Mitral valve prolapse classification
|
Mitral valve prolapse Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Mitral valve prolapse classification On the Web |
|
American Roentgen Ray Society Images of Mitral valve prolapse classification |
|
Risk calculators and risk factors for Mitral valve prolapse classification |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Classification
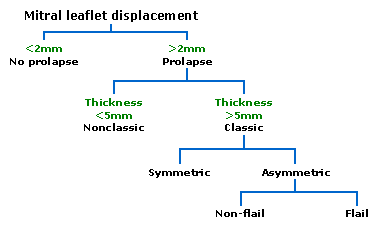
Prolapsed mitral valves are classified into several subtypes, based on leaflet thickness, concavity, and type of connection to the mitral annulus. Subtypes can be described as classic, nonclassic, symmetric, asymmetric, flail, or non-flail.
Note: all measurements below refer to adult patients and applying them to children may be misleading.
-
Diagnosis of mitral valve prolapse is based on modern echocardiographic techniques which can pinpoint abnormal leaflet thickening and other related pathology.

Classic versus nonclassic
Prolapse occurs when the mitral valve leaflets are displaced more than 2 mm above the mitral annulus high points. The condition can be further divided into classic and nonclassic subtypes based on the thickness of the mitral valve leaflets: up to 5 mm is considered nonclassic, while anything beyond 5 mm is considered classic MVP.
Symmetric versus asymmetric
Classic MVP may be subdivided into symmetric and asymmetric, referring to the point at which leaflet tips join the mitral annulus. In symmetric coaptation, leaflet tips meet at a common point on the annulus. Asymmetric coaptation is characterized by one leaflet being displaced toward the atrium with respect to the other. Patients with asymmetric prolapse are susceptible to severe deterioration of the mitral valve, with the possible rupture of the chordae tendineae and the development of a flail leaflet.
Flail versus non-flail
Asymmetric prolapse is further subdivided into flail and non-flail prolapse. Flail prolapse occurs when a leaflet tip turns outward, becoming concave toward the left atrium, causing the deterioration of the mitral valve. The severity of flail leaflet varies, ranging from tip eversion to chordal rupture. Dissociation of leaflet and chordae tendineae provides for unrestricted motion of the leaflet (hence "flail leaflet"). Thus patients with flail leaflets have a higher prevalence of mitral regurgitation than those with the non-flail subtype.