Leiomyoma: Difference between revisions
No edit summary |
No edit summary |
||
| Line 9: | Line 9: | ||
Uterine leiomyoma was first discovered by Hippocrates, a greek physician also called as father of modern medicine in 460-375 B.C and called it “uterine stone”. Uterine leiomyoma may be classified according to their location into 3 subtypes: submucosal, subserous, and intramural. The pathogenesis of leiomyoma is characterized by [[benign]] [[smooth muscle]] [[neoplasm]]. They can occur in any organ, but the most common forms occur in the [[uterus]], [[small bowel]] and the [[esophagus]]. Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q has been associated with the development of leiomyoma. Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as:uterine adenomyoma, pregnancy, hematometra, uterine sarcoma, uterine carcinosarcoma, and metastasis. Leiomyoma is more commonly observed among patients aged 40 years and older. Common risk factors in the development of uterine leiomyoma are Afro-American race, early menarche, prenatal exposure to diethylstilbestrol, having one or more pregnancies extending beyond 20 weeks, obesity, significant consumption of beef and other reds meats, hypertension, family history, and alcohol consumption. Physical examination may be remarkable for enlarged, mobile uterus with an irregular contour on bimanual pelvic examination. The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, [[Gonadotropin-releasing hormone analog]]s. Surgery is the mainstay of therapy for uterine leiomyoma. | Uterine leiomyoma was first discovered by Hippocrates, a greek physician also called as father of modern medicine in 460-375 B.C and called it “uterine stone”. Uterine leiomyoma may be classified according to their location into 3 subtypes: submucosal, subserous, and intramural. The pathogenesis of leiomyoma is characterized by [[benign]] [[smooth muscle]] [[neoplasm]]. They can occur in any organ, but the most common forms occur in the [[uterus]], [[small bowel]] and the [[esophagus]]. Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q has been associated with the development of leiomyoma. Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as:uterine adenomyoma, pregnancy, hematometra, uterine sarcoma, uterine carcinosarcoma, and metastasis. Leiomyoma is more commonly observed among patients aged 40 years and older. Common risk factors in the development of uterine leiomyoma are Afro-American race, early menarche, prenatal exposure to diethylstilbestrol, having one or more pregnancies extending beyond 20 weeks, obesity, significant consumption of beef and other reds meats, hypertension, family history, and alcohol consumption. Physical examination may be remarkable for enlarged, mobile uterus with an irregular contour on bimanual pelvic examination. The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, [[Gonadotropin-releasing hormone analog]]s. Surgery is the mainstay of therapy for uterine leiomyoma. | ||
==Historical Perspective== | ==Historical Perspective== | ||
*Uterine leiomyoma was first discovered by Hippocrates | *Uterine leiomyoma was first discovered by Hippocrates in 460-375 B.C and called it “uterine stone”. | ||
*In the second | *In the second century AD, Galen described the lesion as "scleromas".<ref name="BoziniBaracat2007">{{cite journal|last1=Bozini|first1=Nilo|last2=Baracat|first2=Edmund C|title=The history of myomectomy at the Medical School of University of São Paulo|journal=Clinics|volume=62|issue=3|year=2007|issn=1807-5932|doi=10.1590/S1807-59322007000300002}}</ref> | ||
*In 1860 and 1863, Rokitansky and Klob coined the term | *In 1860 and 1863, Rokitansky and Klob coined the term fibroid. | ||
*In 1854, Virchow a German pathologist demonstrated that those tumors originated from the uterine smooth muscle. Thus, the term "myoma" became current in clinical use. | *In 1854, Virchow, a German pathologist demonstrated that those tumors originated from the uterine smooth muscle. Thus, the term "myoma" became current in clinical use. | ||
*In 1809, the first laparotomy consequent to myoma indication was conducted by Ephraim McDowell to treat | *In 1809, the first laparotomy consequent to myoma indication was conducted by Ephraim McDowell to treat leiomyoma in Danville, USA. | ||
*The first successful myomectomy was performed by Amussat in 1840, after a clinical diagnosis of ovarian tumor because pelvic examination showed a pediculate and large uterine leiomyoma. | *The first successful myomectomy was performed by Amussat in 1840, after a clinical diagnosis of ovarian tumor because pelvic examination showed a pediculate and large uterine leiomyoma. | ||
*The first scientific report of a uterus conserving myomectomy through the vagina appeared in 1845 in the American Journal of | *The first scientific report of a uterus conserving myomectomy through the vagina appeared in 1845 in the American Journal of Medical Science, accomplished by Washington Atlee, in Pennsylvania. | ||
*In 1898, Alexander Adam presented 11 cases of myomectomy through an abdominal route, in Liverpool. | *In 1898, Alexander Adam presented 11 cases of myomectomy through an abdominal route, in Liverpool. | ||
*In 1940, Carlos R. Círio proposed a technique of the myometrium emptying, called myometrectomy. | *In 1940, Carlos R. Círio proposed a technique of the myometrium emptying, called myometrectomy. | ||
==Classification== | ==Classification== | ||
*Uterine leiomyoma may be classified according to | *Uterine leiomyoma may be classified into 3 subtypes according to location: | ||
:* | :*[[Submucosal]] – lie just beneath the [[endometrium]]. | ||
:*[[wiktionary:Intramural|Intramural]] – lie within the uterine wall. | :*[[wiktionary:Intramural|Intramural]] – lie within the uterine wall. | ||
:* | :*Subserous – lies at the [[Serous|serosal]] surface of the uterus or may bulge out from the [[myometrium]] and can become [[pedunculated]]. | ||
==Pathophysiology== | ==Pathophysiology== | ||
*The pathogenesis of leiomyoma is characterized by [[benign]] [[smooth muscle]] [[neoplasm]]. They can occur in any organ, but the most common forms occur in the [[uterus]], [[small bowel]] and the [[esophagus]]. | *The pathogenesis of leiomyoma is characterized by [[benign]] [[smooth muscle]] [[neoplasm]]. They can occur in any organ, but the most common forms occur in the [[uterus]], [[small bowel]] and the [[esophagus]]. | ||
*The chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q | *The chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma.<ref>Genetics of Uterine Leiomyomas. glowm (2016). http://www.glowm.com/section_view/heading/Genetics%20of%20Uterine%20Leiomyomas/item/363 Accessed on April 19, 2016</ref> | ||
*On gross pathology, round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and whorled are characteristic findings of leiomyoma . | *On gross pathology, round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and whorled are characteristic findings of leiomyoma . | ||
*On microscopic histopathological analysis, elongated, spindle-shaped cells with a cigar-shaped nucleus are characteristic findings of leiomyoma. | *On microscopic histopathological analysis, elongated, spindle-shaped cells with a cigar-shaped nucleus are characteristic findings of leiomyoma. | ||
===Uterine Leiomyomata=== | ===Uterine Leiomyomata=== | ||
Uterine fibroids are leiomyomata of the [[uterus|uterine]] smooth muscle. As other leiomyomata, they are [[benign]], but may lead to excessive menstrual bleeding ([[menorrhagia]]), often cause [[anemia]] and may lead to [[infertility]]. Enucleation is removal of fibroids without removing the uterus ([[hysterectomy]]), which is also commonly performed. [[Laser]] surgery (called myolysis) is increasingly used, and provides a viable alternative to surgery. Estrogen and progesterone usually stimulate their growth, and hormone suppression may hence decrease their size. | Uterine fibroids are leiomyomata of the [[uterus|uterine]] smooth muscle. As with other leiomyomata, they are [[benign]], but may lead to excessive menstrual bleeding ([[menorrhagia]]), often cause [[anemia]] and may lead to [[infertility]]. Enucleation is removal of fibroids without removing the uterus ([[hysterectomy]]), which is also commonly performed. [[Laser]] surgery (called myolysis) is increasingly used, and provides a viable alternative to surgery. Estrogen and progesterone usually stimulate their growth, and hormone suppression may hence decrease their size. | ||
===Esophageal=== | ===Esophageal=== | ||
Leiomyoma of the esophagus is the most common [[benign]] [[esophagus|esophageal]] [[tumour]], though this accounts for less than 1% of esophageal neoplasms. The remainder consists mainly of carcinomas. Although the vast majority of benign esophageal tumors are clinically silent and go undetected, large or strategically located tumors may become symptomatic. <ref name="AMN">{{cite web | author = James C. Chou, MD & Frank G. Gress, MD | title =Benign Esophageal Tumors | work =Esophageal Cancer Overview (Cancer of the Esophagus) | url=http://www.health.am/cr/benign-esophageal-tumors/ | publsiher=Armenian Health Network, Health.am | accessdate=2007-03-21}}</ref> | |||
===Leiomyoma of Jejunum=== | ===Leiomyoma of Jejunum=== | ||
Leiomyoma is the most common benign tumor of small bowel. Approximately 50% of cases are found in the jejunum, followed by the ileum in 31% of cases. Almost one half of all lesions are less than 5 centimeters. <ref name=ARO>{{cite web | author = By Michael P. Buetow, M.D. | title =Leiomyoma of Jejunum | url=http://www.appliedradiology.com/case/case.asp?ID=88&SubCatID=97&CatID=43&ThreadID= | publsiher=Applied Radiology Online | accessdate=2007-03-21}}</ref> | Leiomyoma is the most common benign tumor of small bowel. Approximately 50% of cases are found in the jejunum, followed by the ileum in 31% of cases. Almost one half of all lesions are less than 5 centimeters. <ref name="ARO">{{cite web | author = By Michael P. Buetow, M.D. | title =Leiomyoma of Jejunum | url=http://www.appliedradiology.com/case/case.asp?ID=88&SubCatID=97&CatID=43&ThreadID= | publsiher=Applied Radiology Online | accessdate=2007-03-21}}</ref> | ||
<gallery> | <gallery> | ||
Image:leiomyoma.jpg|Leiomyoma enucleated from a uterus. External surface on left; cut surface on right | Image:leiomyoma.jpg|Leiomyoma enucleated from a uterus. External surface on left; cut surface on right | ||
| Line 39: | Line 39: | ||
</gallery> | </gallery> | ||
==Causes== | ==Causes== | ||
* Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q | * Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma. | ||
==Differentiating Leiomyoma from other Diseases== | ==Differentiating Leiomyoma from other Diseases== | ||
*Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as: | *Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as: | ||
:*Uterine adenomyoma | :*Uterine [[adenomyoma]] | ||
:*Pregnancy | :*Pregnancy | ||
:*Hematometra | :*[[Hematometra]] | ||
:*Uterine sarcoma | :*[[Uterine sarcoma]] | ||
:*Uterine carcinosarcoma | :*Uterine carcinosarcoma | ||
:*Endometrial carcinoma | :*[[Endometrial carcinoma]] | ||
:*Metastasis | :*Metastasis | ||
==Epidemiology and Demographics== | ==Epidemiology and Demographics== | ||
| Line 53: | Line 53: | ||
*Leiomyoma is more commonly observed among patients aged 40 years and older. | *Leiomyoma is more commonly observed among patients aged 40 years and older. | ||
===Race=== | ===Race=== | ||
*Leiomyoma usually affects | *Leiomyoma usually affects African-American women. | ||
==Risk Factors== | ==Risk Factors== | ||
*Common risk factors in the development of uterine leiomyoma | *Common risk factors in the development of uterine leiomyoma include: | ||
**African-American race | |||
**Early [[menarche]] | |||
**Prenatal exposure to [[diethylstilbestrol]] | |||
**Having one or more pregnancies extending beyond 20 weeks | |||
**Obesity | |||
**Significant consumption of beef and other reds meats | |||
**[[Hypertension]] | |||
**Alcohol consumption | |||
== Natural History, Complications and Prognosis== | == Natural History, Complications and Prognosis== | ||
*The majority of patients with uterine leiomyoma remain asymptomatic for | *The majority of patients with uterine leiomyoma remain asymptomatic for decades | ||
*Common complications of uterine leiomyoma include | *Common complications of uterine leiomyoma include: | ||
**[[Dysmenorrhea]] | |||
**[[Dyspareunia]] | |||
**Leiomyoma degeneration or torsion | |||
**Transcervical prolapse | |||
**Miscarriage. | |||
== Diagnosis == | == Diagnosis == | ||
=== Symptoms === | === Symptoms === | ||
| Line 76: | Line 89: | ||
*On ultrasound imaging, uterine leiomyoma is characterized by the fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam. | *On ultrasound imaging, uterine leiomyoma is characterized by the fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam. | ||
=== Other Diagnostic Studies === | === Other Diagnostic Studies === | ||
*Uterine leiomyoma may also be diagnosed using diagnostic hysteroscopy, magnetic resonance imaging, and hysterosalpingography. | *Uterine leiomyoma may also be diagnosed using diagnostic [[hysteroscopy]], [[magnetic resonance imaging]], and [[hysterosalpingography]]. | ||
<gallery> | <gallery> | ||
Image: | Image: | ||
| Line 144: | Line 157: | ||
=== Surgery === | === Surgery === | ||
*Surgery is the mainstay of therapy for uterine leiomyoma. | *Surgery is the mainstay of therapy for uterine leiomyoma. | ||
*[[Uterine artery embolization]] in conjunction with [[laparotomy|laparotomic]] myomectomy is the most common approach to the treatment of | *[[Uterine artery embolization]] in conjunction with [[laparotomy|laparotomic]] myomectomy is the most common approach to the treatment of leiomyoma. | ||
*[[Hysteroscopy|Hysteroscopic]] myomectomy can also be performed for patients with uterine leiomyoma. | *[[Hysteroscopy|Hysteroscopic]] myomectomy can also be performed for patients with uterine leiomyoma. | ||
Revision as of 13:54, 26 April 2016
|
WikiDoc Resources for Leiomyoma |
|
Articles |
|---|
|
Most recent articles on Leiomyoma |
|
Media |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Leiomyoma at Clinical Trials.gov Clinical Trials on Leiomyoma at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Leiomyoma
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Leiomyoma Discussion groups on Leiomyoma Directions to Hospitals Treating Leiomyoma Risk calculators and risk factors for Leiomyoma
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Leiomyoma |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
For patient information, click here.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Shanshan Cen, M.D. [3]; Ammu Susheela, M.D. [4]
Synonyms and keywords: Uterine myoma; Fibroid; Fibroids, Uterine; Fibroid Tumor; Fibroid Uterus; Uterine fibromyoma
Overview
Uterine leiomyoma was first discovered by Hippocrates, a greek physician also called as father of modern medicine in 460-375 B.C and called it “uterine stone”. Uterine leiomyoma may be classified according to their location into 3 subtypes: submucosal, subserous, and intramural. The pathogenesis of leiomyoma is characterized by benign smooth muscle neoplasm. They can occur in any organ, but the most common forms occur in the uterus, small bowel and the esophagus. Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q has been associated with the development of leiomyoma. Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as:uterine adenomyoma, pregnancy, hematometra, uterine sarcoma, uterine carcinosarcoma, and metastasis. Leiomyoma is more commonly observed among patients aged 40 years and older. Common risk factors in the development of uterine leiomyoma are Afro-American race, early menarche, prenatal exposure to diethylstilbestrol, having one or more pregnancies extending beyond 20 weeks, obesity, significant consumption of beef and other reds meats, hypertension, family history, and alcohol consumption. Physical examination may be remarkable for enlarged, mobile uterus with an irregular contour on bimanual pelvic examination. The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, Gonadotropin-releasing hormone analogs. Surgery is the mainstay of therapy for uterine leiomyoma.
Historical Perspective
- Uterine leiomyoma was first discovered by Hippocrates in 460-375 B.C and called it “uterine stone”.
- In the second century AD, Galen described the lesion as "scleromas".[1]
- In 1860 and 1863, Rokitansky and Klob coined the term fibroid.
- In 1854, Virchow, a German pathologist demonstrated that those tumors originated from the uterine smooth muscle. Thus, the term "myoma" became current in clinical use.
- In 1809, the first laparotomy consequent to myoma indication was conducted by Ephraim McDowell to treat leiomyoma in Danville, USA.
- The first successful myomectomy was performed by Amussat in 1840, after a clinical diagnosis of ovarian tumor because pelvic examination showed a pediculate and large uterine leiomyoma.
- The first scientific report of a uterus conserving myomectomy through the vagina appeared in 1845 in the American Journal of Medical Science, accomplished by Washington Atlee, in Pennsylvania.
- In 1898, Alexander Adam presented 11 cases of myomectomy through an abdominal route, in Liverpool.
- In 1940, Carlos R. Círio proposed a technique of the myometrium emptying, called myometrectomy.
Classification
- Uterine leiomyoma may be classified into 3 subtypes according to location:
- Submucosal – lie just beneath the endometrium.
- Intramural – lie within the uterine wall.
- Subserous – lies at the serosal surface of the uterus or may bulge out from the myometrium and can become pedunculated.
Pathophysiology
- The pathogenesis of leiomyoma is characterized by benign smooth muscle neoplasm. They can occur in any organ, but the most common forms occur in the uterus, small bowel and the esophagus.
- The chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma.[2]
- On gross pathology, round, well circumscribed (but not encapsulated), solid nodules that are white or tan, and whorled are characteristic findings of leiomyoma .
- On microscopic histopathological analysis, elongated, spindle-shaped cells with a cigar-shaped nucleus are characteristic findings of leiomyoma.
Uterine Leiomyomata
Uterine fibroids are leiomyomata of the uterine smooth muscle. As with other leiomyomata, they are benign, but may lead to excessive menstrual bleeding (menorrhagia), often cause anemia and may lead to infertility. Enucleation is removal of fibroids without removing the uterus (hysterectomy), which is also commonly performed. Laser surgery (called myolysis) is increasingly used, and provides a viable alternative to surgery. Estrogen and progesterone usually stimulate their growth, and hormone suppression may hence decrease their size.
Esophageal
Leiomyoma of the esophagus is the most common benign esophageal tumour, though this accounts for less than 1% of esophageal neoplasms. The remainder consists mainly of carcinomas. Although the vast majority of benign esophageal tumors are clinically silent and go undetected, large or strategically located tumors may become symptomatic. [3]
Leiomyoma of Jejunum
Leiomyoma is the most common benign tumor of small bowel. Approximately 50% of cases are found in the jejunum, followed by the ileum in 31% of cases. Almost one half of all lesions are less than 5 centimeters. [4]
-
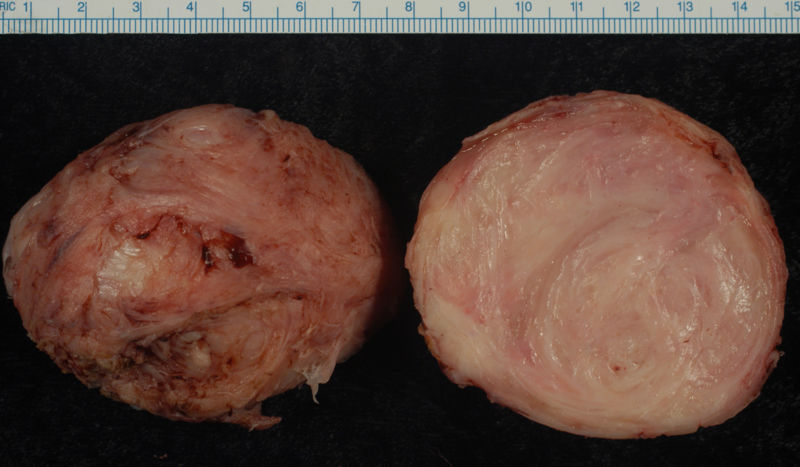
Leiomyoma enucleated from a uterus. External surface on left; cut surface on right
-
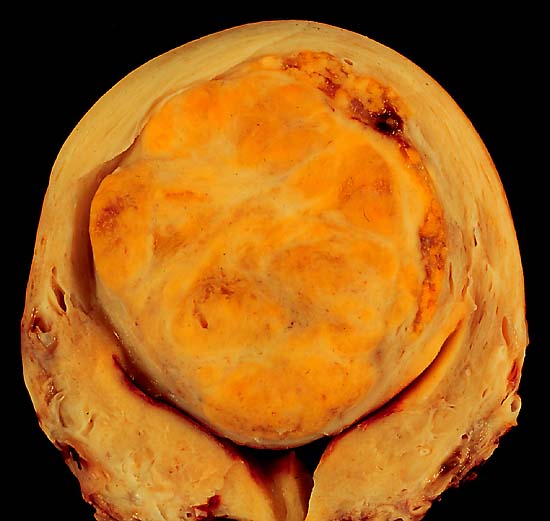
A large, solitary leiomyoma in the uterus, distoring the endometrial cavity into a Y shape by splaying and pressing it downwards.
(Image courtesy of Ed Uthman, MD)


Causes
- Chromosome aberrations such as t(12;14)(q14-q15;q23–24), del(7)(q22q32), rearrangements involving 6p21, 10q, trisomy 12, and deletions of 1p3q have been associated with the development of leiomyoma.
Differentiating Leiomyoma from other Diseases
- Uterine leiomyoma must be differentiated from other diseases that cause uterine mass, such as:
- Uterine adenomyoma
- Pregnancy
- Hematometra
- Uterine sarcoma
- Uterine carcinosarcoma
- Endometrial carcinoma
- Metastasis
Epidemiology and Demographics
Age
- Leiomyoma is more commonly observed among patients aged 40 years and older.
Race
- Leiomyoma usually affects African-American women.
Risk Factors
- Common risk factors in the development of uterine leiomyoma include:
- African-American race
- Early menarche
- Prenatal exposure to diethylstilbestrol
- Having one or more pregnancies extending beyond 20 weeks
- Obesity
- Significant consumption of beef and other reds meats
- Hypertension
- Alcohol consumption
Natural History, Complications and Prognosis
- The majority of patients with uterine leiomyoma remain asymptomatic for decades
- Common complications of uterine leiomyoma include:
- Dysmenorrhea
- Dyspareunia
- Leiomyoma degeneration or torsion
- Transcervical prolapse
- Miscarriage.
Diagnosis
Symptoms
- Leiomyoma is usually asymptomatic.
- Symptoms of uterine leiomyoma may include the following:
- Abnormal gynecologic hemorrhage
- Heavy or painful periods
- Abdominal discomfort or bloating
- Back ache
- Urinary frequency or retention
- Infertility
Physical Examination
- Physical examination may be remarkable for:
- Enlarged, mobile uterus with an irregular contour on bimanual pelvic examination
Imaging Findings
- On ultrasound imaging, uterine leiomyoma is characterized by the fibroids as focal masses with a heterogeneous texture, which usually cause shadowing of the ultrasound beam.
Other Diagnostic Studies
- Uterine leiomyoma may also be diagnosed using diagnostic hysteroscopy, magnetic resonance imaging, and hysterosalpingography.




Patient #1: MR images demonstrate large degenerating leiomyomas





Patient #2: MR images demonstrate a leiomyoma prolapsing into the endometrial canal


Hysterosalpingogram(HSG) reveals a submucosal leiomyoma


Treatment
Medical Therapy
- The mainstay of therapy for uterine leiomyoma is oral contraceptive pills, either combination pills or progestin-only, Gonadotropin-releasing hormone analogs.
Surgery
- Surgery is the mainstay of therapy for uterine leiomyoma.
- Uterine artery embolization in conjunction with laparotomic myomectomy is the most common approach to the treatment of leiomyoma.
- Hysteroscopic myomectomy can also be performed for patients with uterine leiomyoma.
References
- ↑ Bozini, Nilo; Baracat, Edmund C (2007). "The history of myomectomy at the Medical School of University of São Paulo". Clinics. 62 (3). doi:10.1590/S1807-59322007000300002. ISSN 1807-5932.
- ↑ Genetics of Uterine Leiomyomas. glowm (2016). http://www.glowm.com/section_view/heading/Genetics%20of%20Uterine%20Leiomyomas/item/363 Accessed on April 19, 2016
- ↑ James C. Chou, MD & Frank G. Gress, MD. "Benign Esophageal Tumors". Esophageal Cancer Overview (Cancer of the Esophagus). Retrieved 2007-03-21. Unknown parameter
|publsiher=ignored (|publisher=suggested) (help) - ↑ By Michael P. Buetow, M.D. "Leiomyoma of Jejunum". Retrieved 2007-03-21. Unknown parameter
|publsiher=ignored (|publisher=suggested) (help)