Herpes zoster physical examination: Difference between revisions
No edit summary |
No edit summary |
||
| Line 46: | Line 46: | ||
Image:Herpes zoster 7.jpg|[[Plantar]] foot [[rash]] caused by herpes zoster | Image:Herpes zoster 7.jpg|[[Plantar]] foot [[rash]] caused by herpes zoster | ||
Image:Herpes zoster 8.jpg|[[Vesicle|Vesicular]] [[lesion]]s of Herpes zoster | Image:Herpes zoster 8.jpg|[[Vesicle|Vesicular]] [[lesion]]s of Herpes zoster | ||
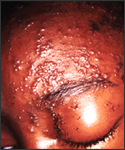
Image:Herpes zoster9.jpg|The [[pathological|pathologic]] changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the [[Varicella zoster virus]] (VZV) pathogen | Image:Herpes zoster9.jpg|The [[pathological|pathologic]] changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the [[Varicella zoster virus]] (VZV) pathogen. | ||
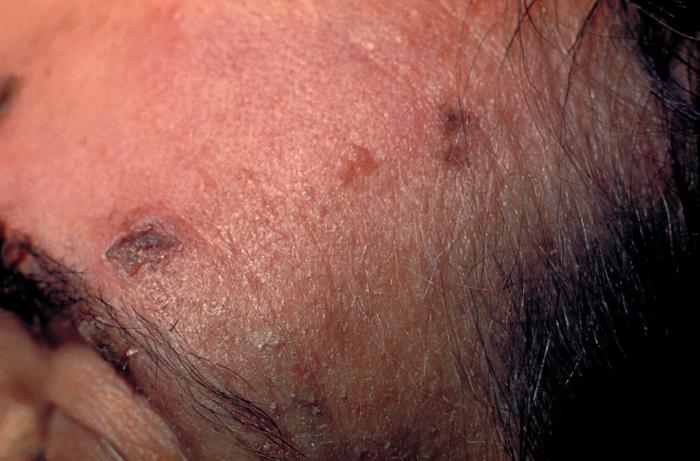
Image:Herpes zoster 10.jpg|The [[pustule|pustulo-]][[vesicle|vesicular]] [[rash]] on this African-American woman’s face, represents a herpes [[outbreak]] due to the [[Varicella zoster virus]] (VZV) pathogen | Image:Herpes zoster 10.jpg|The [[pustule|pustulo-]][[vesicle|vesicular]] [[rash]] on this African-American woman’s face, represents a herpes [[outbreak]] due to the [[Varicella zoster virus]] (VZV) pathogen. | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
Revision as of 18:54, 2 January 2013
|
Herpes zoster Microchapters |
|
Diagnosis |
|---|
|
History and Symptoms |
|
Treatment |
|
Case Studies |
|
Herpes zoster physical examination On the Web |
|
American Roentgen Ray Society Images of Herpes zoster physical examination |
|
Risk calculators and risk factors for Herpes zoster physical examination |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; L. Katie Morrison, MD; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please help WikiDoc by adding more content here. It's easy! Click here to learn about editing.
Physical Examination
People with herpes zoster most commonly have a rash in one or two adjacent dermatomes (localized zoster). The rash most commonly appears on the trunk along a thoracic dermatome. The rash does not usually cross the body’s midline. However, approximately 20% of people have rash that overlaps adjacent dermatomes. Less commonly, the rash can be more widespread and affect three or more dermatomes. This condition is called disseminated zoster. This generally occurs only in people with compromised immune systems. Disseminated zoster can be difficult to distinguish from varicella.
The rash develops into clusters of clear vesicles. New vesicles continue to form over three to five days and progressively dry and crust over. They usually heal in two to four weeks. There may be permanent pigmentation changes and scarring on the skin.
-

Dermatomal involvement of rash
-

Dermatomal involvement of skin rash
-

Herpes zoster on the chest
-

-

Varicella zoster





(Images shown below courtesy of Charlie Goldberg, M.D., UCSD School of Medicine and VA Medical Center, San Diego, CA)
-

-

Herpes Zoster: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-

Herpes Zoster: Dermatomally distributed vesicles in patient with HZV infection.
-

Herpes Zoster: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-
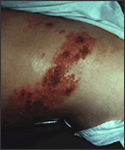
Shingles on waist





-

Herpes Zoster.
(Courtesy of Josh Fierer, M.D. and Charlie Goldberg, M.D.) -

Herpes Zoster C3 Distribution: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-

Herpes Zoster C3 Distribution: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-

Shingles on face
-
Shingles on face





-

Child with shingles who had a history of leukemia
-

-
-

The pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella zoster virus (VZV) pathogen.
-
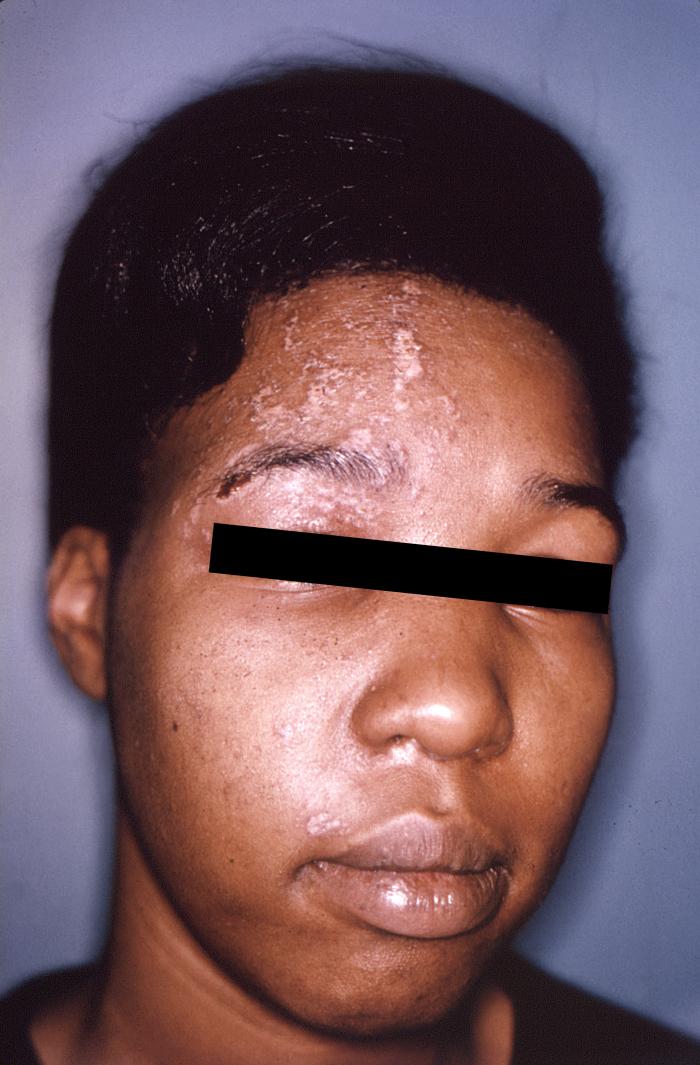
The pustulo-vesicular rash on this African-American woman’s face, represents a herpes outbreak due to the Varicella zoster virus (VZV) pathogen.





-

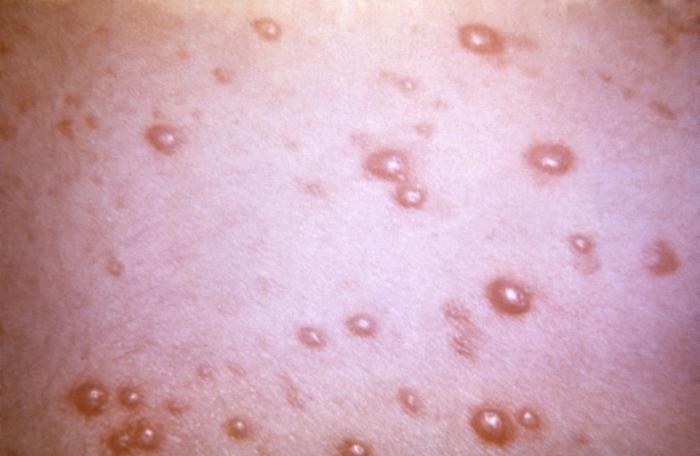
This 1968 image depicted a number of varicella, or chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters, each in a different developmental stage.
-

-

This skin disorder was found to be herpes zoster, not syphilitic in nature as was initially suspected.
-
-

A case of shingles that demonstrates the typical dermatomal distribution, in this case C8/T1




