Ofatumumab
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
WARNING
See full prescribing information for complete Boxed Warning.
HEPATITIS B VIRUS (HBV) REACTIVATION AND PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY
|
Overview
Ofatumumab is a CD20-directed cytolytic monoclonal antibody that is FDA approved for the treatment of previously untreated patients with chronic lymphocytic leukemia (CLL) in combination with chlorambucil and patients with CLL refractory to fludarabine and alemtuzumab. There is a Black Box Warning for this drug as shown here. Common adverse reactions include infusion reactions, neutropenia, pneumonia, pyrexia, cough, diarrhea, anemia, fatigue, dyspnea, rash, nausea, bronchitis, and upper respiratory tract infections.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Previously Untreated Chronic Lymphocytic Leukemia
- ARZERRA (ofatumumab) is indicated, in combination with chlorambucil, for the treatment of previously untreated patients with chronic lymphocytic leukemia (CLL) for whom fludarabine-based therapy is considered inappropriate [seeClinical Studies (14.1)].
- The recommended dosage and schedule is:
- 300 mg on Day 1 followed 1 week later by 1,000 mg on Day 8 (Cycle 1) followed by
- 1,000 mg on Day 1 of subsequent 28-day cycles for a minimum of 3 cycles until best response or a maximum of 12 cycles.
Refractory CLL
- ARZERRA is indicated for the treatment of patients with CLL refractory to fludarabine and alemtuzumab.
- The recommended dosage and schedule is 12 doses administered as follows:
- 300 mg initial dose (Dose 1), followed 1 week later by
- 2,000 mg weekly for 7 doses (Doses 2 through 8), followed 4 weeks later by
- 2,000 mg every 4 weeks for 4 doses (Doses 9 through 12).
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Ofatumumab in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Ofatumumab in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Ofatumumab in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Ofatumumab in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Ofatumumab in pediatric patients.
Contraindications
- None.
Warnings
|
WARNING
See full prescribing information for complete Boxed Warning.
HEPATITIS B VIRUS (HBV) REACTIVATION AND PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY
|
Precautions
- Infusion Reactions
- ARZERRA can cause serious, including fatal, infusion reactions manifesting as bronchospasm, dyspnea, laryngeal edema, pulmonary edema, flushing, hypertension, hypotension, syncope, cardiac events (e.g., myocardial ischemia/infarction, acute coronary syndrome, arrhythmia, bradycardia), back pain, abdominal pain, pyrexia, rash, urticaria, angioedema, cytokine release syndrome, and anaphylactoid/anaphylactic reactions. Infusion reactions occur more frequently with the first 2 infusions. These reactions may result in temporary interruption or withdrawal of treatment.
- Premedicate with acetaminophen, an antihistamine, and a corticosteroid. Infusion reactions may occur despite premedication. Interrupt infusion with ARZERRA for infusion reactions of any severity. Institute medical management for severe infusion reactions including angina or other signs and symptoms of myocardial ischemia. If an anaphylactic reaction occurs, immediately and permanently discontinue ARZERRA and initiate appropriate medical treatment.
- Hepatitis B Virus Reactivation
- Hepatitis B virus (HBV) reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, has occurred in patients treated with ARZERRA. Cases have been reported in patients who are hepatitis B surface antigen (HBsAg) positive and also in patients who are HBsAg negative but are hepatitis B core antibody (anti-HBc) positive. Reactivation also has occurred in patients who appear to have resolved hepatitis B infection (i.e., HBsAg negative, anti-HBc positive, and hepatitis B surface antibody [anti-HBs] positive).
- HBV reactivation is defined as an abrupt increase in HBV replication manifesting as a rapid increase in serum HBV DNA level or detection of HBsAg in a person who was previously HBsAg negative and anti-HBc positive. Reactivation of HBV replication is often followed by hepatitis, i.e., increase in transaminase levels and, in severe cases, increase in bilirubin levels, liver failure, and death.
- Screen all patients for HBV infection by measuring HBsAg and anti-HBc before initiating treatment with ARZERRA. For patients who show evidence of hepatitis B infection (HBsAg positive [regardless of antibody status] or HBsAg negative but anti-HBc positive), consult physicians with expertise in managing hepatitis B regarding monitoring and consideration for HBV antiviral therapy.
- Monitor patients with evidence of current or prior HBV infection for clinical and laboratory signs of hepatitis or HBV reactivation during and for several months following treatment with ARZERRA. HBV reactivation has been reported for at least 12 months following completion of therapy.
- In patients who develop reactivation of HBV while receiving ARZERRA, immediately discontinue ARZERRA and any concomitant chemotherapy, and institute appropriate treatment. Resumption of ARZERRA in patients whose HBV reactivation resolves should be discussed with physicians with expertise in managing hepatitis B. Insufficient data exist regarding the safety of resuming ARZERRA in patients who develop HBV reactivation.
- Hepatitis B Virus Infection
- Fatal infection due to hepatitis B in patients who have not been previously infected has been observed with ARZERRA. Monitor patients for clinical and laboratory signs of hepatitis.
- Progressive Multifocal Leukoencephalopathy
- Progressive multifocal leukoencephalopathy (PML) resulting in death has occurred with ARZERRA. Consider PML in any patient with new onset of or changes in pre-existing neurological signs or symptoms. If PML is suspected, discontinue ARZERRA and initiate evaluation for PML including neurology consultation.
- Tumor Lysis Syndrome
- Tumor lysis syndrome (TLS), including the need for hospitalization, has occurred in patients treated with ARZERRA. Patients with high tumor burden and/or high circulating lymphocyte counts (>25 x 109/L) are at greater risk for developing TLS. Consider tumor lysis prophylaxis with anti-hyperuricemics and hydration beginning 12 to 24 hours prior to infusion of ARZERRA. For treatment of TLS, administer aggressive intravenous hydration and anti-hyperuricemic agents, correct electrolyte abnormalities, and monitor renal function.
- Cytopenias
- Severe cytopenias, including neutropenia, thrombocytopenia, and anemia, can occur with ARZERRA. Pancytopenia, agranulocytosis, and fatal neutropenic sepsis have occurred in patients who received ARZERRA in combination with chlorambucil. Grade 3 or 4 late-onset neutropenia (onset at least 42 days after last treatment dose) and/or prolonged neutropenia (not resolved between 24 and 42 days after last treatment dose) were reported in patients who received ARZERRA. Monitor complete blood counts at regular intervals during and after conclusion of therapy, and increase the frequency of monitoring in patients who develop Grade 3 or 4 cytopenias.
- Immunizations
- The safety of immunization with live viral vaccines during or following administration of ARZERRA has not been studied. Do not administer live viral vaccines to patients who have recently received ARZERRA. The ability to generate an immune response to any vaccine following administration of ARZERRA has not been studied.
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
- Previously Untreated CLL: The safety of ARZERRA was evaluated in an open-label, parallel-arm, randomized trial (Study 1) in 444 patients with previously untreated CLL. Patients were randomized to receive either ARZERRA as an intravenous infusion every 28 days in combination with chlorambucil (n = 217) or chlorambucil as a single agent (n = 227). In both arms, patients received chlorambucil 10 mg/m2 orally on Days 1 to 7 every 28 days. The infusion schedule for ARZERRA was 300 mg administered on Cycle 1 Day 1, 1,000 mg administered on Cycle 1 Day 8, and 1,000 mg administered on Day 1 of subsequent 28-day cycles. The median number of cycles of ARZERRA completed was 6.
- The data described in Table 3 include relevant adverse reactions occurring up to 60 days after the last dose of study medication; Table 4 includes relevant hematologic laboratory abnormalities.

This image is provided by the National Library of Medicine.


This image is provided by the National Library of Medicine.

- Infusion Reactions: Overall, 67% of patients who received ARZERRA in combination with chlorambucil experienced one or more symptoms of infusion reactions (10% were Grade 3 or greater; none were fatal). Infusion reactions that were either Grade 3 or greater, serious, or led to treatment interruption or discontinuation occurred most frequently during Cycle 1 (56% on Day 1 [6% were Grade 3 or greater] and 23% on Day 8 [3% were Grade 3 or greater]) and decreased with subsequent infusions. Infusion reactions led to discontinuation of treatment in 3% of patients. Serious adverse events of infusion reactions occurred in 2% of patients.
- Neutropenia: Overall, 3% of patients had neutropenia as a serious adverse event, reported up to 60 days after the last dose. One patient died with neutropenic sepsis and agranulocytosis. Prolonged neutropenia occurred in 6% of patients receiving ARZERRA in combination with chlorambucil compared with 4% of patients receiving chlorambucil. Late-onset neutropenia occurred in 6% of patients receiving ARZERRA in combination with chlorambucil compared with 1% of patients receiving chlorambucil alone.
- Refractory CLL: The safety of monotherapy with ARZERRA was evaluated in 181 patients with relapsed or refractory CLL in 2 open‑label, non‑randomized, single‑arm studies. In these studies, ARZERRA was administered at 2,000 mg beginning with the second dose for 11 doses (Study 2 [n = 154]) or 3 doses (Study 3 [n = 27]).
- The data described in Table 5 and other sections below are derived from 154 patients in Study 2. All patients received 2,000 mg weekly from the second dose onward. Ninety percent of patients received at least 8 infusions of ARZERRA and 55% received all 12 infusions. The median age was 63 years (range: 41 to 86 years), 72% were male, and 97% were white.
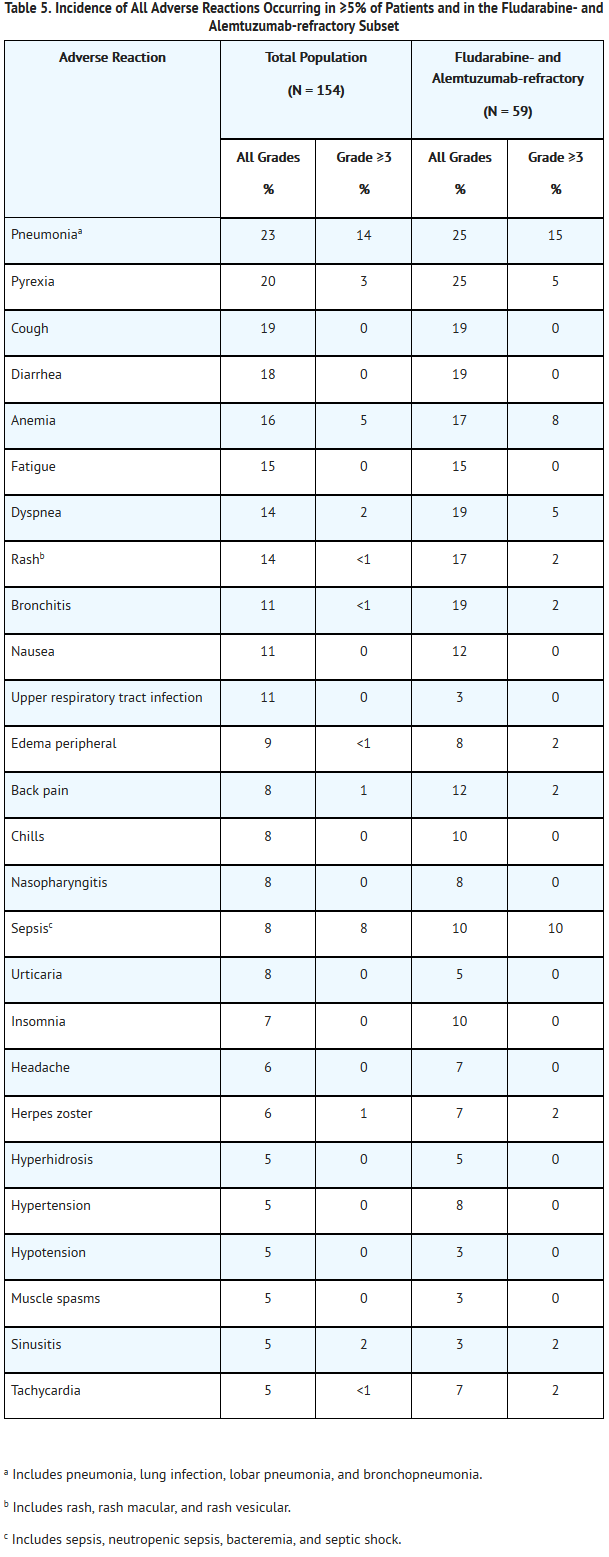
This image is provided by the National Library of Medicine.

- Infusion Reactions: Infusion reactions occurred in 44% of patients on the day of the first infusion (300 mg), 29% on the day of the second infusion (2,000 mg), and less frequently during subsequent infusions.
- Infections: A total of 108 patients (70%) experienced bacterial, viral, or fungal infections. A total of 45 patients (29%) experienced Grade 3 or greater infections, of which 19 (12%) were fatal. The proportion of fatal infections in the fludarabine‑ and alemtuzumab‑refractory group was 17%.
- Neutropenia: Of 108 patients with normal neutrophil counts at baseline, 45 (42%) developed Grade 3 or greater neutropenia. Nineteen (18%) developed Grade 4 neutropenia. Some patients experienced new onset Grade 4 neutropenia >2 weeks in duration.
- Immunogenicity
- There is a potential for immunogenicity with therapeutic proteins such as ofatumumab. Serum samples from more than 300 patients with CLL were tested during and after treatment for antibodies to ARZERRA. There was no formation of anti‑ofatumumab antibodies in patients with CLL after treatment with ofatumumab.
- Immunogenicity assay results are highly dependent on several factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of incidence of antibodies to ARZERRA with the incidence of antibodies to other products may be misleading.
Postmarketing Experience
- The following adverse reactions have been identified during post-approval use of ARZERRA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Infusion-related Cardiac Events: Cardiac arrest.
- Mucocutaneous Reactions: Stevens-Johnson syndrome, porphyria cutanea tarda.
Drug Interactions
- Coadministration of ARZERRA with chlorambucil did not result in clinically relevant effects on the pharmacokinetics of chlorambucil or its active metabolite, phenylacetic acid mustard.
Use in Specific Populations
Pregnancy
- Pregnancy Category C
- There are no adequate or well‑controlled studies of ofatumumab in pregnant women. A reproductive study in pregnant cynomolgus monkeys that received ofatumumab at doses up to 3.5 times the maximum recommended human dose (2,000 mg) of ofatumumab did not demonstrate maternal toxicity or teratogenicity. Ofatumumab crossed the placental barrier, and fetuses exhibited depletion of peripheral B cells and decreased spleen and placental weights. ARZERRA should be used during pregnancy only if the potential benefit to the mother justifies the potential risk to the fetus.
- There are no human or animal data on the potential short- and long-term effects of perinatal B-cell depletion in offspring following in utero exposure to ofatumumab. Ofatumumab does not bind normal human tissues other than B lymphocytes. It is not known if binding occurs to unique embryonic or fetal tissue targets. In addition, the kinetics of B-lymphocyte recovery are unknown in offspring with B-cell depletion.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Ofatumumab in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Ofatumumab during labor and delivery.
Nursing Mothers
- It is not known whether ofatumumab is secreted in human milk; however, human IgG is secreted in human milk. Published data suggest that neonatal and infant consumption of breast milk does not result in substantial absorption of these maternal antibodies into circulation. Because the effects of local gastrointestinal and limited systemic exposure to ofatumumab are unknown, caution should be exercised when ARZERRA is administered to a nursing woman.
Pediatric Use
- Safety and effectiveness of ARZERRA have not been established in children.
Geriatic Use
- In Study 1, 68% of patients (148/217) receiving ARZERRA plus chlorambucil were 65 years and older. Patients age 65 years and older experienced a higher incidence of the following Grade 3 or greater adverse reactions compared with patients younger than 65 years of age: neutropenia (30% versus 17%) and pneumonia (5% versus 1%). In patients 65 years and older, 29% experienced serious adverse events compared with 13% of patients younger than 65 years. No clinically meaningful differences in the effectiveness of ARZERRA plus chlorambucil were observed between older and younger patients.
- In refractory CLL, clinical studies of ARZERRA did not include sufficient numbers of subjects aged 65 years and older to determine whether they respond differently from younger subjects.
Gender
There is no FDA guidance on the use of Ofatumumab with respect to specific gender populations.
Race
There is no FDA guidance on the use of Ofatumumab with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Ofatumumab in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Ofatumumab in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Ofatumumab in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Ofatumumab in patients who are immunocompromised.
Administration and Monitoring
Administration
- Intravenous
Monitoring
There is limited information regarding Monitoring of Ofatumumab in the drug label.
IV Compatibility
- Do not shake product.
- Inspect parenteral drug products visually for particulate matter and discoloration prior to administration. ARZERRA should be a clear to opalescent, colorless solution. The solution should not be used if discolored or cloudy, or if foreign particulate matter is present.
- Preparation of Solution:
- 300-mg dose: Withdraw and discard 15 mL from a 1,000-mL bag of 0.9% Sodium Chloride Injection, USP. Withdraw 5 mL from each of 3 single-use 100-mg vials of ARZERRA and add to the bag. Mix diluted solution by gentle inversion.
- 1,000-mg dose: Withdraw and discard 50 mL from a 1,000-mL bag of 0.9% Sodium Chloride Injection, USP. Withdraw 50 mL from 1 single-use 1,000-mg vial of ARZERRA and add to the bag. Mix diluted solution by gentle inversion.
- 2,000-mg dose: Withdraw and discard 100 mL from a 1,000-mL bag of 0.9% Sodium Chloride Injection, USP. Withdraw 50 mL from each of 2 single-use 1,000-mg vials of ARZERRA and add to the bag. Mix diluted solution by gentle inversion.
- Store diluted solution between 2° to 8°C (36° to 46°F).
- No incompatibilities between ARZERRA and polyvinylchloride or polyolefin bags and administration sets have been observed.
- Administration Instructions:
- Do not mix ARZERRA with, or administer as an infusion with, other medicinal products.
- Administer using an infusion pump and an administration set.
- Flush the intravenous line with 0.9% Sodium Chloride Injection, USP before and after each dose.
- Start infusion within 12 hours of preparation.
- Discard prepared solution after 24 hours.
Overdosage
Chronic Overdose
There is limited information regarding Chronic Overdose of Ofatumumab in the drug label.
Pharmacology
Ofatumumab?
| |
| Therapeutic monoclonal antibody | |
| Source | u |
| Target | CD20 |
| Identifiers | |
| CAS number | |
| ATC code | L01 |
| PubChem | ? |
| Chemical data | |
| Formula | Template:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox |
| Mol. mass | 146.1 kDa |
| Pharmacokinetic data | |
| Bioavailability | ? |
| Metabolism | ? |
| Half life | 14 days |
| Excretion | ? |
| Therapeutic considerations | |
| Licence data |
, |
| Pregnancy cat. |
C(US) |
| Legal status |
POM(UK) [[Prescription drug|Template:Unicode-only]](US) |
| Routes | IV |
Mechanism of Action
- Ofatumumab binds specifically to both the small and large extracellular loops of the CD20 molecule. The CD20 molecule is expressed on normal B lymphocytes (pre–B- to mature B-lymphocyte) and on B-cell CLL. The CD20 molecule is not shed from the cell surface and is not internalized following antibody binding.
- The Fab domain of ofatumumab binds to the CD20 molecule and the Fc domain mediates immune effector functions to result in B-cell lysis in vitro. Data suggest that possible mechanisms of cell lysis include complement-dependent cytotoxicity and antibody-dependent, cell-mediated cytotoxicity.
Structure
- ARZERRA (ofatumumab) is an IgG1κ human monoclonal antibody with a molecular weight of approximately 149 kDa. The antibody was generated via transgenic mouse and hybridoma technology and is produced in a recombinant murine cell line (NS0) using standard mammalian cell cultivation and purification technologies.
- ARZERRA is a sterile, clear to opalescent, colorless, preservative-free liquid concentrate for intravenous administration. ARZERRA is supplied at a concentration of 20 mg/mL in single-use vials. Each single-use vial contains either 100 mg ofatumumab in 5 mL of solution or 1,000 mg ofatumumab in 50 mL of solution.
- Inactive ingredients include: 10 mg/mL arginine, diluted hydrochloric acid, 0.019 mg/mL edetate disodium, 0.2 mg/mL polysorbate 80, 6.8 mg/mL sodium acetate, 2.98 mg/mL sodium chloride, and Water for Injection, USP. The pH is 5.5.
Pharmacodynamics
- B-Cell Depletion: In patients with previously untreated CLL, at 6 months after the last dose, the median reductions in CD19‑positive B cells were >99% (n = 155) for ARZERRA in combination with chlorambucil and 94% (n = 121) for chlorambucil alone.
- In patients with CLL refractory to fludarabine and alemtuzumab, the median decrease in circulating CD19‑positive B cells was 91% (n = 50) with the 8th infusion and 85% (n = 32) with the 12th infusion. The time to recovery of lymphocytes, including CD19‑positive B cells, to normal levels has not been determined.
- Although the depletion of B-cells in the peripheral blood is a measurable pharmacodynamic effect, it is not directly correlated with the depletion of B cells in solid organs or in malignant deposits. B-cell depletion has not been shown to be directly correlated to clinical response.
- Cardiac Electrophysiology: The effect of multiple doses of ARZERRA on the QTc interval was evaluated in a pooled analysis of 3 open-label studies in patients with CLL (N = 85). Patients received ARZERRA 300 mg on Day 1 followed by either 1,000 mg or 2,000 mg for subsequent doses. No large changes in the mean QTc interval (i.e., >20 milliseconds) were detected in the pooled analysis.
Pharmacokinetics
- Ofatumumab is eliminated through both a target‑independent route and a B cell‑mediated route. Ofatumumab exhibited dose‑dependent clearance in the dose range of 100 to 2,000 mg. Due to the depletion of B cells, the clearance of ofatumumab decreased substantially after subsequent infusions compared with the first infusion.
- Pharmacokinetic data were obtained after repeated administration (4, 5, 8, or 12 infusions) of 1,000 mg or 2,000 mg doses in 381 patients with CLL (Studies 1, 2, and 3). The geometric mean (%CV) values for clearance, volume of distribution at steady state (Vss), and half-life for ofatumumab in these patients were 12.9 mL/hour (76%), 5.7 L (65%), and 15.6 days (90%). The pharmacokinetic profile was similar across doses in patients with CLL.
- Specific Populations:Effects of Body Size, Gender, Age, and Renal Impairment: Based on population pharmacokinetic analyses, body size, gender, age, and renal impairment (evaluated in patients with a calculated creatinine clearance ≥30 mL/min) do not have a clinically meaningful effect on the pharmacokinetics of ofatumumab.
Nonclinical Toxicology
- Carcinogenesis, Mutagenesis, Impairment of Fertility
- No carcinogenicity or mutagenicity studies of ofatumumab have been conducted. In a repeat‑dose toxicity study, no tumorigenic or unexpected mitogenic responses were noted in cynomolgus monkeys treated for 7 months with up to 3.5 times the maximum human dose (2,000 mg) of ofatumumab. Effects on male and female fertility have not been evaluated in animal studies.
- Reproductive and Developmental Toxicology
- Pregnant cynomolgus monkeys dosed with 0.7 or 3.5 times the maximum human dose (2,000 mg) of ofatumumab weekly during the period of organogenesis (gestation days 20 to 50) had no maternal toxicity or teratogenicity. Both dose levels of ofatumumab depleted circulating B cells in the dams, with signs of initial B cell recovery 50 days after the final dose. Following Caesarean section at gestational day 100, fetuses from ofatumumab‑treated dams exhibited decreases in mean peripheral B‑cell counts (decreased to approximately 10% of control values), splenic B‑cell counts (decreased to approximately 15% to 20% of control values), and spleen weights (decreased by 15% for the low‑dose and by 30% for the high‑dose group, compared with control values). Fetuses from treated dams exhibiting anti‑ofatumumab antibody responses had higher B cell counts and higher spleen weights compared with the fetuses from other treated dams, indicating partial recovery in those animals developing anti‑ofatumumab antibodies. When compared with control animals, fetuses from treated dams in both dose groups had a 10% decrease in mean placental weights. A 15% decrease in mean thymus weight compared with the controls was also observed in fetuses from dams treated with 3.5 times the human dose of ofatumumab. The biological significance of decreased placental and thymic weights is unknown.
- The kinetics of B‑lymphocyte recovery and the potential long-term effects of perinatal B‑cell depletion in offspring from ofatumumab‑treated dams have not been studied in animals.
Clinical Studies
Previously Untreated CLL
- The efficacy of ARZERRA was evaluated in a randomized, open-label, parallel-arm study; 447 patients previously untreated for CLL were randomized to receive either ARZERRA as monthly intravenous infusions (Cycle 1: 300 mg on Day 1 and 1,000 mg on Day 8; subsequent cycles: 1,000 mg on Day 1 every 28 days) in combination with chlorambucil (10 mg/m2 orally on Days 1 to 7 every 28 days) or chlorambucil alone (10 mg/m2 orally on Days 1 to 7 every 28 days). Patients received treatment for a minimum of 3 cycles. Treatment was continued for 3 cycles beyond maximal response (2 consecutive response assessments of stable disease, partial response, or complete response) for up to 12 cycles. Approximately 60% of patients received 3 to 6 cycles of ARZERRA and 30% received 7 to 12 cycles.
- This trial enrolled patients for whom fludarabine-based therapy was considered to be inappropriate by the investigator for reasons that included advanced age or presence of co-morbidities. In the overall trial population, the median age was 69 years (range: 35 to 92 years) and 69% of patients in both arms were at least 65 years of age. In the overall trial population, 72% of patients had 2 or more co-morbidities and 48% of patients had a creatinine clearance of less than 70 mL/min. Sixty-three percent of patients were male and 89% were white. Elevated beta-2 microglobulin (β2m) >3,500 mcg/L was present in 72% of patients at baseline.
- The primary endpoint was progression-free-survival (PFS) as assessed by a blinded Independent Review Committee (IRC) using the International Workshop for Chronic Lymphocytic Leukemia (IWCLL) updated National Cancer Institute-sponsored Working Group (NCI-WG) guidelines (2008). ARZERRA plus chlorambucil resulted in statistically significant improvement in IRC-assessed median PFS compared with chlorambucil alone (22.4 months versus 13.1 months; hazard ratio: 0.57 [0.45, 0.72]) (Table 6; Figure 1).
- Secondary efficacy endpoints, including overall response (OR), complete response (CR), and duration of response, were also assessed by the IRC using the 2008 IWCLL Guidelines (Table 6).

This image is provided by the National Library of Medicine.

=Refractory CLL
- Study 2 was a single‑arm, multicenter study in 154 patients with relapsed or refractory CLL. ARZERRA was administered by intravenous infusion according to the following schedule: 300 mg (Week 0), 2,000 mg weekly for 7 infusions (Weeks 1 through 7), and 2,000 mg every 4 weeks for 4 infusions (Weeks 12 through 24). Patients with CLL refractory to fludarabine and alemtuzumab (n = 59) comprised the efficacy population. Drug refractoriness was defined as failure to achieve at least a partial response to, or disease progression within 6 months of, the last dose of fludarabine or alemtuzumab. The main efficacy outcome was durable objective tumor response rate. Objective tumor responses were determined using the 1996 NCI-WG Guidelines for CLL.
- In patients with CLL refractory to fludarabine and alemtuzumab, the median age was 64 years (range: 41 to 86 years), 75% were male, and 95% were white. The median number of prior therapies was 5; 93% received prior alkylating agents, 59% received prior rituximab, and all received prior fludarabine and alemtuzumab. Eighty-eight percent of patients received at least 8 infusions of ARZERRA and 54% received 12 infusions.
- The investigator‑determined overall response rate in patients with CLL refractory to fludarabine and alemtuzumab was 42% (99% CI: 26, 60) with a median duration of response of 6.5 months (95% CI: 5.8, 8.3). There were no complete responses. Anti‑tumor activity was also observed in additional patients in Study 2 and in a multicenter, open‑label, dose-escalation study (Study 3) conducted in patients with relapsed or refractory CLL.
How Supplied
- ARZERRA (ofatumumab) is a sterile, clear to opalescent, colorless, preservative-free liquid concentrate (20 mg/mL) for dilution and intravenous administration provided in single-use glass vials with a rubber stopper (not made with natural rubber latex) and an aluminum overseal. Each vial contains either 100 mg ofatumumab in 5 mL of solution or 1,000 mg ofatumumab in 50 mL of solution.
- ARZERRA is available as follows:

This image is provided by the National Library of Medicine.

- Store ARZERRA refrigerated between 2° to 8°C (36° to 46°F). Do not freeze. Vials should be protected from light.
Storage
There is limited information regarding Ofatumumab Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Ofatumumab |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Ofatumumab |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
- Advise patients to contact a healthcare professional for any of the following:
- Signs and symptoms of infusion reactions including fever, chills, rash, or breathing problems within 24 hours of infusion.
- Symptoms of hepatitis including worsening fatigue or yellow discoloration of skin or eyes.
- New neurological symptoms such as confusion, dizziness or loss of balance, difficulty talking or walking, or vision problems.
- Bleeding, easy bruising, petechiae, pallor, worsening weakness, or fatigue.
- Signs of infections including fever and cough.
- Pregnancy or nursing.
- Advise patients of the need for:
- Monitoring and possible need for treatment if they have a history of hepatitis B infection (based on the blood test).
- Periodic monitoring for blood counts.
- Avoiding vaccination with live viral vaccines.
Precautions with Alcohol
- Alcohol-Ofatumumab interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- ARZERRA®[1]
Look-Alike Drug Names
There is limited information regarding Ofatumumab Look-Alike Drug Names in the drug label.
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
{{#subobject:
|Page Name=Ofatumumab
|Pill Name=No image.jpg
|Drug Name=
|Pill Ingred=|+sep=;
|Pill Imprint=
|Pill Dosage={{{dosageValue}}} {{{dosageUnit}}}
|Pill Color=|+sep=;
|Pill Shape=
|Pill Size (mm)=
|Pill Scoring=
|Pill Image=
|Drug Author=
|NDC=
}}
{{#subobject:
|Label Page=Ofatumumab |Label Name=Ofatumumab08.png
}}
{{#subobject:
|Label Page=Ofatumumab |Label Name=Ofatumumab09.png
}}