence_EU = | licence_US = | pregnancy_US = | legal_UK = | legal_US = Rx-only | routes_of_administration = Oral tablets
| bioavailability = | protein_bound = Probably high[1] | metabolism = Oxidation (CYP3A) | elimination_half-life = 48 hours | excretion = Feces (68%), urine (14%)
| IUPHAR_ligand =
| CAS_number_Ref =
| CAS_number = 1421373-65-0
| ATC_prefix = L01
| ATC_suffix = XE35
| PubChem = 71496458
| DrugBank_Ref =
| DrugBank = DB09330
| ChemSpiderID_Ref =
| ChemSpiderID = 31042598
| UNII_Ref =
| UNII = 3C06JJ0Z2O
| KEGG_Ref =
| KEGG = D10766
| ChEMBL_Ref =
| ChEMBL =
| ChEBI_Ref = ![]() | ChEBI = 90943
| synonyms = AZD9291
| ChEBI = 90943
| synonyms = AZD9291
| C = 28 | H = 33 | N = 7 | O = 2
| smiles = CN1C=C(C2=CC=CC=C21)C3=NC(=NC=C3)NC4=C(C=C(C(=C4)NC(=O)C=C)N(C)CCN(C)C)OC
| StdInChI=1S/C28H33N7O2/c1-7-27(36)30-22-16-23(26(37-6)17-25(22)34(4)15-14-33(2)3)32-28-29-13-12-21(31-28)20-18-35(5)24-11-9-8-10-19(20)24/h7-13,16-18H,1,14-15H2,2-6H3,(H,30,36)(H,29,31,32)
| StdInChIKey = DUYJMQONPNNFPI-UHFFFAOYSA-N
| StdInChI_Ref =
| StdInChIKey_Ref =
}}
|mechAction=Osimertinib is a kinase inhibitor of the epidermal growth factor receptor (EGFR), which binds irreversibly to certain mutant forms of EGFR (T790M, L858R, and exon 19 deletion) at approximately 9-fold lower concentrations than wild-type. In cultured cells and animal tumor implantation models, osimertinib exhibited anti-tumor activity against NSCLC lines harboring EGFR-mutations (T790M/L858R, L858R, T790M/exon 19 deletion, and exon 19 deletion) and, to a lesser extent, wild-type EGFR amplifications. Two pharmacologically-active metabolites (AZ7550 and AZ5104 circulating at approximately 10% of the parent) with similar inhibitory profiles to osimertinib have been identified in the plasma after oral administration of osimertinib. AZ7550 showed a similar potency to osimertinib, while AZ5104 showed greater potency against exon 19 deletion and T790M mutants (approximately 8-fold) and wild-type (approximately 15-fold) EGFR. In vitro, osimertinib also inhibited the activity of HER2, HER3, HER4, ACK1, and BLK at clinically relevant concentrations.
|structure=The molecular formula for osimertinib mesylate is C28H33N7O2•CH4O3S, and the molecular weight is 596 g/mol. The chemical name is N-(2-{2-dimethylaminoethyl-methylamino}-4-methoxy-5-{[4-(1-methylindol-3-yl)pyrimidin-2-yl]amino}phenyl)prop-2-enamide mesylate salt. Osimertinib has the following structural formula (as osimertinib mesylate):
 |PD=Cardiac Electrophysiology
|PD=Cardiac Electrophysiology
The QTc interval prolongation potential of osimertinib was assessed in 210 patients who received Osimertinib 80 mg daily in Study 2. A central tendency analysis of the QTcF data at steady-state demonstrated that the maximum mean change from baseline was 16.2 msec (upper bound of two-sided 90% confidence interval (CI) 17.6 msec). A pharmacokinetic/pharmacodynamic analysis in Study 2 suggested a concentration-dependent QTc interval prolongation of 14 msec (upper bound of two-sided 90% CI: 16 msec) at a dose of Osimertinib 80 mg. |PK=Pharmacokinetics The area under the plasma concentration-time curve (AUC) and maximal plasma concentration (Cmax) of osimertinib increased dose proportionally over 20 to 240 mg dose range (i.e., 0.25 to 3 times the recommended dosage) after oral administration and exhibited linear pharmacokinetics (PK). Administration of Osimertinib orally once daily resulted in approximately 3-fold accumulation with steady state exposures achieved after 15 days of dosing. At steady state, the Cmax to Cmin (minimal concentration) ratio was 1.6-fold.
Absorption
The median time to Cmax of osimertinib was 6 hours (range 3-24 hours).
Following administration of a 20 mg Osimertinib tablet with a high-fat, high-calorie meal (containing approximately 58 grams of fat and 1000 calories), the Cmax and AUC of osimertinib were comparable to that under fasting conditions.
Distribution
The mean volume of distribution at steady-state (Vss/F) of osimertinib was 986 L. Plasma protein binding of osimertinib is likely high based on its physiochemical properties.
Elimination
Osimertinib plasma concentrations decreased with time and a population estimated mean half-life of osimertinib was 48 hours, and oral clearance (CL/F) was 14.2 (L/h).
Metabolism
The main metabolic pathways of osimertinib were oxidation (predominantly CYP3A) and dealkylation in vitro. Two pharmacologically active metabolites (AZ7550 and AZ5104) have been identified in the plasma after Osimertinib oral administration. The geometric mean exposure (AUC) of each metabolite (AZ5104 and AZ7550) was approximately 10% of the exposure of osimertinib at steady-state.
Excretion
Osimertinib is primarily eliminated in the feces (68%) and to a lesser extent in the urine (14%). Unchanged osimertinib accounted for approximately 2% of the elimination.
Specific Populations
No clinically significant differences in the pharmacokinetics of osimertinib were observed based on age, sex, ethnicity, body weight, smoking status, mild (CLcr 60-89 mL/min, as estimated by C-G) or moderate (CLcr 30-59 mL/min, as estimated by C-G) renal impairment, or mild hepatic impairment (total bilirubin less than or equal to ULN and AST greater than ULN or total bilirubin between 1 to 1.5 times ULN and any AST). The pharmacokinetics of osimertinib in patients with severe renal impairment (CLcr less than 30 mL/min) or with moderate to severe hepatic impairment (moderate: total bilirubin between 1.5 to 3 times ULN and any AST, and severe: total bilirubin between 3 to 10 times ULN and any AST) are unknown. |nonClinToxic=Carcinogenesis, Mutagenesis, Impairment of Fertility Carcinogenicity studies have not been performed with osimertinib. Osimertinib did not cause genetic damage in in vitro and in vivo assays.
Based on studies in animals, male fertility may be impaired by treatment with Osimertinib. Degenerative changes were present in the testes in rats and dogs exposed to osimertinib for 1 month or more with evidence of reversibility in the rat. Following administration of osimertinib to rats for approximately 10 weeks at a dose of 40 mg/kg, at exposures 0.5-times the AUC observed in patients at the recommended dose of 80 mg, there was a reduction in male fertility, demonstrated by increased pre-implantation loss in untreated females mated to treated males.
Based on studies in animals, female fertility may be impaired by treatment with Osimertinib. In repeat dose toxicity studies, histological evidence of anestrus, corpora lutea degeneration in the ovaries and epithelial thinning in the uterus and vagina were seen in rats exposed to osimertinib for 1 month or more at exposures 0.3-times the AUC observed in patients at the recommended dose of 80 mg. Findings in the ovaries seen following 1 month of dosing exhibited evidence of reversibility. In a female fertility study in rats, administration of osimertinib from 2 weeks prior to mating through Day 8 of gestation at a dose of 20 mg/kg/day (approximately 1.5-times the human Cmax at the recommended dose of 80 mg/day) had no effects on oestrus cycling or the number of females becoming pregnant, but caused early embryonic deaths. These findings showed evidence of reversibility when females were mated 1 month after treatment discontinuation. |clinicalStudies=The efficacy of Osimertinib was demonstrated in two multicenter, single-arm, open-label clinical trials, Study 1 and Study 2, in patients with metastatic EGFR T790M mutation-positive NSCLC who had progressed on prior systemic therapy, including an EGFR TKI. All patients were required to have EGFR T790M mutation-positive NSCLC as detected by the cobas® EGFR mutation test and received Osimertinib 80 mg once daily. The major efficacy outcome measure of both trials was ORR according to RECIST v1.1 as evaluated by a Blinded Independent Central Review (BICR). Duration of response (DOR) was an additional outcome measure.
Study 1 population characteristics were: median age 62 years (range 37 to 89), female (66%), White (38%), Asian (58%), never smoker (67%), WHO performance status 0 (34%) or 1 (66%), adenocarcinoma histology (97%), 1 prior line of therapy [EGFR-TKI treatment only, second line, chemotherapy-naïve] (30%), 2 or more prior lines of therapy (70%). Sites of extra-thoracic metastasis included liver (32%), bone (51%), and brain (37%). Somatic EGFR mutations in addition to T790M were exon 19 deletion (71%), L858R (25%), G719X (2%), and S768I (2%).
Study 2 population characteristics were: median age 64 years (range 35 to 88), female (70%), White (34%), Asian (63%), never smoker (76%), WHO performance status 0 (40%) or 1 (60%), adenocarcinoma histology (95%), 1 prior line of therapy [EGFR-TKI treatment only, second line, chemotherapy-naïve] (32%), 2 or more prior lines of therapy (68%). Sites of extra-thoracic metastasis included liver (26%), bone (43%), and brain (41%). Somatic EGFR mutations in addition to T790M were exon 19 deletion (65%), L858R (32%), G719X (2%), and S768I (1%).
Efficacy results by BICR from Study 1 and Study 2 are summarized in Table 4. The majority (96%) of patients with confirmed objective responses had ongoing responses ranging from 1.1 to 5.6 months after a median duration of follow-up of 4.2 months for Study 1 and 4.0 months for Study 2. |howSupplied=80 mg tablets: beige, oval and biconvex tablet marked with “AZ 80” on one side and plain on the reverse and are available in bottles of 30 (NDC 0310-1350-30).
40 mg tablets: beige, round and biconvex tablet marked with “AZ 40” on one side and plain on the reverse and are available in bottles of 30 (NDC 0310-1349-30).
. |storage=Store Osimertinib bottles at 25°C (77°F). Excursions permitted to 15-30°C (59-86°F) [see USP Controlled Room Temperature]
|packLabel=

|fdaPatientInfo=Advise the patient to read the FDA-approved patient labeling (Patient Information). Interstitial Lung Disease/Pneumonitis Inform patients of the risks of severe or fatal ILD, including pneumonitis. Advise patients to contact their healthcare provider immediately to report new or worsening respiratory symptoms. QTc Interval Prolongation Inform patients of symptoms that may be indicative of significant QTc prolongation including dizziness, lightheadedness, and syncope. Advise patients to report these symptoms and to inform their physician about the use of any heart or blood pressure medications. Cardiomyopathy • Osimertinib can cause cardiomyopathy. Advise patients to immediately report any signs or symptoms of heart failure to their healthcare provider. Embryo-Fetal Toxicity • Osimertinib can cause fetal harm if taken during pregnancy. Advise pregnant women of the potential risk to a fetus. • Advise females to inform their healthcare provider if they become pregnant or if pregnancy is suspected, while taking Osimertinib. Females and Males of Reproductive Potential • Advise females of reproductive potential to use effective contraception during treatment with Osimertinib and for 6 weeks after the final dose • Advise males to use effective contraception during treatment and for 4 months after the final dose of Osimertinib [see Use in Specific Populations (8.3)]. Lactation Advise women not to breastfeed during treatment with Osimertinib and for 2 weeks after the final dose |alcohol=Alcohol-Osimertinib interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication. |brandNames=TAGRISSO }}
- ↑ "Tagrisso (osimertinib) Tablet, for Oral Use. Full Prescribing Information" (PDF). AstraZeneca Pharmaceuticals LP, Wilmington, DE 19850. Retrieved 16 November 2015.