Donepezil
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Donepezil is a reversible inhibitor of the enzyme acetylcholinesterase that is FDA approved for the {{{indicationType}}} of dementia of the Alzheimer's type. Common adverse reactions include hypertension, syncope, weight decreased, diarrhea, loss of appetite, nausea, vomiting, contusion, asthenia, depression and urinary incontinence.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Dementia of the Alzheimer's type
- Dosing Information
- The dosages of ARICEPT® shown to be effective in controlled clinical trials are 5 mg and 10 mg administered once per day.
- The higher dose of 10 mg did not provide a statistically significantly greater clinical benefit than 5 mg. There is a suggestion, however, based upon order of group mean scores and dose trend analyses of data from these clinical trials, that a daily dose of 10 mg of ARICEPT® might provide additional benefit for some patients. Accordingly, whether or not to employ a dose of 10 mg is a matter of prescriber and patient preference.
- Evidence from the controlled trials indicates that the 10 mg dose, with a one week titration, is likely to be associated with a higher incidence of cholinergic adverse events than the 5 mg dose. In open label trials using a 6 week titration, the frequency of these same adverse events was similar between the 5 mg and 10 mg dose groups. Therefore, because steady state is not achieved for 15 days and because the incidence of untoward effects may be influenced by the rate of dose escalation, treatment with a dose of 10 mg should not be contemplated until patients have been on a daily dose of 5 mg for 4 to 6 weeks.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Donepezil in adult patients.
Non–Guideline-Supported Use
Multi-infarct dementia
- Dosing Information
- Donepezil 5 to 10 mg daily for 24 weeks.
Alzheimer's disease - Dementia (Mild to Moderate)
- Dosing Information
- Donepezil 10 mg/day.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Donepezil in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Donepezil in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Donepezil in pediatric patients.
Contraindications
- ARICEPT® is contraindicated in patients with known hypersensitivity to donepezil hydrochloride or to piperidine derivatives.
Warnings
Precautions
- Anesthesia
- ARICEPT®, as a cholinesterase inhibitor, is likely to exaggerate succinylcholine-type muscle relaxation during anesthesia.
- Cardiovascular Conditions
- Because of their pharmacological action, cholinesterase inhibitors may have vagotonic effects on the sinoatrial and atrioventricular nodes. This effect may manifest as bradycardia or heart block in patients both with and without known underlying cardiac conduction abnormalities. Syncopal episodes have been reported in association with the use of ARICEPT®.
- Gastrointestinal Conditions
- Through their primary action, cholinesterase inhibitors may be expected to increase gastric acid secretion due to increased cholinergic activity. Therefore, patients should be monitored closely for symptoms of active or occult gastrointestinal bleeding, especially those at increased risk for developing ulcers, e.g., those with a history of ulcer disease or those receiving concurrent nonsteroidal anti-inflammatory drugs (NSAIDS). Clinical studies of ARICEPT® have shown no increase, relative to placebo, in the incidence of either peptic ulcer disease or gastrointestinal bleeding.
- ARICEPT®, as a predictable consequence of its pharmacological properties, has been shown to produce diarrhea, nausea and vomiting. These effects, when they occur, appear more frequently with the 10 mg/day dose than with the 5 mg/day dose. In most cases, these effects have been mild and transient, sometimes lasting one to three weeks, and have resolved during continued use of ARICEPT®.
- Genitourinary
- Although not observed in clinical trials of ARICEPT®, cholinomimetics may cause bladder outflow obstruction.
- Neurological Conditions
- Seizures: Cholinomimetics are believed to have some potential to cause generalized convulsions. However, seizure activity also may be a manifestation of Alzheimer's Disease.
- Pulmonary Conditions
- Because of their cholinomimetic actions, cholinesterase inhibitors should be prescribed with care to patients with a history of asthma or obstructive pulmonary disease.
- Sulfites
- ARICEPT® Oral Solution contains sodium metabisulfite, a sulfite that may cause allergic-type reactions including anaphylactic symptoms and life-threatening or less severe asthmatic episodes in certain susceptible people. The overall prevalence of sulfite sensitivity in the general population is unknown and probably low. Sulfite sensitivity is seen more frequently in asthmatic than nonasthmatic people.
Adverse Reactions
Clinical Trials Experience
Mild to Moderate Alzheimer's Disease Trials
- Adverse Events Leading to Discontinuation
- The rates of discontinuation from controlled clinical trials of ARICEPT® due to adverse events for the ARICEPT® 5 mg/day treatment groups were comparable to those of placebo-treatment groups at approximately 5%. The rate of discontinuation of patients who received 7-day escalations from 5 mg/day to 10 mg/day, was higher at 13%.
- The most common adverse events leading to discontinuation, defined as those occurring in at least 2% of patients and at twice the incidence seen in placebo patients, are shown in Table 1.
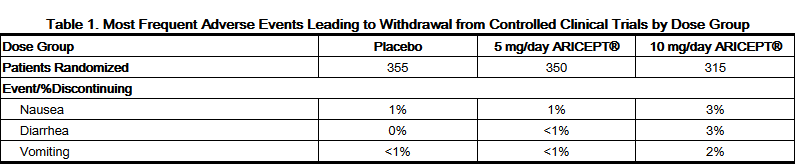
This image is provided by the National Library of Medicine.

- Most Frequent Adverse Clinical Events Seen in Association with the Use of ARICEPT®
- The most common adverse events, defined as those occurring at a frequency of at least 5% in patients receiving 10 mg/day and twice the placebo rate, are largely predicted by ARICEPT®'s cholinomimetic effects. These include nausea, diarrhea, insomnia, vomiting, muscle cramp, fatigue and anorexia. These adverse events were often of mild intensity and transient, resolving during continued ARICEPT® treatment without the need for dose modification.
- There is evidence to suggest that the frequency of these common adverse events may be affected by the rate of titration. An open-label study was conducted with 269 patients who received placebo in the 15 and 30-week studies. These patients were titrated to a dose of 10 mg/day over a 6-week period. The rates of common adverse events were lower than those seen in patients titrated to 10 mg/day over one week in the controlled clinical trials and were comparable to those seen in patients on 5 mg/day.
- See Table 2 for a comparison of the most common adverse events following one and six week titration regimens.

This image is provided by the National Library of Medicine.

- Adverse Events Reported in Controlled Trials
- The events cited reflect experience gained under closely monitored conditions of clinical trials in a highly selected patient population. In actual clinical practice or in other clinical trials, these frequency estimates may not apply, as the conditions of use, reporting behavior, and the kinds of patients treated may differ. Table 3 lists treatment emergent signs and symptoms that were reported in at least 2% of patients in placebo-controlled trials who received ARICEPT® and for which the rate of occurrence was greater for ARICEPT® assigned than placebo assigned patients. In general, adverse events occurred more frequently in female patients and with advancing age.

This image is provided by the National Library of Medicine.

- Other Adverse Events Observed During Clinical Trials
- ARICEPT® has been administered to over 1700 individuals during clinical trials worldwide. Approximately 1200 of these patients have been treated for at least 3 months and more than 1000 patients have been treated for at least 6 months. Controlled and uncontrolled trials in the United States included approximately 900 patients. In regards to the highest dose of 10 mg/day, this population includes 650 patients treated for 3 months, 475 patients treated for 6 months and 116 patients treated for over 1 year. The range of patient exposure is from 1 to 1214 days.
- Treatment emergent signs and symptoms that occurred during 3 controlled clinical trials and two open-label trials in the United States were recorded as adverse events by the clinical investigators using terminology of their own choosing. To provide an overall estimate of the proportion of individuals having similar types of events, the events were grouped into a smaller number of standardized categories using a modified COSTART dictionary and event frequencies were calculated across all studies. These categories are used in the listing below. The frequencies represent the proportion of 900 patients from these trials who experienced that event while receiving ARICEPT®. All adverse events occurring at least twice are included, except for those already listed in Tables 2 or 3, COSTART terms too general to be informative, or events less likely to be drug caused. Events are classified by body system and listed using the following definitions: frequent adverse events - those occurring in at least 1/100 patients; infrequent adverse events - those occurring in 1/100 to 1/1000 patients. These adverse events are not necessarily related to ARICEPT® treatment and in most cases were observed at a similar frequency in placebo-treated patients in the controlled studies. No important additional adverse events were seen in studies conducted outside the United States.
- Body as a Whole:Frequent: influenza, chest pain, toothache; Infrequent: fever, edema face, periorbital edema, hernia hiatal, abscess, cellulitis, chills, generalized coldness, head fullness, listlessness.
- Cardiovascular System:Frequent: hypertension, vasodilation, atrial fibrillation, hot flashes, hypotension; Infrequent: angina pectoris,postural hypotension, myocardial infarction, AV block (first degree), congestive heart failure, arteritis, bradycardia, peripheral vascular disease, supraventricular tachycardia, deep vein thrombosis.
- Digestive System:Frequent: fecal incontinence, gastrointestinal bleeding, bloating, epigastric pain; Infrequent: eructation, gingivitis, increased appetite, flatulence, periodontal abscess, cholelithiasis, diverticulitis, drooling, dry mouth, fever sore, gastritis, irritable colon, tongue edema, epigastric distress, gastroenteritis, increased transaminases, hemorrhoids, ileus, increased thirst, jaundice, melena, polydipsia, duodenal ulcer, stomach ulcer.
- Endocrine System:Infrequent: diabetes mellitus, goiter.
- Hemic and Lymphatic System:Infrequent: anemia, thrombocythemia, thrombocytopenia, eosinophilia, erythrocytopenia.
- Metabolic and Nutritional Disorders:Frequent: dehydration; Infrequent: gout, hypokalemia, increased creatine kinase, hyperglycemia, weight increase, increased lactate dehydrogenase.
- Musculoskeletal System:Frequent: bone fracture; Infrequent: muscle weakness, muscle fasciculation.
- Nervous System:Frequent: delusions, tremor, irritability, paresthesia, aggression, vertigo, ataxia, increased libido, restlessness, abnormal crying, nervousness, aphasia; Infrequent: cerebrovascular accident, intracranial hemorrhage, transient ischemic attack, emotional lability, neuralgia, coldness (localized), muscle spasm, dysphoria, gait abnormality, hypertonia, hypokinesia, neurodermatitis, numbness (localized), paranoia, dysarthria, dysphasia, hostility, decreased libido, melancholia, emotional withdrawal, nystagmus, pacing.
- Respiratory System:Frequent: dyspnea, sore throat, bronchitis; Infrequent: epistaxis, post nasal drip, pneumonia, hyperventilation, pulmonary congestion, wheezing, hypoxia, pharyngitis, pleurisy, pulmonary collapse, sleep apnea, snoring.
- Skin and Appendages:Frequent: pruritus, diaphoresis, urticaria; Infrequent: dermatitis, erythema, skin discoloration, hyperkeratosis, alopecia, fungal dermatitis, herpes zoster, hirsutism, skin striae, night sweats, skin ulcer.
- Special Senses:Frequent: cataract, eye irritation, vision blurred; Infrequent: dry eyes, glaucoma, earache, tinnitus, blepharitis, decreased hearing, retinal hemorrhage, otitis externa, otitis media, bad taste, conjunctival hemorrhage, ear buzzing, motion sickness, spots before eyes.
- Urogenital System:Frequent: urinary incontinence, nocturia; Infrequent: dysuria, hematuria, urinary urgency, metrorrhagia, cystitis, enuresis, prostate hypertrophy, pyelonephritis, inability to empty bladder, breast fibroadenosis, fibrocystic breast, mastitis, pyuria, renal failure, vaginitis.
Severe Alzheimer's Disease
- Adverse Events Leading to Discontinuation
- The rates of discontinuation from controlled clinical trials of ARICEPT® due to adverse events for the ARICEPT® patients were approximately 12% compared to 7% for placebo patients.
- The most common adverse events leading to discontinuation, defined as those occurring in at least 2% of ARICEPT® patients and at twice the incidence seen in placebo patients, were anorexia (2% vs 1% placebo), nausea (2% vs <1% placebo), diarrhea (2% vs 0% placebo) and urinary tract infection (2% vs 1% placebo).
- Most Frequent Adverse Clinical Events Seen in Association with the Use of ARICEPT®
- The most common adverse events, defined as those occurring at a frequency of at least 5% in patients receiving ARICEPT® and twice the placebo rate, are largely predicted by ARICEPT®'s cholinomimetic effects. These include diarrhea, anorexia, vomiting, nausea, and ecchymosis. These adverse events were often of mild intensity and transient, resolving during continued ARICEPT® treatment without the need for dose modification.
- Adverse Events Reported in Controlled Trials
- Table 4 lists treatment emergent signs and symptoms that were reported in at least 2% of patients in placebo-controlled trials who received ARICEPT® and for which the rate of occurrence was greater for ARICEPT® assigned than placebo assigned patients.

This image is provided by the National Library of Medicine.

- Other Adverse Events Observed During Clinical Trials
- ARICEPT® has been administered to over 600 patients with severe Alzheimer's Disease during clinical trials of at least 6 months duration, including 3 double blind placebo controlled trials, one of which had an open label extension. All adverse events occurring at least twice are included, except for those already listed in Table 4, COSTART terms too general to be informative, or events less likely to be drug caused. Events are classified by body system using the COSTART dictionary and listed using the following definitions: frequent adverse events - those occurring in at least 1/100 patients; infrequent adverse events - those occurring in 1/100 to 1/1000 patients. These adverse events are not necessarily related to ARICEPT® treatment and in most cases were observed at a similar frequency in placebo-treated patients in the controlled studies.
- Body as a Whole:Frequent: abdominal pain, asthenia, fungal infection, flu syndrome; Infrequent: allergic reaction, cellulitis, malaise, sepsis, face edema, hernia.
- Cardiovascular System:Frequent: hypotension, bradycardia, ECG abnormal, heart failure; Infrequent: myocardial infarction, angina pectoris, atrial fibrillation, congestive heart failure, peripheral vascular disorder, supraventricular extrasystoles, ventricular extrasystoles, cardiomegaly.
- Digestive System:Frequent: constipation, gastroenteritis, fecal incontinence, dyspepsia; Infrequent: gamma glutamyl transpeptidase increase, gastritis, dysphagia, periodontitis, stomach ulcer, periodontal abscess, flatulence, liver function tests abnormal, eructation, esophagitis, rectal hemorrhage.
- Endocrine System:Infrequent: diabetes mellitus.
- Hemic and Lymphatic System:Frequent: anemia; Infrequent: leukocytosis.
- Metabolic and Nutritional Disorders:Frequent: weight loss, peripheral edema, edema, lactic dehydrogenase increased, alkaline phosphatase increased; Infrequent hypercholesteremia, hypokalemia, hypoglycemia, weight gain, bilirubinemia, BUN increased, B12 deficiency anemia, cachexia, creatinine increased, gout, hyponatremia, hypoproteinemia, iron deficiency anemia, SGOT increased, SGPT increased.
- Musculoskeletal System:Frequent: arthritis; Infrequent: arthrosis, bone fracture, arthralgia, leg cramps, osteoporosis, myalgia.
- Nervous System:Frequent: agitation, anxiety, tremor, convulsion, wandering, abnormal gait; Infrequent: apathy, vertigo, delusions, abnormal dreams, cerebrovascular accident, increased salivation, ataxia, euphoria, vasodilatation, cerebral hemorrhage, cerebral infarction, cerebral ischemia, dementia, extrapyramidal syndrome, grand mal convulsion, hemiplegia, hypertonia, hypokinesia.
- Respiratory System:Frequent: pharyngitis, pneumonia, cough increased, bronchitis; Infrequent: dyspnea, rhinitis, asthma.
- Skin and Appendages:Frequent: rash, skin ulcer, pruritus; Infrequent: psoriasis, skin discoloration, herpes zoster, dry skin, sweating, urticaria, vesiculobullous rash
- Special Senses:Infrequent: conjunctivitis, glaucoma, abnormal vision, ear pain, lacrimation disorder.
- Urogenital System:Frequent: urinary tract infection, cystitis, hematuria, glycosuria; Infrequent: vaginitis, dysuria, urinary frequency, albuminuria.
Postmarketing Experience
- Voluntary reports of adverse events temporally associated with ARICEPT® that have been received since market introduction that are not listed above, and that there is inadequate data to determine the causal relationship with the drug include the following: abdominal pain, agitation, cholecystitis, confusion, convulsions, hallucinations, heart block (all types), hemolytic anemia, hepatitis, hyponatremia, neuroleptic malignant syndrome, pancreatitis, and rash.
Drug Interactions
- Effect of ARICEPT® on the Metabolism of Other Drugs
- No in vivo clinical trials have investigated the effect of ARICEPT® on the clearance of drugs metabolized by CYP 3A4 (e.g. cisapride, terfenadine) or by CYP 2D6 (e.g. imipramine). However, in vitro studies show a low rate of binding to these enzymes (mean Ki about 50-130 μM), that, given the therapeutic plasma concentrations of donepezil (164 nM), indicates little likelihood of interference.
- Whether ARICEPT® has any potential for enzyme induction is not known.
- Formal pharmacokinetic studies evaluated the potential of ARICEPT® for interaction with theophylline, cimetidine, warfarin and digoxin. No significant effects on the pharmacokinetics of these drugs were observed..
- Effect of Other Drugs on the Metabolism of ARICEPT®
- Ketoconazole and quinidine, inhibitors of CYP450, 3A4 and 2D6, respectively, inhibit donepezil metabolism in vitro. Whether there is a clinical effect of these inhibitors is not known. In a 7-day crossover study in 18 healthy volunteers, ketoconazole (200mg q.d.) increased mean donepezil (5mg q.d.) concentrations (AUC0-24 and Cmax) by 36%. The clinical relevance of this increase in concentration is unknown.
- Inducers of CYP 2D6 and CYP 3A4 (e.g., phenytoin, carbamazepine, dexamethasone, rifampin, and phenobarbital) could increase the rate of elimination of ARICEPT®.
- Formal pharmacokinetic studies demonstrated that the metabolism of ARICEPT® is not significantly affected by concurrent administration of digoxin or cimetidine.
- Use with Anticholinergics
- Because of their mechanism of action, cholinesterase inhibitors have the potential to interfere with the activity of anticholinergic medications.
- Use with Cholinomimetics and Other Cholinesterase Inhibitors
- A synergistic effect may be expected when cholinesterase inhibitors are given concurrently with succinylcholine, similar neuromuscular blocking agents or cholinergic agonists such as bethanechol.
Use in Specific Populations
Pregnancy
- Pregnancy Category C
- Teratology studies conducted in pregnant rats at doses up to 16 mg/kg/day (approximately 13 times the maximum recommended human dose on a mg/m2 basis) and in pregnant rabbits at doses up to 10 mg/kg/day (approximately 16 times the maximum recommended human dose on a mg/m2 basis) did not disclose any evidence for a teratogenic potential of donepezil. However, in a study in which pregnant rats were given up to 10 mg/kg/day (approximately 8 times the maximum recommended human dose on a mg/m2 basis) from day 17 of gestation through day 20 postpartum, there was a slight increase in still births and a slight decrease in pup survival through day 4 postpartum at this dose; the next lower dose tested was 3 mg/kg/day. There are no adequate or well-controlled studies in pregnant women. ARICEPT® should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Donepezil in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Donepezil during labor and delivery.
Nursing Mothers
- It is not known whether donepezil is excreted in human breast milk. ARICEPT® has no indication for use in nursing mothers.
Pediatric Use
- There are no adequate and well-controlled trials to document the safety and efficacy of ARICEPT® in any illness occurring in children.
Geriatic Use
- Alzheimer's disease is a disorder occurring primarily in individuals over 55 years of age. The mean age of patients enrolled in the clinical studies with ARICEPT® was 73 years; 80% of these patients were between 65 and 84 years old and 49% of patients were at or above the age of 75. The efficacy and safety data presented in the clinical trials section were obtained from these patients. There were no clinically significant differences in most adverse events reported by patient groups ≥ 65 years old and < 65 years old.
Gender
There is no FDA guidance on the use of Donepezil with respect to specific gender populations.
Race
There is no FDA guidance on the use of Donepezil with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Donepezil in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Donepezil in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Donepezil in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Donepezil in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
There is limited information regarding Monitoring of Donepezil in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Donepezil in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- Because strategies for the management of overdose are continually evolving, it is advisable to contact a Poison Control Center to determine the latest recommendations for the management of an overdose of any drug.
- As in any case of overdose, general supportive measures should be utilized. Overdosage with cholinesterase inhibitors can result in cholinergic crisis characterized by severe nausea, vomiting, salivation, sweating, bradycardia, hypotension, respiratory depression, collapse and convulsions. Increasing muscle weakness is a possibility and may result in death if respiratory muscles are involved. Atypical responses in blood pressure and heart rate have been reported with other cholinomimetics when co-administered with quaternary anticholinergics such as glycopyrrolate. It is not known whether ARICEPT® and/or its metabolites can be removed by dialysis (hemodialysis, peritoneal dialysis, or hemofiltration).
- Dose-related signs of toxicity in animals included reduced spontaneous movement, prone position, staggering gait, lacrimation, clonic convulsions, depressed respiration, salivation, miosis, tremors, fasciculation and lower body surface temperature.
Management
- Tertiary anticholinergics such as atropine may be used as an antidote for ARICEPT® overdosage. Intravenous atropine sulfate titrated to effect is recommended: an initial dose of 1.0 to 2.0 mg IV with subsequent doses based upon clinical response.
Chronic Overdose
There is limited information regarding Chronic Overdose of Donepezil in the drug label.
Pharmacology

| |
1 : 1 mixture (racemate)Donepezil
| |
| Systematic (IUPAC) name | |
| (RS)-2-[(1-benzyl-4-piperidyl)methyl]- 5,6-dimethoxy-2,3-dihydroinden-1-one | |
| Identifiers | |
| CAS number | |
| ATC code | N06 |
| PubChem | |
| DrugBank | |
| Chemical data | |
| Formula | Template:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox |
| Mol. mass | 379.492 g/mol |
| SMILES | & |
| Pharmacokinetic data | |
| Bioavailability | 100 (%) |
| Protein binding | 96% |
| Metabolism | ? |
| Half life | 70 hours |
| Excretion | 0,11-0,13 (l/h/kg) |
| Therapeutic considerations | |
| Pregnancy cat. |
C |
| Legal status |
Template:Unicode Prescription only |
| Routes | Oral tablet, 5,10 & 23mg |
Mechanism of Action
- Donepezil hydrochloride is postulated to exert its therapeutic effect by enhancing cholinergic function. This is accomplished by increasing the concentration of acetylcholine through reversible inhibition of its hydrolysis by acetylcholinesterase. There is no evidence that donepezil alters the course of the underlying dementing process.
Structure
- ARICEPT® (donepezil hydrochloride) is a reversible inhibitor of the enzyme acetylcholinesterase, known chemically as (±)-2,3-dihydro-5,6-dimethoxy-2-[1-(phenylmethyl)-4-piperidinyl]methyl]-1H-inden-1-one hydrochloride. Donepezil hydrochloride is commonly referred to in the pharmacological literature as E2020. It has an empirical formula of C24H29NO3HCl and a molecular weight of 415.96. Donepezil hydrochloride is a white crystalline powder and is freely soluble in chloroform, soluble in water and in glacial acetic acid, slightly soluble in ethanol and in acetonitrile and practically insoluble in ethyl acetate and in n-hexane.

This image is provided by the National Library of Medicine.

- Each 1mL of ARICEPT® Oral Solution contains 1 mg of donepezil hydrochloride. ARICEPT® Oral Solution also contains sorbitol solution 70%, povidone K-30, citric acid anhydrous, sodium citrate dihydrate, sodium benzoate, methylparaben, propylene glycol, sodium metabisulfite, purified water and strawberry flavor.
Pharmacodynamics
- Current theories on the pathogenesis of the cognitive signs and symptoms of Alzheimer's Disease attribute some of them to a deficiency of cholinergic neurotransmission. Donepezil hydrochloride is postulated to exert its therapeutic effect by enhancing cholinergic function. This is accomplished by increasing the concentration of acetylcholine through reversible inhibition of its hydrolysis by acetylcholinesterase. There is no evidence that donepezil alters the course of the underlying dementing process.
Pharmacokinetics
- ARICEPT® Oral Solution is bioequivalent to ARICEPT® Tablets. Donepezil is well absorbed with a relative oral bioavailability of 100% and reaches peak plasma concentrations in 3 to 4 hours. Pharmacokinetics are linear over a dose range of 1-10 mg given once daily. Neither food nor time of administration (morning vs. evening dose) influences the rate or extent of absorption of ARICEPT® Tablets. Administration of ARICEPT® Oral Solution to healthy volunteers with a high-fat meal decreased Cmax by 17% and increased Tmax by 1 hour, while the AUC0-72 was similar under fed and fasted conditions. This delay in absorption and decrease in exposure is not likely to be clinically significant; therefore ARICEPT® Oral Solution can be taken without regard to meals.
- The elimination half life of donepezil is about 70 hours and the mean apparent plasma clearance (Cl/F) is 0.13 L/hr/kg. Following multiple dose administration, donepezil accumulates in plasma by 4-7 fold and steady state is reached within 15 days. The steady state volume of distribution is 12 L/kg. Donepezil is approximately 96% bound to human plasma proteins, mainly to albumins (about 75%) and alpha1 - acid glycoprotein (about 21%) over the concentration range of 2-1000 ng/mL.
- Donepezil is both excreted in the urine intact and extensively metabolized to four major metabolites, two of which are known to be active, and a number of minor metabolites, not all of which have been identified. Donepezil is metabolized by CYP 450 isoenzymes 2D6 and 3A4 and undergoes glucuronidation. Following administration of 14C-labeled donepezil, plasma radioactivity, expressed as a percent of the administered dose, was present primarily as intact donepezil (53%) and as 6-O-desmethyl donepezil (11%), which has been reported to inhibit AChE to the same extent as donepezil in vitro and was found in plasma at concentrations equal to about 20% of donepezil. Approximately 57% and 15% of the total radioactivity was recovered in urine and feces, respectively, over a period of 10 days, while 28% remained unrecovered, with about 17% of the donepezil dose recovered in the urine as unchanged drug.
- Special Populations
- Hepatic Disease
- In a study of 10 patients with stable alcoholic cirrhosis, the clearance of ARICEPT® was decreased by 20% relative to 10 healthy age and sex matched subjects.
- Renal Disease
- In a study of 4 patients with moderate to severe renal impairment (ClCr< 22 mL/min/1.73 m2) the clearance of ARICEPT® did not differ from 4 age and sex matched healthy subjects.
- Age
- No formal pharmacokinetic study was conducted to examine age related differences in the pharmacokinetics of ARICEPT®. However, mean plasma ARICEPT® concentrations measured during therapeutic drug monitoring of elderly patients with Alzheimer's Disease are comparable to those observed in young healthy volunteers.
- Gender and Race
- No specific pharmacokinetic study was conducted to investigate the effects of gender and race on the disposition of ARICEPT®. However, retrospective pharmacokinetic analysis indicates that gender and race (Japanese and Caucasians) did not affect the clearance of ARICEPT®.
- Drug-Drug Interactions
- Drugs Highly Bound to Plasma Proteins
- Drug displacement studies have been performed in vitro between this highly bound drug (96%) and other drugs such as furosemide, digoxin, and warfarin. ARICEPT® at concentrations of 0.3-10 μg/mL did not affect the binding of furosemide (5 μg/mL), digoxin (2 ng/mL), and warfarin (3 μg/mL) to human albumin. Similarly, the binding of ARICEPT® to human albumin was not affected by furosemide, digoxin and warfarin.
- Effect of ARICEPT® on the Metabolism of Other Drugs
- No in vivo clinical trials have investigated the effect of ARICEPT® on the clearance of drugs metabolized by CYP 3A4 (e.g. cisapride, terfenadine) or by CYP 2D6 (e.g. imipramine). However, in vitro studies show a low rate of binding to these enzymes (mean Ki about 50-130 μM), that, given the therapeutic plasma concentrations of donepezil (164 nM), indicates little likelihood of interference.
- Whether ARICEPT® has any potential for enzyme induction is not known.
- Formal pharmacokinetic studies evaluated the potential of ARICEPT® for interaction with theophylline, cimetidine, warfarin and digoxin. No significant effects on the pharmacokinetics of these drugs were observed.
- Effect of Other Drugs on the Metabolism of ARICEPT®
- Ketoconazole and quinidine, inhibitors of CYP450, 3A4 and 2D6, respectively, inhibit donepezil metabolism in vitro. Whether there is a clinical effect of quinidine is not known. In a 7-day crossover study in 18 healthy volunteers, ketoconazole (200mg q.d.) increased mean donepezil (5mg q.d.) concentrations (AUC0-24 and Cmax) by 36%. The clinical relevance of this increase in concentration is unknown.
- Inducers of CYP 2D6 and CYP 3A4 (e.g., phenytoin, carbamazepine, dexamethasone, rifampin, and phenobarbital) could increase the rate of elimination of ARICEPT®.
- Formal pharmacokinetic studies demonstrated that the metabolism of ARICEPT® is not significantly affected by concurrent administration of digoxin or cimetidine.
Nonclinical Toxicology
- No evidence of a carcinogenic potential was obtained in an 88-week carcinogenicity study of donepezil hydrochloride conducted in CD-1 mice at doses up to 180 mg/kg/day (approximately 90 times the maximum recommended human dose on a mg/m2 basis), or in a 104-week carcinogenicity study in Sprague-Dawley rats at doses up to 30mg/kg/day (approximately 30 times the maximum recommended human dose on a mg/m2 basis).
- Donepezil was not mutagenic in the Ames reverse mutation assay in bacteria, or in a mouse lymphoma forward mutation assay in vitro. In the chromosome aberration test in cultures of Chinese hamster lung (CHL) cells, some clastogenic effects were observed. Donepezil was not clastogenic in the in vivo mouse micronucleus test and was not genotoxic in an in vivo unscheduled DNA synthesis assay in rats.
- Donepezil had no effect on fertility in rats at doses up to 10 mg/kg/day (approximately 8 times the maximum recommended human dose on a mg/m2 basis).
Clinical Studies
- The effectiveness of ARICEPT® as a treatment for Alzheimer's Disease is demonstrated by the results of randomized, double-blind, placebo-controlled clinical investigations in mild, moderate and severe patients with Alzheimer's Disease.
- Mild-Moderate Alzheimer's Disease
- The effectiveness of ARICEPT® as a treatment for Alzheimer's Disease is demonstrated by the results of two randomized, double-blind, placebo-controlled clinical investigations in patients with Alzheimer's Disease (diagnosed by NINCDS and DSM III-R criteria, Mini-Mental State Examination ≥ 10 and ≤ 26 and Clinical Dementia Rating of 1 or 2). The mean age of patients participating in ARICEPT® trials was 73 years with a range of 50 to 94. Approximately 62% of patients were women and 38% were men. The racial distribution was white 95%, black 3% and other races 2%.
- Study Outcome Measures
- In each study, the effectiveness of treatment with ARICEPT® was evaluated using a dual outcome assessment strategy.
- The ability of ARICEPT® to improve cognitive performance was assessed with the cognitive subscale of the Alzheimer's Disease Assessment Scale (ADAS-cog), a multi-item instrument that has been extensively validated in longitudinal cohorts of Alzheimer's Disease patients. The ADAS-cog examines selected aspects of cognitive performance including elements of memory, orientation, attention, reasoning, language and praxis. The ADAS-cog scoring range is from 0 to 70, with higher scores indicating greater cognitive impairment. Elderly normal adults may score as low as 0 or 1, but it is not unusual for non-demented adults to score slightly higher.
- The patients recruited as participants in each study had mean scores on the Alzheimer's Disease Assessment Scale (ADAS-cog) of approximately 26 units, with a range from 4 to 61. Experience gained in longitudinal studies of ambulatory patients with mild to moderate Alzheimer's Disease suggest that they gain 6 to 12 units a year on the ADAS-cog. However, lesser degrees of change are seen in patients with very mild or very advanced disease because the ADAS-cog is not uniformly sensitive to change over the course of the disease. The annualized rate of decline in the placebo patients participating in ARICEPT® trials was approximately 2 to 4 units per year.
- The ability of ARICEPT® to produce an overall clinical effect was assessed using a Clinician's Interview Based Impression of Change that required the use of caregiver information, the CIBIC plus. The CIBIC plus is not a single instrument and is not a standardized instrument like the ADAS-cog. Clinical trials for investigational drugs have used a variety of CIBIC formats, each different in terms of depth and structure.
- As such, results from a CIBIC plus reflect clinical experience from the trial or trials in which it was used and cannot be compared directly with the results of CIBIC plus evaluations from other clinical trials. The CIBIC plus used in ARICEPT® trials was a semi-structured instrument that was intended to examine four major areas of patient function: General, Cognitive, Behavioral and Activities of Daily Living. It represents the assessment of a skilled clinician based upon his/her observations at an interview with the patient, in combination with information supplied by a caregiver familiar with the behavior of the patient over the interval rated. The CIBIC plus is scored as a seven point categorical rating, ranging from a score of 1, indicating "markedly improved," to a score of 4, indicating "no change" to a score of 7, indicating "markedly worse." The CIBIC plus has not been systematically compared directly to assessments not using information from caregivers (CIBIC) or other global methods.
- Thirty-Week Study
- In a study of 30 weeks duration, 473 patients were randomized to receive single daily doses of placebo, 5 mg/day or 10 mg/day of ARICEPT®. The 30-week study was divided into a 24-week double-blind active treatment phase followed by a 6-week single-blind placebo washout period. The study was designed to compare 5 mg/day or 10 mg/day fixed doses of ARICEPT® to placebo. However, to reduce the likelihood of cholinergic effects, the 10 mg/day treatment was started following an initial 7-day treatment with 5 mg/day doses.
- Effects on the ADAS-cog
- Figure 1 illustrates the time course for the change from baseline in ADAS-cog scores for all three dose groups over the 30 weeks of the study. After 24 weeks of treatment, the mean differences in the ADAS-cog change scores for ARICEPT® treated patients compared to the patients on placebo were 2.8 and 3.1 units for the 5 mg/day and 10 mg/day treatments, respectively. These differences were statistically significant. While the treatment effect size may appear to be slightly greater for the 10 mg/day treatment, there was no statistically significant difference between the two active treatments.
- Following 6 weeks of placebo washout, scores on the ADAS-cog for both the ARICEPT® treatment groups were indistinguishable from those patients who had received only placebo for 30 weeks. This suggests that the beneficial effects of ARICEPT® abate over 6 weeks following discontinuation of treatment and do not represent a change in the underlying disease. There was no evidence of a rebound effect 6 weeks after abrupt discontinuation of therapy.

This image is provided by the National Library of Medicine.

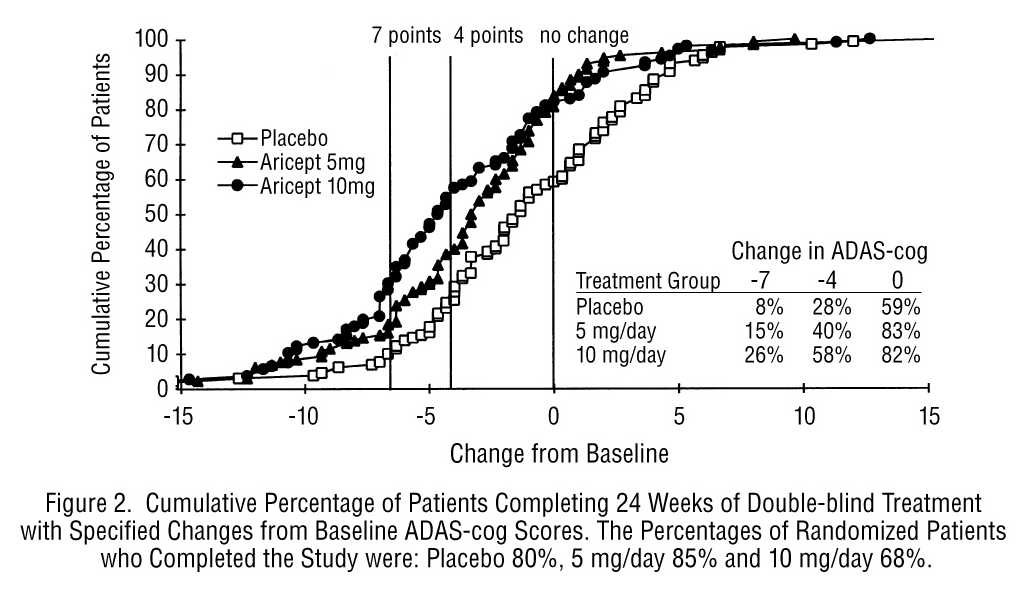
- Figure 2 illustrates the cumulative percentages of patients from each of the three treatment groups who had attained the measure of improvement in ADAS-cog score shown on the X axis. Three change scores, (7-point and 4-point reductions from baseline or no change in score) have been identified for illustrative purposes and the percent of patients in each group achieving that result is shown in the inset table.
- The curves demonstrate that both patients assigned to placebo and ARICEPT® have a wide range of responses, but that the active treatment groups are more likely to show the greater improvements. A curve for an effective treatment would be shifted to the left of the curve for placebo, while an ineffective or deleterious treatment would be superimposed upon or shifted to the right of the curve for placebo, respectively.
This image is provided by the National Library of Medicine.

- Effects on the CIBIC plus
- Figure 3 is a histogram of the frequency distribution of CIBIC plus scores attained by patients assigned to each of the three treatment groups who completed 24 weeks of treatment. The mean drug-placebo differences for these groups of patients were 0.35 units and 0.39 units for 5 mg/day and 10 mg/day of ARICEPT®, respectively. These differences were statistically significant. There was no statistically significant difference between the two active treatments.

This image is provided by the National Library of Medicine.

- Fifteen-Week Study
- In a study of 15 weeks duration, patients were randomized to receive single daily doses of placebo or either 5 mg/day or 10 mg/day of ARICEPT® for 12 weeks, followed by a 3-week placebo washout period. As in the 30-week study, to avoid acute cholinergic effects, the 10 mg/day treatment followed an initial 7-day treatment with 5 mg/day doses.
- Effects on the ADAS-Cog
- Figure 4 illustrates the time course of the change from baseline in ADAS-cog scores for all three dose groups over the 15 weeks of the study.
- After 12 weeks of treatment, the differences in mean ADAS-cog change scores for the ARICEPT® treated patients compared to the patients on placebo were 2.7 and 3.0 units each, for the 5 and 10 mg/day ARICEPT®treatment groups respectively. These differences were statistically significant. The effect size for the 10 mg/day group may appear to be slightly larger than that for 5 mg/day. However, the differences between active treatments were not statistically significant.

This image is provided by the National Library of Medicine.

- Following 3 weeks of placebo washout, scores on the ADAS-cog for both the ARICEPT® treatment groups increased, indicating that discontinuation of ARICEPT® resulted in a loss of its treatment effect. The duration of this placebo washout period was not sufficient to characterize the rate of loss of the treatment effect, but, the 30-week study (see above) demonstrated that treatment effects associated with the use of ARICEPT® abate within 6 weeks of treatment discontinuation.
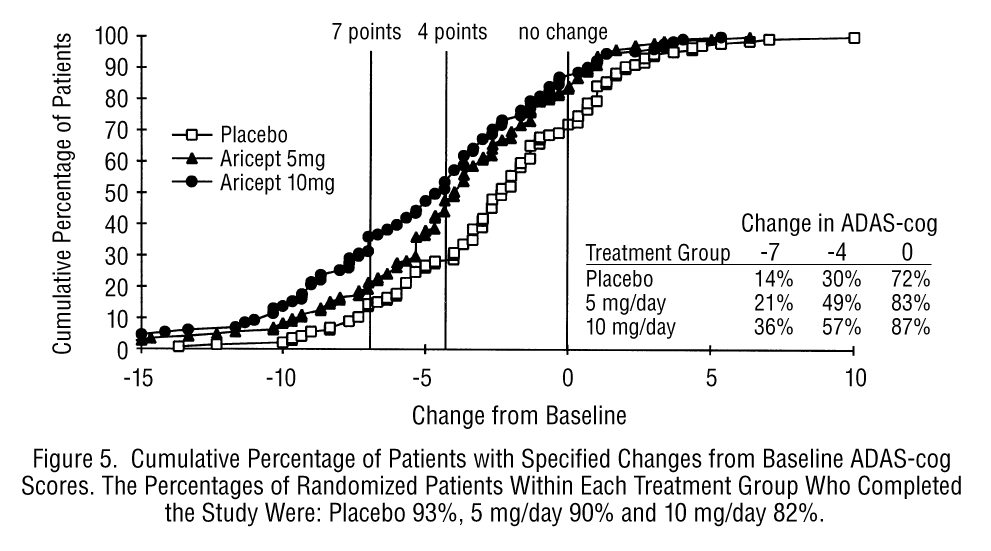
- Figure 5 illustrates the cumulative percentages of patients from each of the three treatment groups who attained the measure of improvement in ADAS-cog score shown on the X axis. The same three change scores, (7-point and 4-point reductions from baseline or no change in score) as selected for the 30-week study have been used for this illustration. The percentages of patients achieving those results are shown in the inset table.
- As observed in the 30-week study, the curves demonstrate that patients assigned to either placebo or to ARICEPT® have a wide range of responses, but that the ARICEPT® treated patients are more likely to show the greater improvements in cognitive performance.
This image is provided by the National Library of Medicine.

- Effects on the CIBIC plus
- Figure 6 is a histogram of the frequency distribution of CIBIC plus scores attained by patients assigned to each of the three treatment groups who completed 12 weeks of treatment. The differences in mean scores for ARICEPT® treated patients compared to the patients on placebo at Week 12 were 0.36 and 0.38 units for the 5 mg/day and 10 mg/day treatment groups, respectively. These differences were statistically significant.

This image is provided by the National Library of Medicine.

- In both studies, patient age, sex and race were not found to predict the clinical outcome of ARICEPT® treatment.
Severe Alzheimer's Disease
- Swedish 24-Week Study
- The effectiveness of ARICEPT® as a treatment for severe Alzheimer's Disease is demonstrated by the results of a randomized, double-blind, placebo-controlled clinical study conducted in Sweden (24-Week Study) in patients with probable or possible Alzheimer's Disease diagnosed by NINCDS-ADRDA and DSM-IV criteria, MMSE: range of 1-10. Two hundred and forty eight (248) patients with severe Alzheimer's disease were randomized to ARICEPT® or placebo. For patients randomized to ARICEPT®, treatment was initiated at 5 mg once daily for 28-days and then increased to 10 mg once daily. At the end of the 24-week treatment period, 90.5% of the ARICEPT® -treated patients were receiving the 10 mg dose. The mean age of patients was 84.9 years with a range of 59 to 99. Approximately 77 % of patients were women and 23 % were men. Almost all patients were Caucasian. Probable AD was diagnosed in the majority of the patients (83.6% of ARICEPT®-treated patients and 84.2% of placebo-treated patients).
- Study Outcome Measures
- The effectiveness of treatment with ARICEPT® was determined using a dual outcome assessment strategy that evaluated cognitive function using an instrument designed for more impaired patients and overall function through caregiver-rated assessment. This study showed that patients on ARICEPT® experienced significant improvement on both measures compared to placebo.
- The ability of ARICEPT® to improve cognitive performance was assessed with the Severe Impairment Battery (SIB). The SIB, a multi-item instrument, has been validated for the evaluation of cognitive function in patients with moderate to severe dementia. The SIB evaluates selective aspects of cognitive performance, including elements of memory, language, orientation, attention, praxis, visuospatial ability, construction, and social interaction. The SIB scoring range is from 0 to 100, with lower scores indicating greater cognitive impairment.
- Daily function was assessed using the Modified Alzheimer's Disease Cooperative Study Activities of Daily Living Inventory for Severe Alzheimer's Disease (ADCS-ADL-severe). The ADCS-ADL-severe is derived from the Alzheimer's Disease Cooperative Study Activities of Daily Living Inventory, which is a comprehensive battery of ADL questions used to measure the functional capabilities of patients. Each ADL item is rated from the highest level of independent performance to complete loss. The ADCS-ADL-severe is a subset of 19 items, including ratings of the patient's ability to eat, dress, bathe, use the telephone, get around (or travel), and perform other activities of daily living; it has been validated for the assessment of patients with moderate to severe dementia. The ADCS-ADL-severe has a scoring range of 0 to 54 with the lower scores indicating greater functional impairment. The investigator performs the inventory by interviewing a caregiver, in this study a nurse staff member, familiar with the functioning of the patient.
- Effects on the SIB
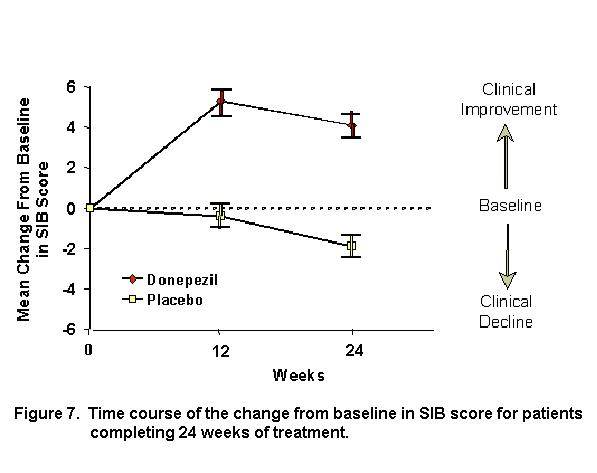
- Figure 7 shows the time course for the change from baseline in SIB score for the two treatment groups over the 24 weeks of the study. At 24 weeks of treatment, the mean difference in the SIB change scores for ARICEPT® -treated patients compared to patients on placebo was 5.9 units. ARICEPT® treatment was statistically significantly superior to placebo.
This image is provided by the National Library of Medicine.

- Figure 8 illustrates the cumulative percentages of patients from each of the two treatment groups who attained the measure of improvement in SIB score shown on the X-axis. While patients assigned both to ARICEPT® and to placebo have a wide range of responses, the curves show that the ARICEPT® group is more likely to show a greater improvement in cognitive performance.
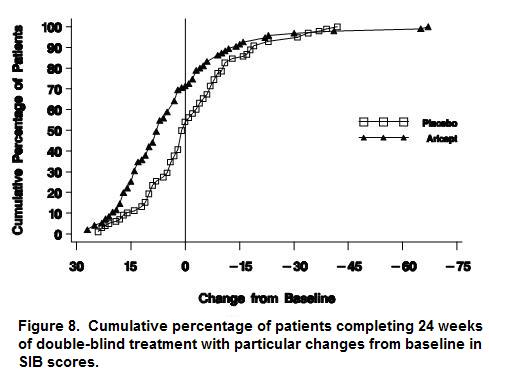
This image is provided by the National Library of Medicine.

This image is provided by the National Library of Medicine.

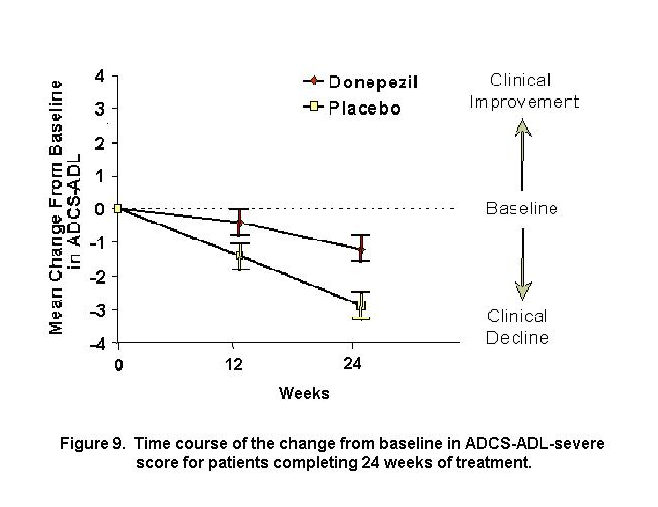
- Effects on the ADCS-ADL-severe
- Figure 9 illustrates the time course for the change from baseline in ADCS-ADL-severe scores for patients in the two treatment groups over the 24 weeks of the study. After 24 weeks of treatment, the mean difference in the ADCS-ADL-severe change scores for ARICEPT® treated patients compared to patients on placebo was 1.8 units. ARICEPT® treatment was statistically significantly superior to placebo.
- Figure 10 shows the cumulative percentages of patients from each treatment group with specified changes from baseline ADCS-ADL-severe scores. While both patients assigned to ARICEPT®and placebo have a wide range of responses, the curves demonstrate that the ARICEPT®group is more likely to show a smaller decline or an improvement.
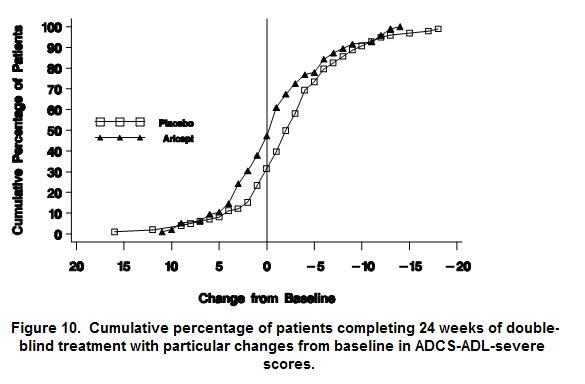
This image is provided by the National Library of Medicine.

- Japanese 24-Week Study
- In a study of 24 weeks duration, conducted in Japan, 325 patients with severe Alzheimer's Disease were randomized to doses of 5 mg/day or 10 mg/day of donepezil, administered once daily, or placebo. Patients randomized to treatment with donepezil were to achieve their assigned doses by titration, beginning at 3 mg/day, and extending over a maximum of 6 weeks. 248 patients completed the study with similar proportions of patients completing the study in each treatment group. The primary efficacy measures for this study were the SIB and CIBIC plus.
- At 24 weeks of treatment, statistically significant treatment differences were observed between the 10 mg/day dose of donepezil and placebo on both the SIB and CIBIC plus. The 5 mg/day dose of donepezil showed a statistically significant superiority to placebo on the SIB, but not on the CIBIC plus.
How Supplied
- ARICEPT® Oral Solution is a clear, colorless to light yellow solution containing 1 mg of donepezil hydrochloride in each mL (1 mg/mL). Each teaspoon (5mL) contains 5 mg of donepezil hydrochloride.
- NDC# 62856-851-30 300 mL HDPE Bottles
- Storage: Store at controlled room temperature, 15°C to 30°C (59°F to 86°F).
Storage
There is limited information regarding Donepezil Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Donepezil |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Donepezil |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Donepezil in the drug label.
Precautions with Alcohol
- Alcohol-Donepezil interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- Aricept®[1]
Look-Alike Drug Names
- Aricept® — Aciphex®[2]
- Aricept® — Azilect®[2]
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ "aricept (donepezil hydrochloride) solution [Eisai Inc.]".
- ↑ 2.0 2.1 "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Donepezil |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Donepezil |Label Name=Donepezil05.png
}}