Herpes zoster physical examination: Difference between revisions
Dima Nimri (talk | contribs) No edit summary |
Dima Nimri (talk | contribs) |
||
| Line 5: | Line 5: | ||
==Overview== | ==Overview== | ||
== Physical Examination == | == Physical Examination == | ||
Physical examination findings of herpes zoster depend on the location of the rash, as well as the stage of the disease: | |||
*Rash: the rash of herpes zoster virus is typically unilateral and does not cross the midline. It follows the distribution of one or two adjacent dermatomes. The rash can involve any area of the body, but most common site are the face ([[ophthalmic]] division of [[trigeminal nerve]]), neck ([[cervical]] dorsal root ganglia) or chest ([[thoracic]] dorsal root ganglia). The rash is initially an erythematous, [[maculopapular]] rash, but over the next 7-10 days, it progresses to pustules and ulceration, with crusts, scabbing or both. Post-inflammatory hyperpigmentation may develop along the affected dermatome(s) as part of the healing process. In the immunocompromised individuals, the rash may be complicated by skin necrosis and scarring.<ref name="pmid23785227">{{cite journal |vauthors=Cohen KR, Salbu RL, Frank J, Israel I |title=Presentation and management of herpes zoster (shingles) in the geriatric population |journal=P T |volume=38 |issue=4 |pages=217–27 |year=2013 |pmid=23785227 |pmc=3684190 |doi= |url=}}</ref><ref name="pmid10375341">{{cite journal |vauthors=Cohen JI, Brunell PA, Straus SE, Krause PR |title=Recent advances in varicella-zoster virus infection |journal=Ann. Intern. Med. |volume=130 |issue=11 |pages=922–32 |year=1999 |pmid=10375341 |doi= |url=}}</ref> | |||
===Gallery=== | ===Gallery=== | ||
Revision as of 15:09, 24 October 2016
|
Herpes zoster Microchapters |
|
Diagnosis |
|---|
|
History and Symptoms |
|
Treatment |
|
Case Studies |
|
Herpes zoster physical examination On the Web |
|
American Roentgen Ray Society Images of Herpes zoster physical examination |
|
Risk calculators and risk factors for Herpes zoster physical examination |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; L. Katie Morrison, MD; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2], Jesus Rosario Hernandez, M.D. [3], Dima Nimri, M.D. [4].
Overview
Physical Examination
Physical examination findings of herpes zoster depend on the location of the rash, as well as the stage of the disease:
- Rash: the rash of herpes zoster virus is typically unilateral and does not cross the midline. It follows the distribution of one or two adjacent dermatomes. The rash can involve any area of the body, but most common site are the face (ophthalmic division of trigeminal nerve), neck (cervical dorsal root ganglia) or chest (thoracic dorsal root ganglia). The rash is initially an erythematous, maculopapular rash, but over the next 7-10 days, it progresses to pustules and ulceration, with crusts, scabbing or both. Post-inflammatory hyperpigmentation may develop along the affected dermatome(s) as part of the healing process. In the immunocompromised individuals, the rash may be complicated by skin necrosis and scarring.[1][2]
Gallery
Skin
(Images shown below courtesy of Charlie Goldberg, M.D., UCSD School of Medicine and VA Medical Center, San Diego, CA)
-

-

Herpes Zoster: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-

Herpes Zoster: Dermatomally distributed vesicles in patient with HZV infection.
-

Herpes Zoster: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-
Shingles on waist
-

Dermatomal involvement of rash
-

Dermatomal involvement of skin rash
-

Herpes zoster on the chest
-

-

Varicella zoster










-

Herpes Zoster.
(Courtesy of Josh Fierer, M.D. and Charlie Goldberg, M.D.) -

Herpes Zoster C3 Distribution: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-

Herpes Zoster C3 Distribution: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-

Shingles on face
-
Shingles on face





-

Child with shingles who had a history of leukemia
-

-
-

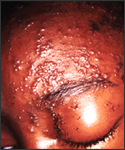
The pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella zoster virus (VZV) pathogen.
-
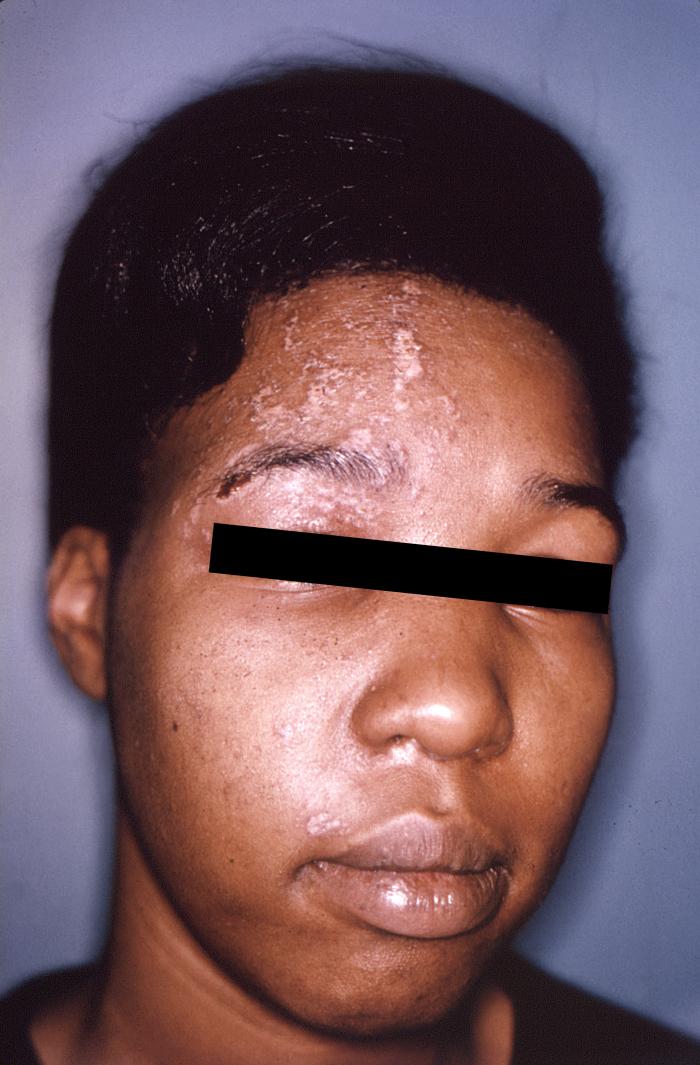
The pustulo-vesicular rash on this African-American woman’s face, represents a herpes outbreak due to the Varicella zoster virus (VZV) pathogen.





-

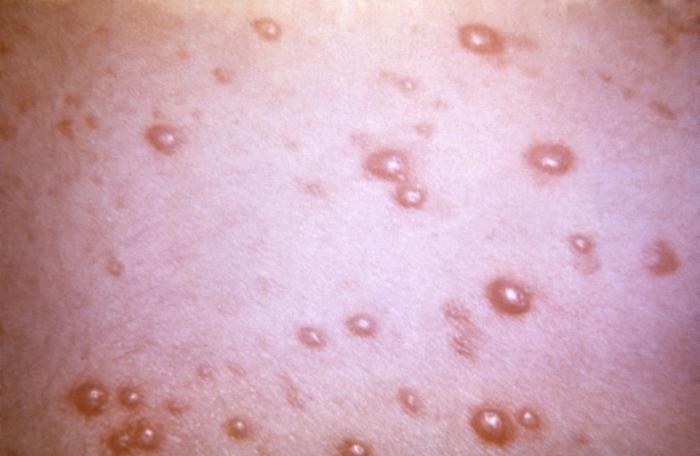
This 1968 image depicted a number of varicella, or chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters, each in a different developmental stage.
-

-

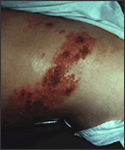
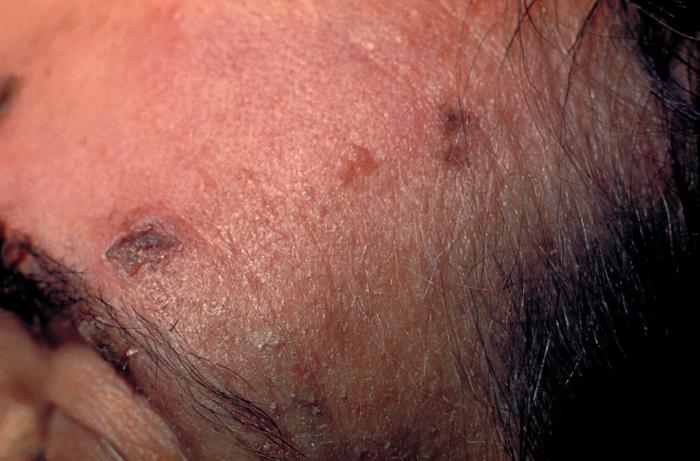
This skin disorder was found to be herpes zoster, not syphilitic in nature as was initially suspected.
-
-

A case of shingles that demonstrates the typical dermatomal distribution, in this case C8/T1





Head


Trunk







Extremities

Neck


Genitourinary System




Skin
(Images shown below courtesy of Charlie Goldberg, M.D., UCSD School of Medicine and VA Medical Center, San Diego, CA)
-
-
Herpes Zoster: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-
Herpes Zoster: Dermatomally distributed vesicles in patient with HZV infection.
-
Herpes Zoster: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-
Shingles on waist
-
Dermatomal involvement of rash
-
Dermatomal involvement of skin rash
-
Herpes zoster on the chest
-
-
Varicella zoster
-
Herpes Zoster.
(Courtesy of Josh Fierer, M.D. and Charlie Goldberg, M.D.) -
Herpes Zoster C3 Distribution: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-
Herpes Zoster C3 Distribution: Dermatomally distributed vesicles, many of which have coalesced, in patient with HZV infection.
-
Shingles on face
-
Shingles on face
-
Child with shingles who had a history of leukemia
-
-
-
The pathologic changes seen on the surface of the right unilateral side of this elderly male patient’s tongue and chin, represent a herpes outbreak due to the Varicella zoster virus (VZV) pathogen.
-
The pustulo-vesicular rash on this African-American woman’s face, represents a herpes outbreak due to the Varicella zoster virus (VZV) pathogen.
-
This 1968 image depicted a number of varicella, or chickenpox lesions on a patient’s back, which were displaying the characteristic “cropping” distribution, or manifesting themselves in clusters, each in a different developmental stage.
-
-
This skin disorder was found to be herpes zoster, not syphilitic in nature as was initially suspected.
-
-
A case of shingles that demonstrates the typical dermatomal distribution, in this case C8/T1
Gallery
-
![Skin disorder was found to be herpes zoster. From Public Health Image Library (PHIL). [3]](/images/d/d6/Chickenpox31.jpeg)
Skin disorder was found to be herpes zoster. From Public Health Image Library (PHIL). [3]
-
![Plantar foot rash was suspected to be smallpox related, but was later determined to be caused by herpes zoster virus. From Public Health Image Library (PHIL). [3]](/images/5/5a/Chickenpox30.jpeg)
Plantar foot rash was suspected to be smallpox related, but was later determined to be caused by herpes zoster virus. From Public Health Image Library (PHIL). [3]
![Skin disorder was found to be herpes zoster. From Public Health Image Library (PHIL). [3]](/index.php/File:Chickenpox31.jpeg)
![Plantar foot rash was suspected to be smallpox related, but was later determined to be caused by herpes zoster virus. From Public Health Image Library (PHIL). [3]](/index.php/File:Chickenpox30.jpeg)
References
- ↑ Cohen KR, Salbu RL, Frank J, Israel I (2013). "Presentation and management of herpes zoster (shingles) in the geriatric population". P T. 38 (4): 217–27. PMC 3684190. PMID 23785227.
- ↑ Cohen JI, Brunell PA, Straus SE, Krause PR (1999). "Recent advances in varicella-zoster virus infection". Ann. Intern. Med. 130 (11): 922–32. PMID 10375341.
- ↑ 3.0 3.1 "Public Health Image Library (PHIL)".