Congenital heart defect
| Congenital heart defect | |
 | |
|---|---|
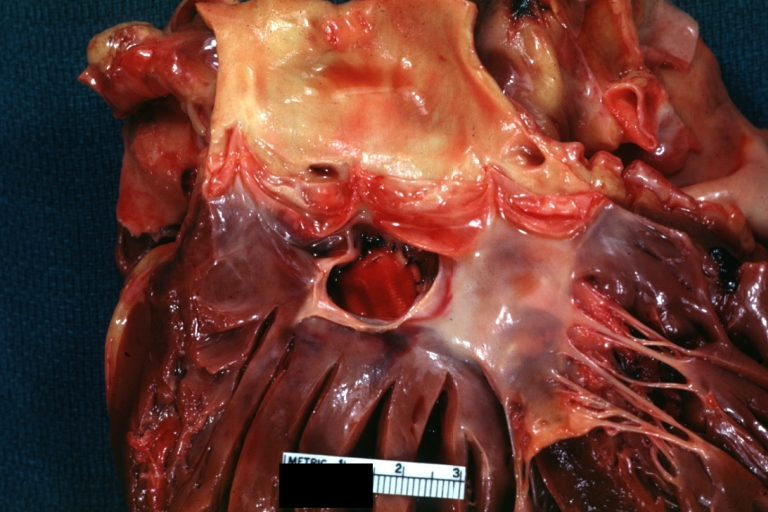
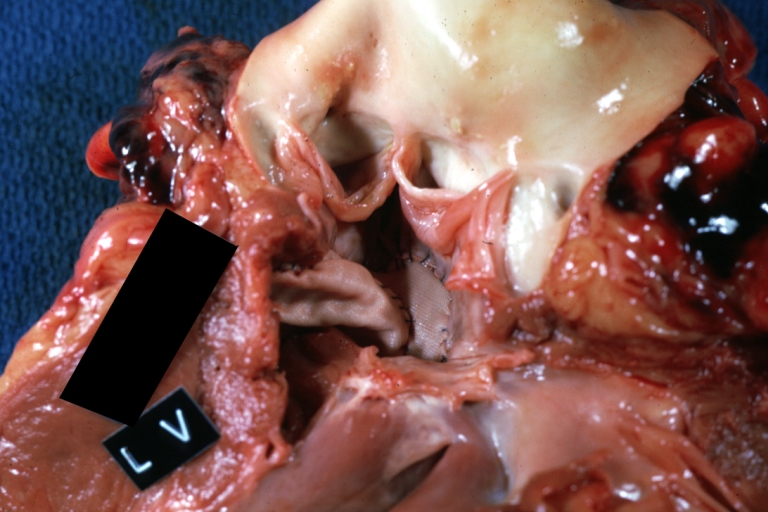
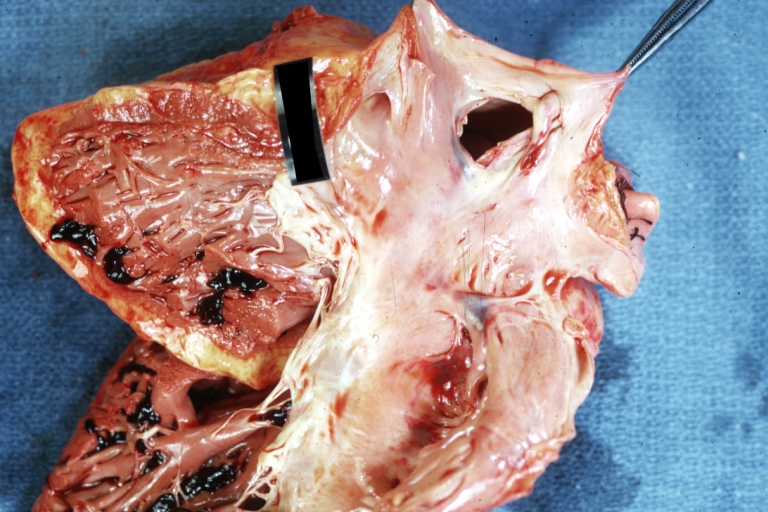
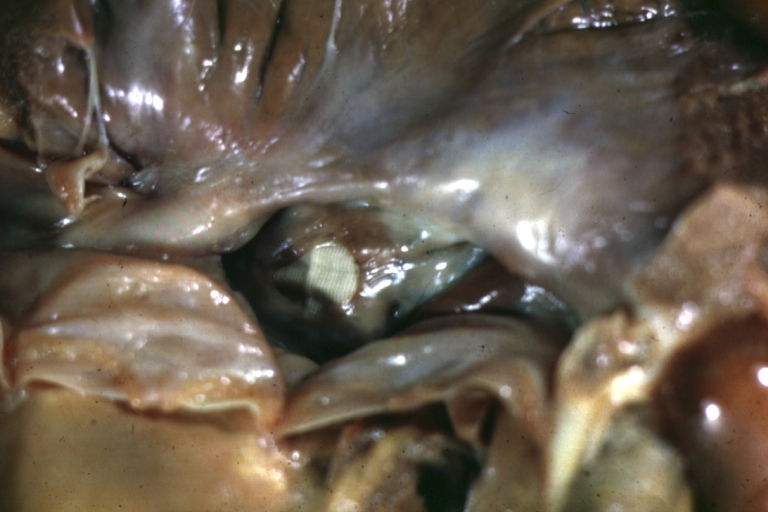
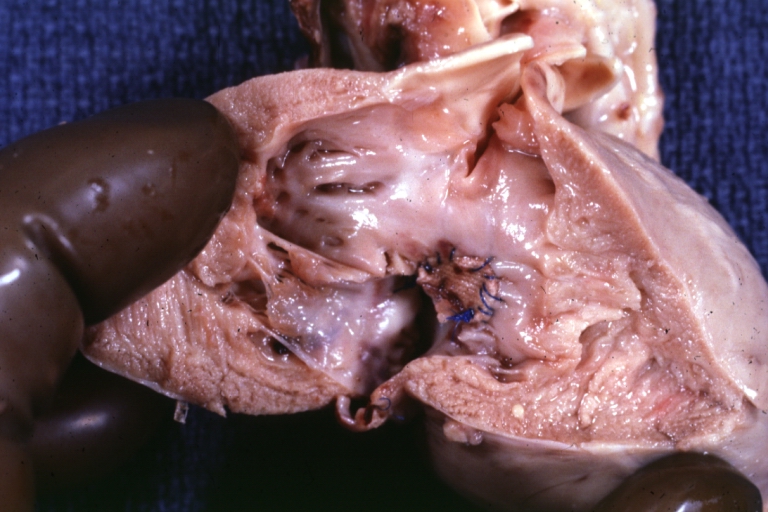
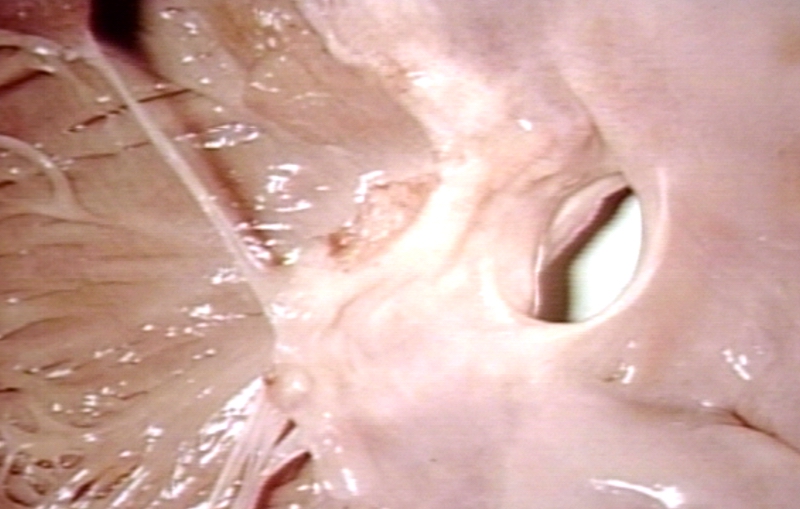
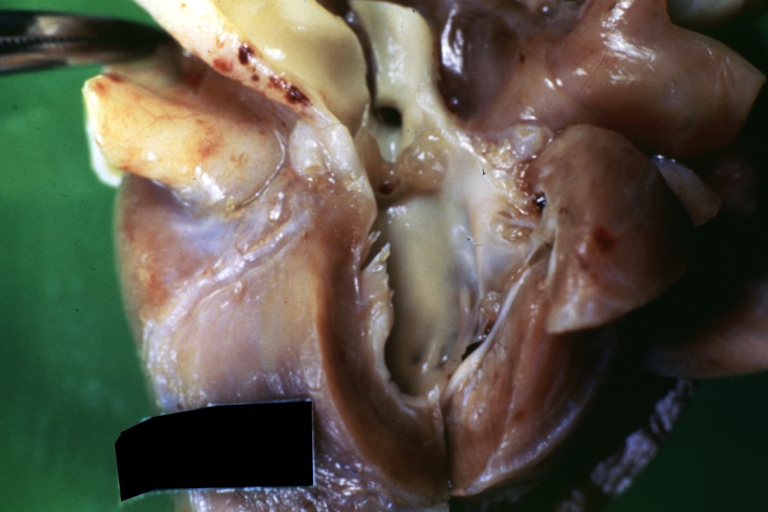
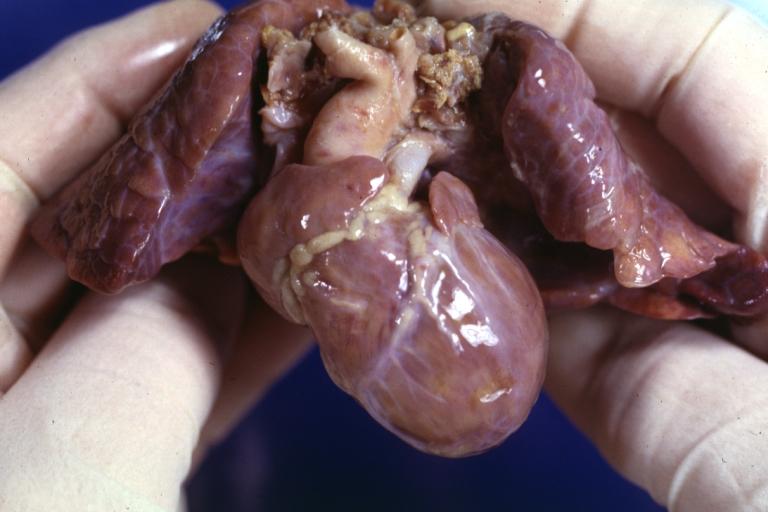
| Subvalvular Ventricular Septal Defect: Gross, good view of defect with overriding aorta. Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology | |
| ICD-10 | Q20-Q26 |
| ICD-9 | 745-747 |
| DiseasesDB | 17017 |
| MeSH | D006330 |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-in-Chief: Keri Shafer, M.D. [2]
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
A congenital heart defect (CHD) is a defect in the structure of the heart and great vessels of a newborn. Most heart defects either obstruct blood flow in the heart or vessels near it or cause blood to flow through the heart in an abnormal pattern, although other defects affecting heart rhythm (such as long QT syndrome) can also occur. Heart defects are among the most common birth defects and are the leading cause of birth defect-related deaths.
Congenital heart defects can be broadly categorized into two groups, acyanotic heart defects ("pink" babies) and cyanotic heart defects ("blue" babies).
Epidemiology
( Affecting approximately one in every 125 babies born, congenital heart defects are the most common birth defect (March of Dimes)[4]. Forty thousand people are born each year with a CHD; 4,000 will not survive their first year(The Children's Heart Foundation). Twice as many children die each year from a CHD than all forms of Pediatric Cancers combined (The Children's Heart Foundation). The eight most common defects account for 80% of all congenital heart diseases, while the remaining 20% consist of many independently infrequent conditions or combinations of several defects. Ventricular septal defect (VSD) is generally considered to be the most common type of malformation, accounting for about 1/3 of all congenital heart defects.
The incidence is higher when a parent or a sibling has a heart defect (4–5%), in stillborns (3–4%), abortuses (10–25%), and premature infants (2%).
The number of adults with problems connected to a congenital heart defect is rising, passing the number of children with congenital heart defects in most Western countries. This group is referred to as grown-up congenital heart disease (GUCH) patients.
Twice as many children die from a CHD than from all forms of pediatric cancers combined.
Etiology
The cause of most congenital heart defects is unknown.
Where a cause is known, it may be of a multifactorial origin and/or a result of genetic predisposition and environmental factors.
Known genetic causes of heart disease includes chromosomal abnormalities such as trisomies 21, 13, and 18, as well as a range of newly recognised genetic point mutations, point deletions and other genetic abnormalities as seen in syndromes such as CATCH 22, familial ASD with heart block, Alagille syndrome, Noonan syndrome, and many more.
Known antenatal environmental factors include maternal infections (Rubella), drugs (alcohol, hydantoin, lithium and thalidomide) and maternal illness (diabetes mellitus, phenylketonuria, and systemic lupus erythematosus).
Relation of congenital heart defects with sex
According to "Teratological rule of sexual dimorphism" (V. Geodakian, 1970), inborn anomalies that have atavistic nature appear more frequently among females, and futuristic anomalies appear among males. This rule was applied to explain differences in sex ratio observed for congenital heart defects.[1][2]
In the 32,000 diagnoses of "female" malformations, those relating to the heart of the embryo and to the phylogenetic human predecessors predominated (Table). The most well-defined female's defects are patent ductus arteriosus (1♂ : 2.72♀), Lutembacher disease (1♂ : 2.1♀), and ostium secundum (1♂ : 1.84♀).
Sex ratio of patients with congenital heart defects Congenital heart defect Sex ratio, males:females Patent ductus arteriosus 1 : 2.72 Lutembaher disease 1 : 2.14 Ostium secundum 1 : 1.84 Ventricular septal defect and patent ductus arteriosus 1 : 1.51 Fallot's triad 1 : 1.45 Eisenmenger's complex 1 : 1.40 Partial atrioventricular canal 1 : 1.36 Ostium primum 1 : 1.20 Partial anomalous pulmonary venous connection 1 : 1.19 Ventricular septal defect 1 : 1.02 Potts and Waterston-Cooley shunts 1 : 1.01 Atrioventricular canal 1 : 1.01 Ebstein's anomaly 1.02 : 1 Stenosis of lung artery 1.04 : 1 Tricuspid atresia 1.16 : 1 Truncus arteriosus 1.21 : 1 Tetralogy of Fallot 1.35 : 1 Coarctation of aorta and an open arterial channel 1.37 : 1 Total anomalous pulmonary venous connection 1.39 : 1 Transposition of the great arteries 1.90 : 1 Coarctation of the aorta 2.14 : 1 Aortic stenosis 2.66 : 1
Most well-defined "male" congenital heart defects are: aortic stenosis (2.66♂ : 1♀), coarctation of the aorta (2.14♂ : 1♀), transpositions of the great arteries (1.90♂ : 1♀), a total anomalous pulmonary venous connection (1.39♂ : 1♀), and coarctation of aorta with an open arterial channel (1.37♂ : 1♀). None of the male's components of congenital heart defects have a corresponding similar formation at normal embryo or at phylogenetic predecessors of the humans. They can be considered as unsuccessful tests of the evolution process.
Other congenital heart defects are of a neutral type. The frequency of occurrence is about the same for both sexes. Among them it is also possible to allocate simple (Potts/Waterston-Cooley shunt and ostium primum) and complex (partial and full atrioventricular canal, Ebstain's anomaly and tricuspid atresia) defects. Simple defects of this group, as well as female defects, can be considered atavistic. The difference between them is that these defects, contrary to female ones, represent a return to the far past in the onthogenetic and phylogenetic sense. They can be considered as a consequence of a block in heart development at early stages of embriogenesis (the first 2-3 months of the embryo's life during which the anatomic formation of the heart occurs), and at earlier (in comparison to female defects) stages of phylogenesis. For complex defects of the neutral group, the sex ratio depends on which of their components prevail—female or male.
Rokitansky (1875) explained congenital heart defects as breaks in heart development at various ontogenesis stages.[3] Spitzer (1923) treats them as returns to one of the phylogenesis stages.[4] Krimsky (1963), synthesizing two previous points of view, considered congenital heart diseases as a stop of development at a certain stage of ontogenesis, corresponding to this or that stage of the phylogenesis.[5] Hence these theories can explain atavistic heart diseases only (feminine and neutral, according to our classification), and no explanation has been found for masculine defects.
The concept allows considering sex of the patient as a diagnostic symptom. This symptom is stable and cheap and does not harm the patient compared to some invasive diagnostic procedures.
Major categories
Patent ductus arteriosus
The ductus arteriosus is a temporary pathway in the foetal heart between the pulmonary artery and aorta, which allows blood to bypass the fetus's nonfunctioning lungs until birth. Normally, the ductus closes within a few hours or days of birth; when it does not, the result is patent ductus arteriosus. This defect is common in premature infants but rare in full-term infants.
Hypoplasia
Hypoplasia can affect the heart, which typically results in the failure of either the right ventricle or the left ventricle to develop adequately, leaving only one side of the heart capable of pumping blood to the body and lungs. Hypoplasia of the heart is rare but is the most serious form of CHD; it is called hypoplastic left heart syndrome when it affects the left side of the heart and hypoplastic right heart syndrome when it affects the right side of the heart. In both conditions, the presence of a patent ductus arteriosus (and, when hypoplasia affects the right side of the heart, a patent foramen ovale) is vital to the infant's ability to survive until emergency heart surgery can be performed, since without these pathways blood cannot circulate to the body (or lungs, depending on which side of the heart is defective). Hypoplasia of the heart is generally a cyanotic heart defect.
Obstruction defects
Obstruction defects occur when heart valves, arteries, or veins are abnormally narrow or blocked. Common obstruction defects include pulmonary valve stenosis, aortic valve stenosis, and coarctation of the aorta, with other types such as bicuspid aortic valve stenosis and subaortic stenosis being comparatively rare. Any narrowing or blockage can cause heart enlargement or hypertension.
Septal defects
The septum is a wall of tissue which separates the left heart from the right heart. It is comparatively common for defects to exist in the interatrial septum or the interventricular septum, allowing blood to flow from the left side of the heart to the right, reducing the heart's efficiency. Ventricular septal defects are collectively the most common type of CHD, although approximately 30% of adults have a type of atrial septal defect called patent foramen ovale. Septal defects may or may not cause cyanosis depending on the severity of the defect.
Cyanotic defects
Cyanotic heart defects are called such because they result in cyanosis, a bluish-grey discoloration of the skin due to a lack of oxygen in the body. Such defects include persistent truncus arteriosus, total anomalous pulmonary venous connection, tetralogy of Fallot, transposition of the great vessels, and tricuspid atresia.
Other defects
Signs and Symptoms
Symptoms and signs are related to the type and severity of the heart defect. Some children have no signs while others may exhibit shortness of breath, cyanosis, chest pain, syncope, sweating, heart murmur, respiratory infections, underdeveloping of limbs and muscles, poor feeding, or poor growth. Most defects cause a whispering sound, or murmur, as blood moves through the heart causing some of these symptoms. All of these symptoms occur at a young age of a child or infant and are typically found during a physical examination.
Treatment
Sometimes CHD improves with no treatment necessary. At other times the defect is so small and does not require any treatment. Most of the time CHD is serious and requires surgery and/or medications. Medications include diuretics, which aid the baby in eliminating water, salts, and digoxin and in strengthening the contraction of the heart. This slows the heartbeat and removes some fluid from tissues. Some defects require surgical procedures to repair as much as possible to restore circulation back to normal. In some cases, multiple surgeries are needed to be performed to help balance the circulation. Interventional cardiology now offers patients minimally invasive alternatives to surgery. Device closures can now be treated with a standard transcatheter procedure using a closure device mounted on a balloon catheter.
Pathological Findings
-
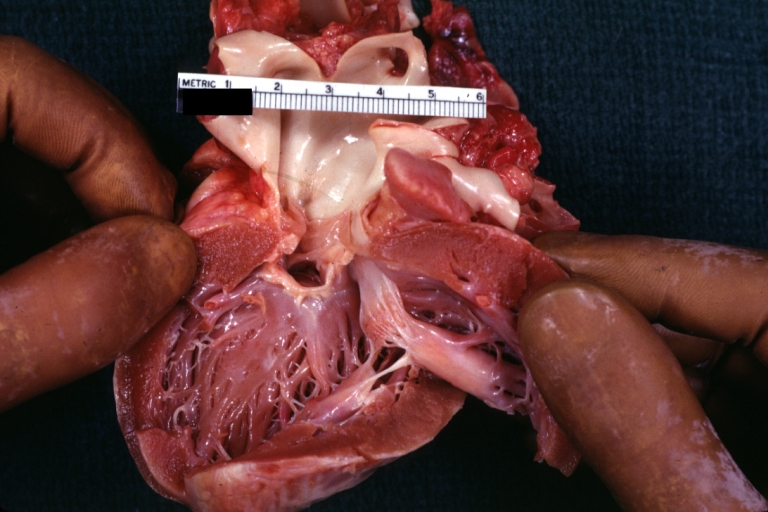
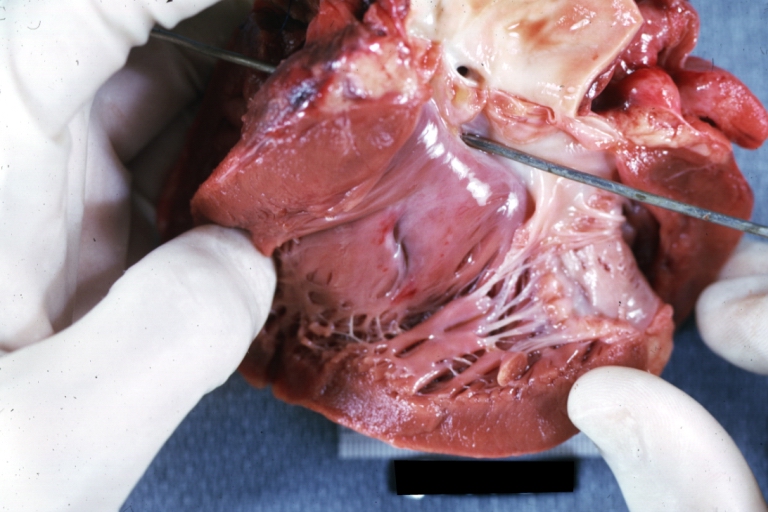
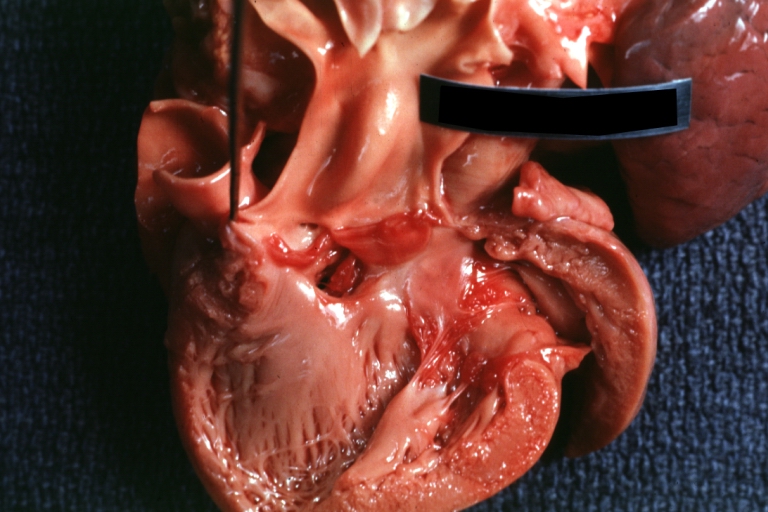
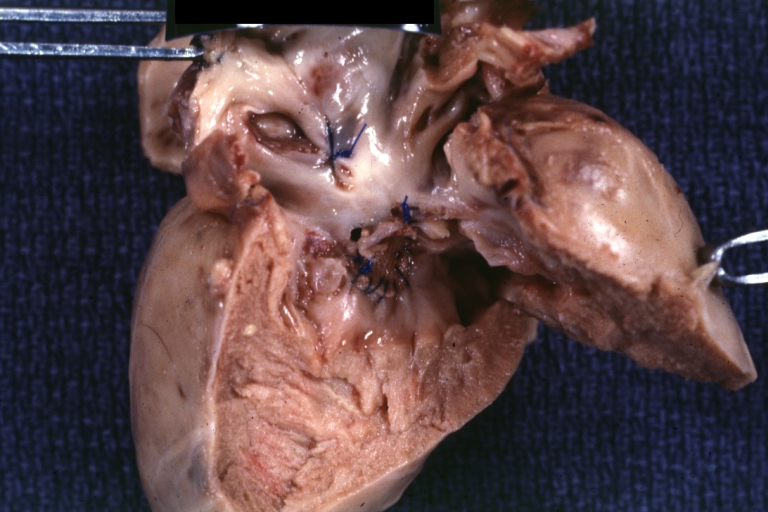
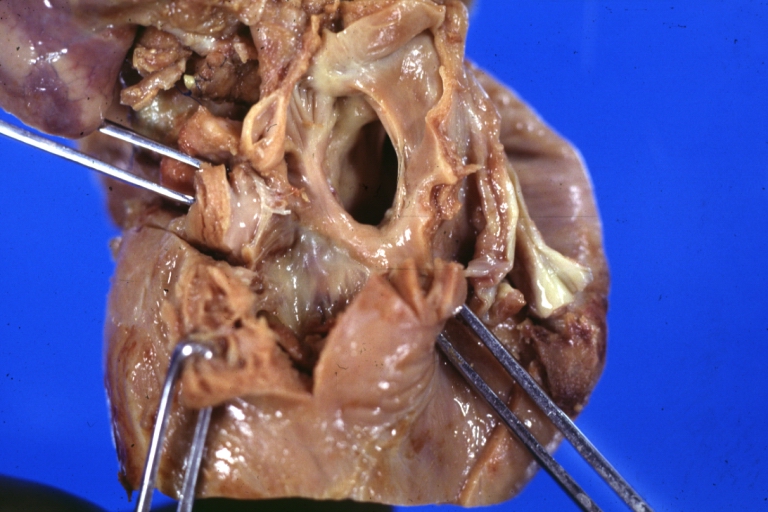
Tetralogy of Fallot: Gross, a good example of repaired perimembranous septal defect
-

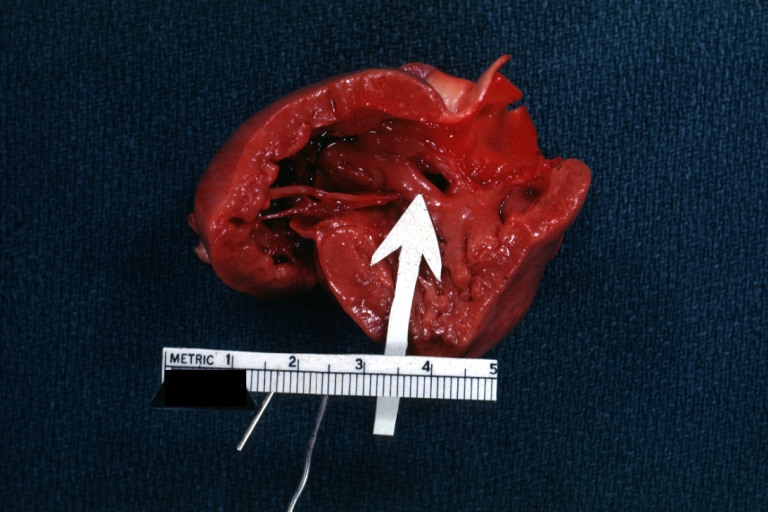
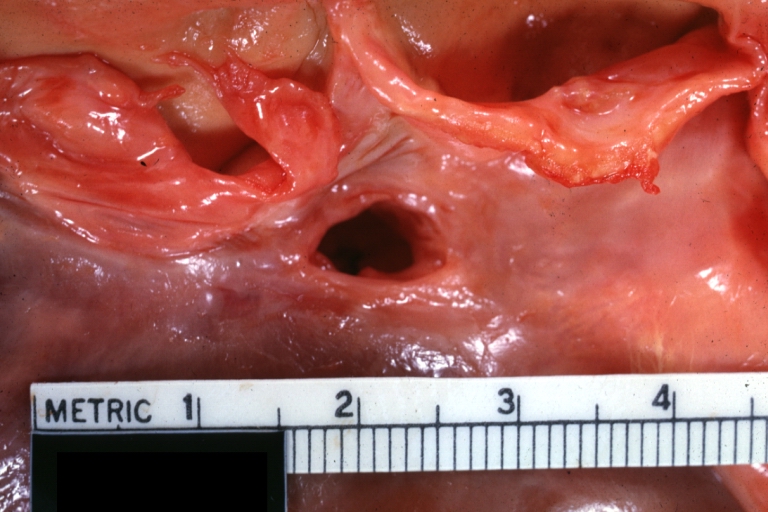
Interventricular Septal Defect (Muscular Septum): Gross, natural color, muscular septal defect in newborn
-
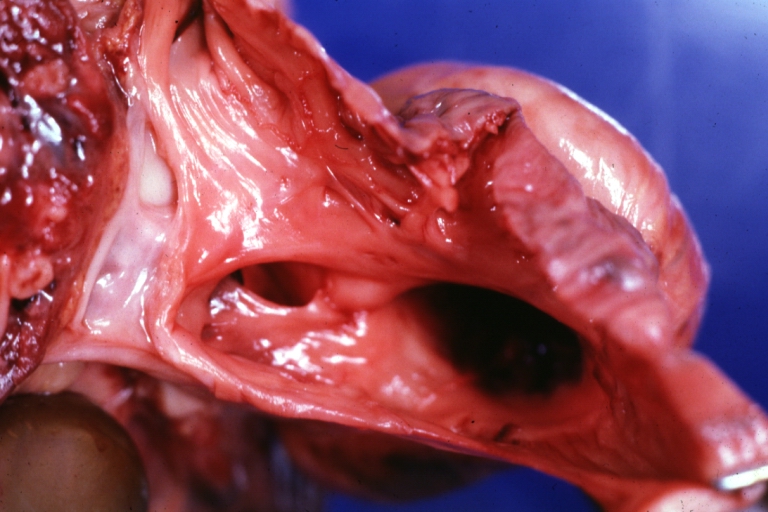
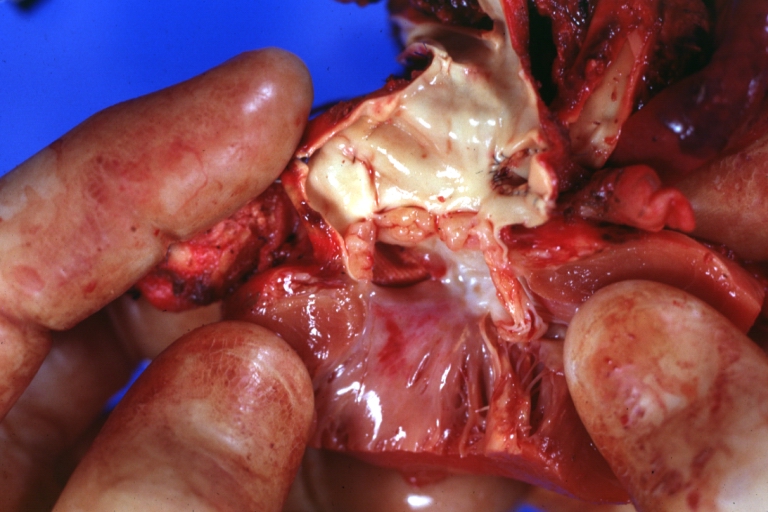
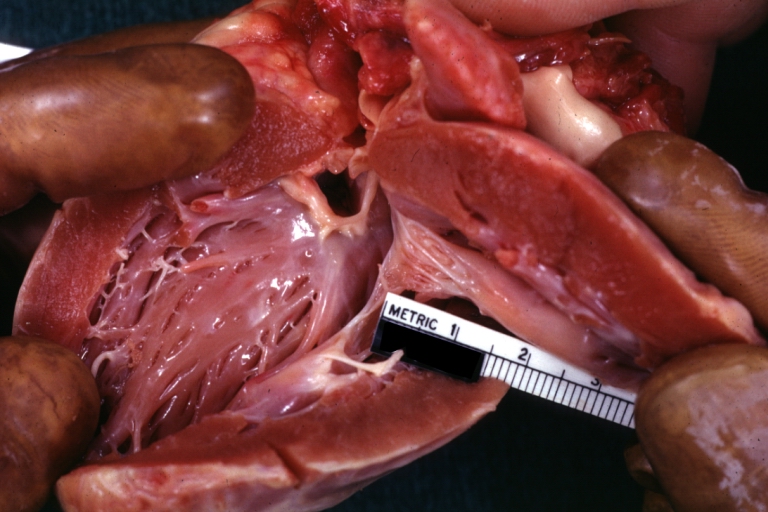
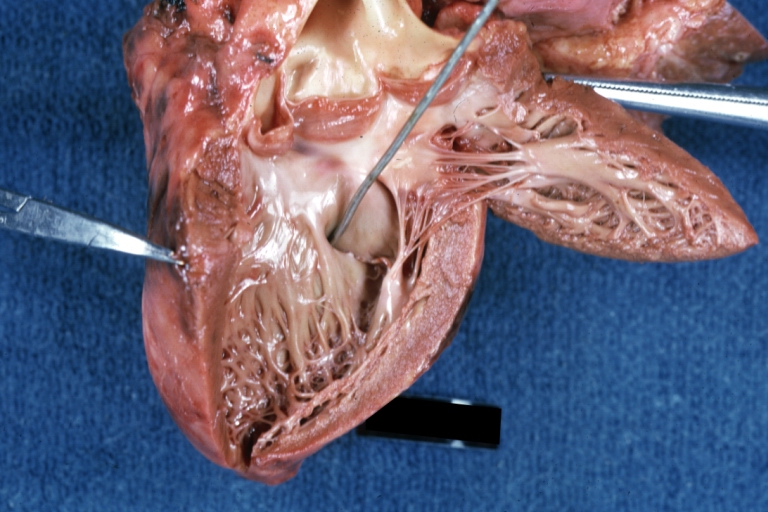
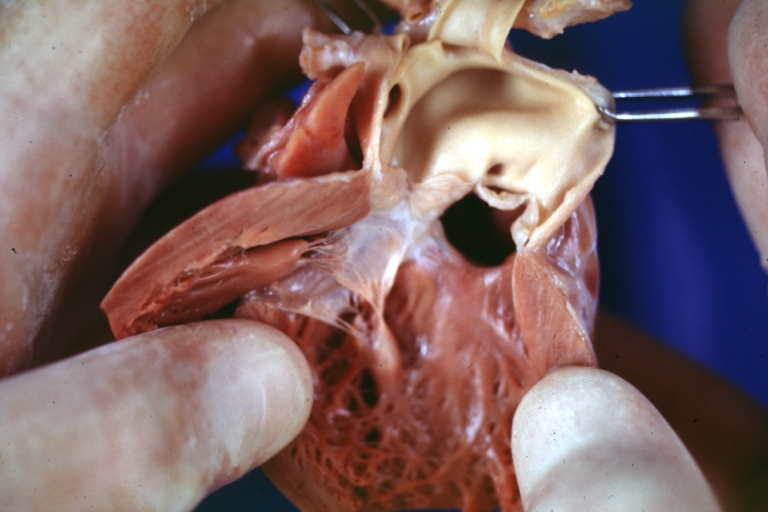
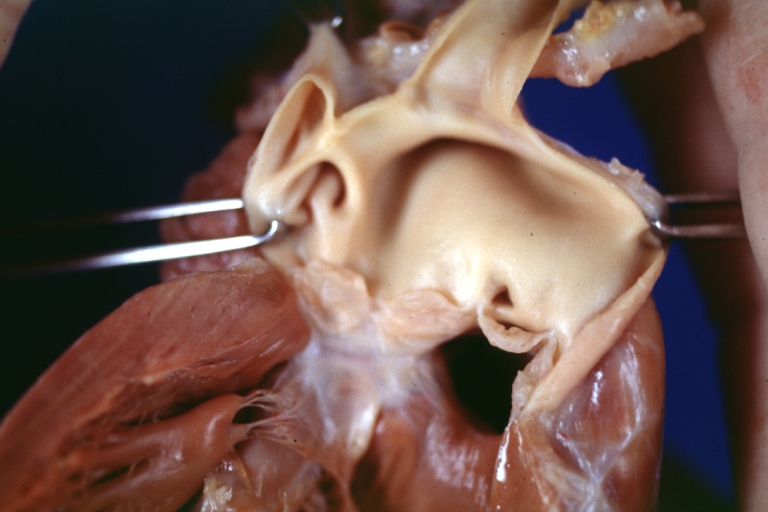
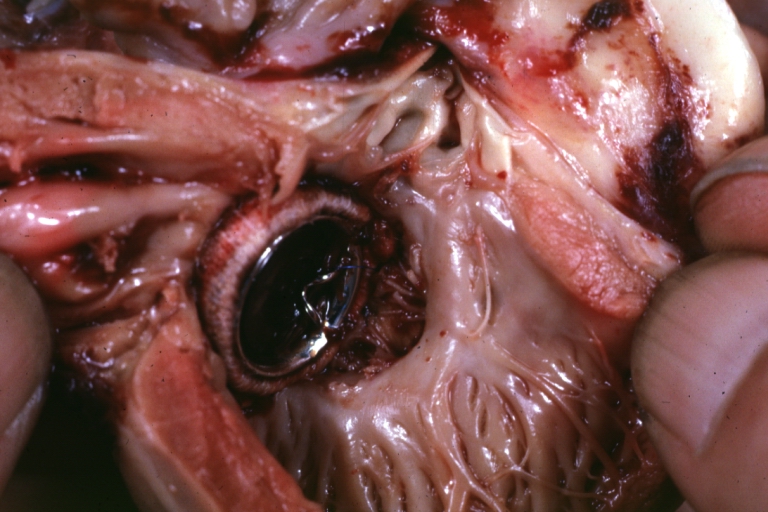
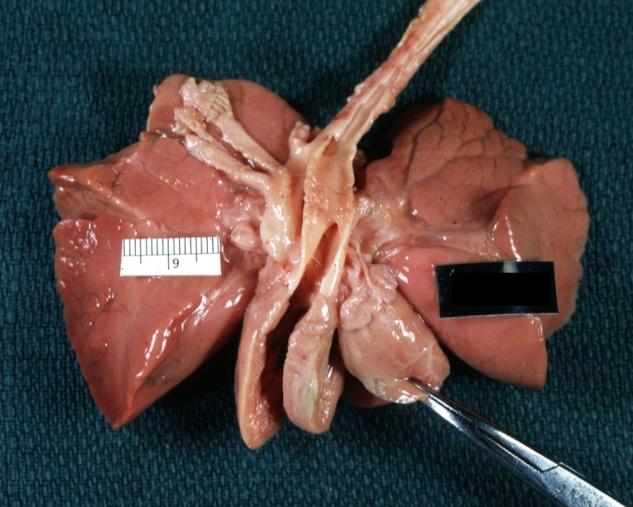
Subvalvular Ventricular Septal Defect: Gross, good view of defect with overriding aorta


-
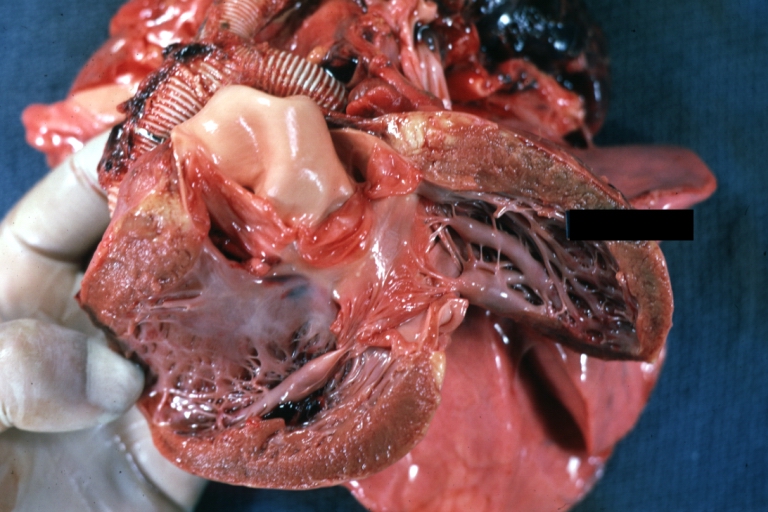
Ventricular Septal Defect: Gross, infant heart, pulmonary outlet, muscular septal defect
-

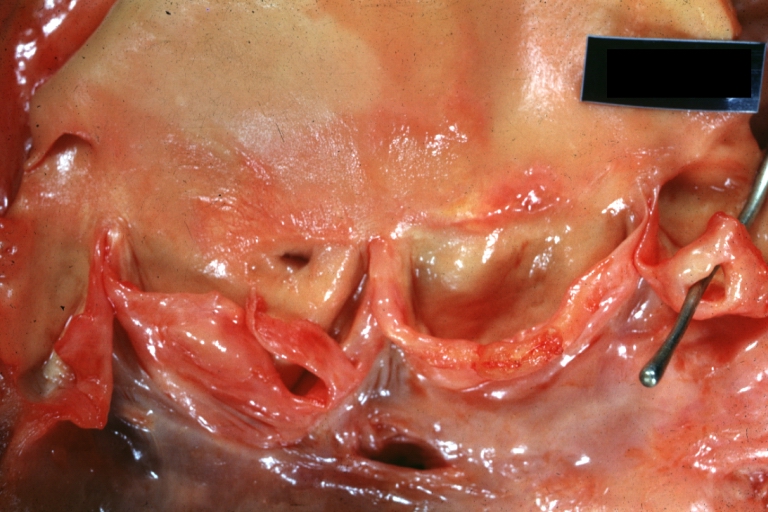
Atrioventricular Canal: Gross, right ventricular view of canal defect
-

Atrioventricular Canal: Gross, left ventricle view of canal defect (very good example)



-

Perimembranous Ventricular Septal Defect: Gross, an excellent example
-
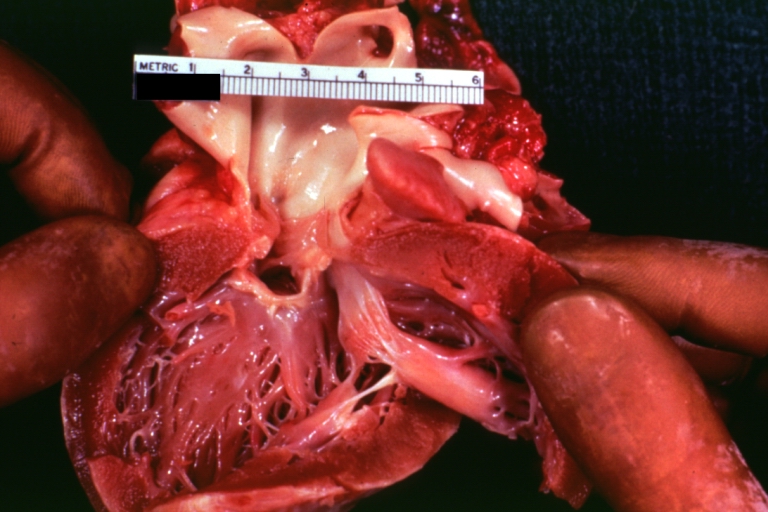
Ventricular Septal Defect: Gross, subvalvular defect, left ventricle view of tetralogy of Fallot (very good example)
-
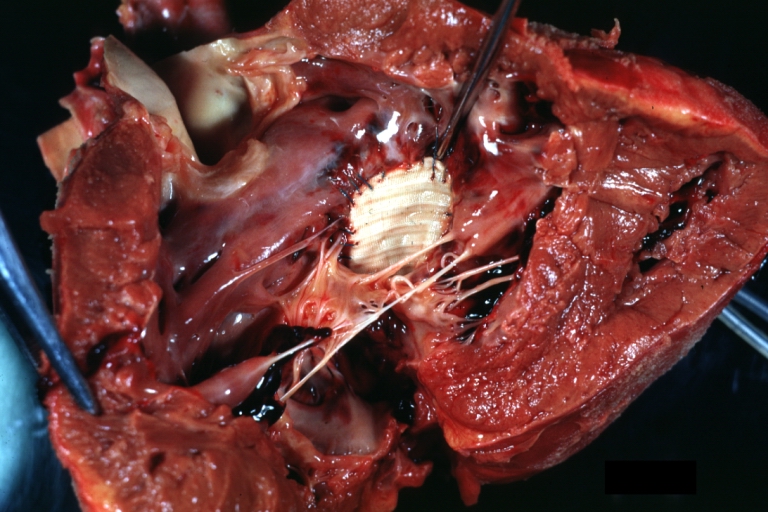
Tetralogy of Fallot: Gross, close-up of aortic valve with subvalvular septal defect with Dacron patch (very good example)



-
Subpulmonic Ventricular Septal Defect: Gross, a well shown lesion.
-
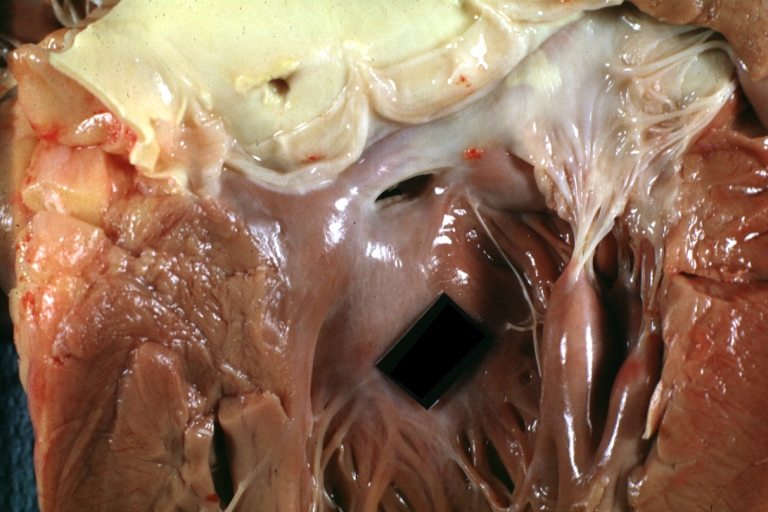
Subvalvular Ventricular Septal Defect
-
Subvalvular Ventricular Septal Defect



-

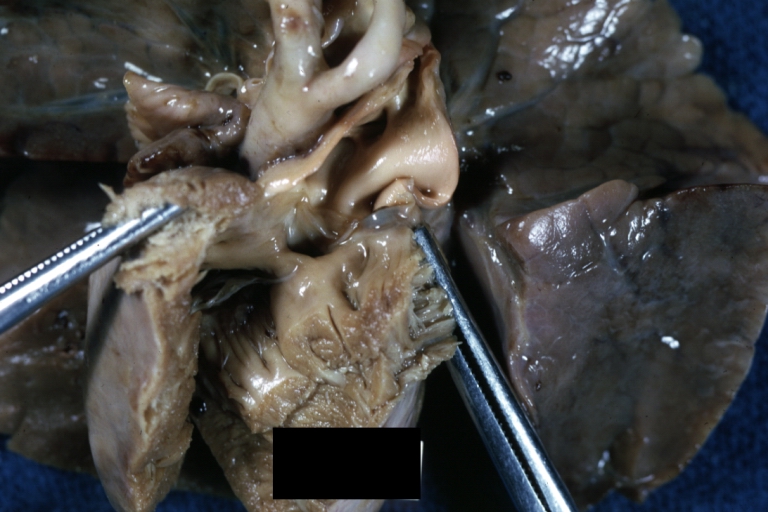
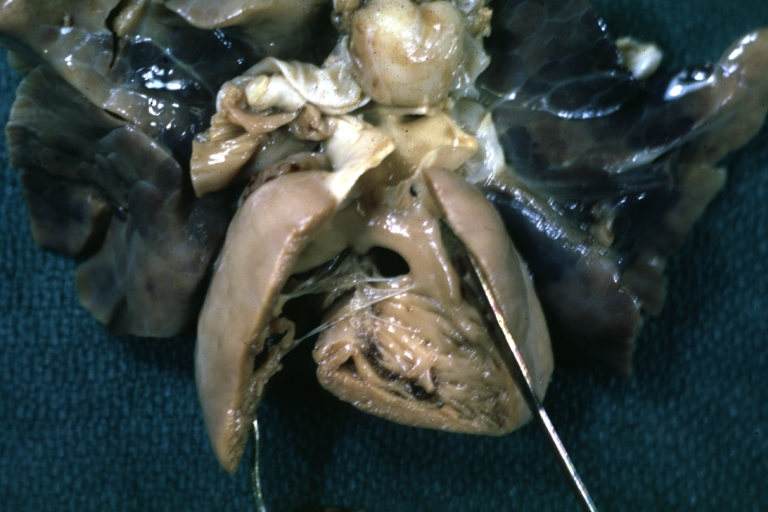
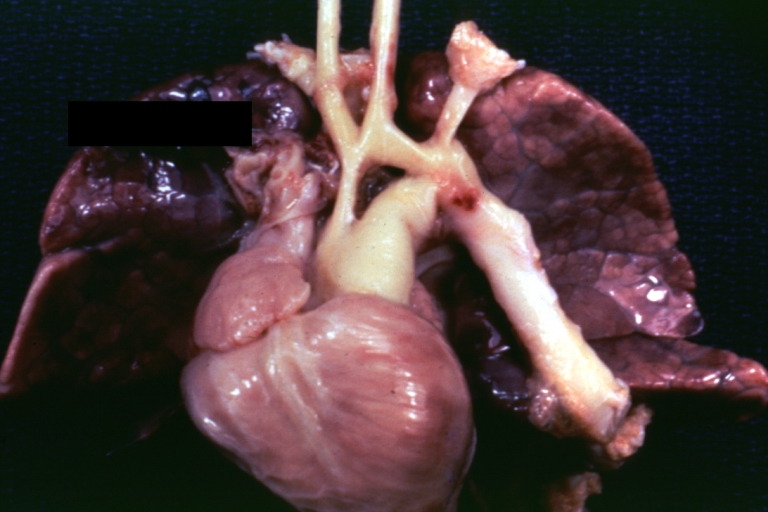
Ventricular Septal Defect: Gross, natural color, view of opened heart with lungs attached shows rather well a subvalvular VSD
-

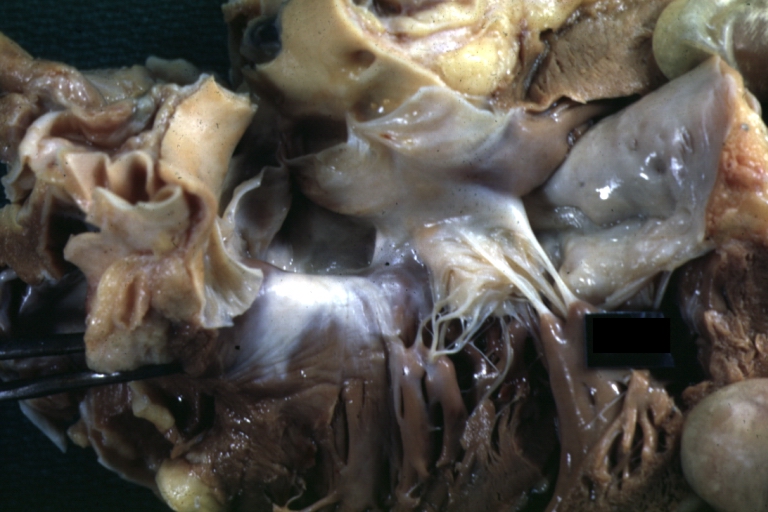
Atrioventricular Canal: Gross, patch repair of defect seen from left side showing left atrial portion extending into a cleft mitral valve
-

Atrioventricular Canal: Gross, corrected defect with patch viewed from left side atrium and cleft mitral valve



-
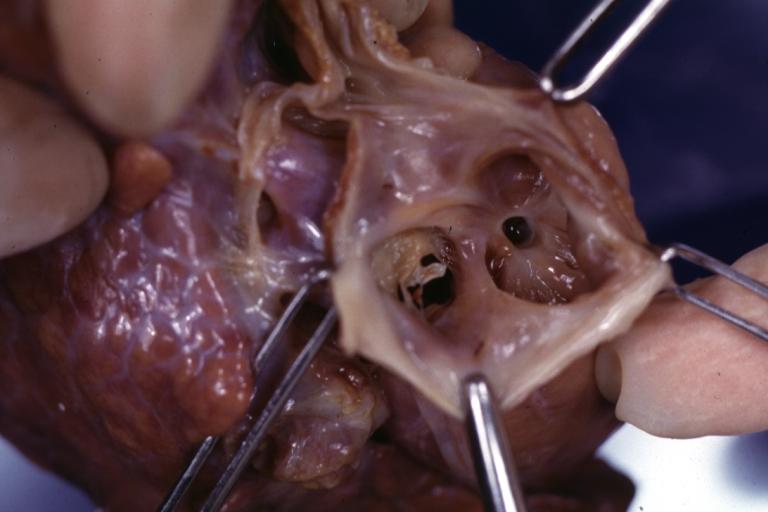
Atrial Septal Defect: Gross, (an excellent example) foramen ovale defect with right ventricular hypertrophy and fatty infiltration of the right ventricular wall, enlarged right atrium
-
Ventricular Septal Defect: Gross close-up adult heart, small perimembranous septal defect (very good example)
-
Interventricular Septal Defect (Muscular Septum): Gross, natural color, low septal defect shown from aortic outlet. The same defect (with a probe in hole) shown from right ventricle.



-
Interventricular Septal Defect (Muscular Septum): Gross natural color right ventricular outlet (probe in defect) view from left ventricular side
-
Atrial Septal Defect: Gross natural color infant heart foramen ovale defect, septum secundum
-
Aortic Subvalvular Ventricular Septal Defect: Gross, natural color, septal defect has patch repair. Aortic valve is myxomatous. A complex case of truncus with interrupted arch.



-
Interventricular Septal Defect Membranous Septum: Gross natural color close-up (an excellent demonstration)
-
Interventricular Septal Defect Membranous Septum: Gross natural color small defect well shown. Aortic cusps are scarred and one is perforated
-
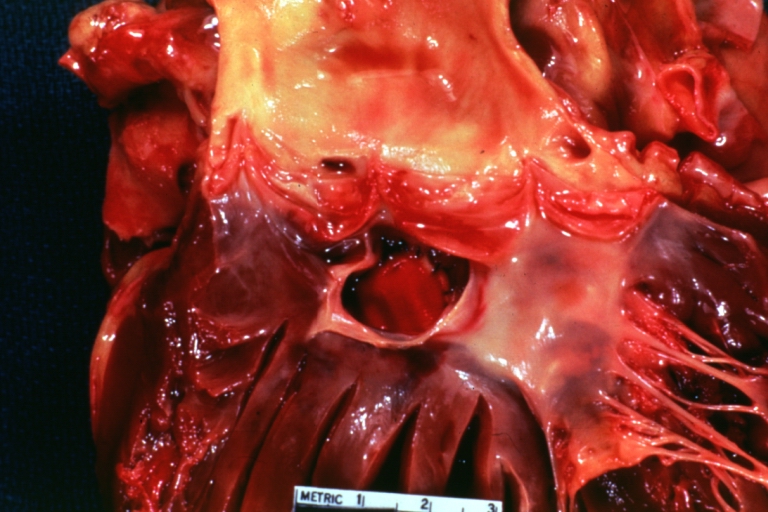
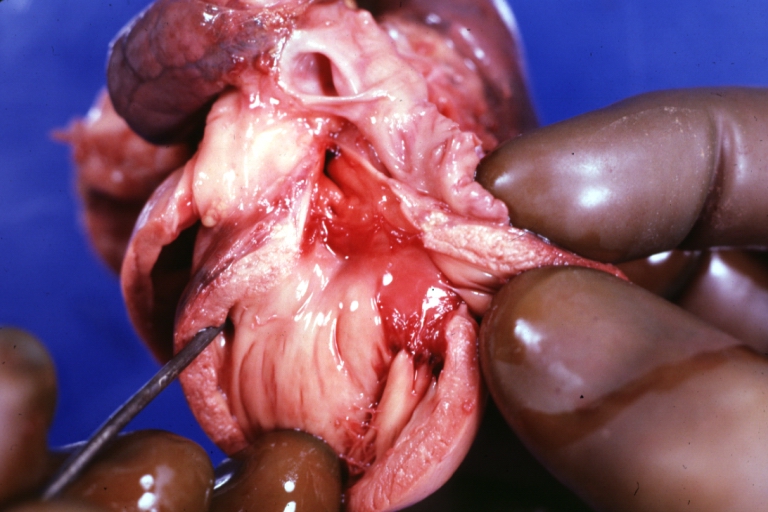
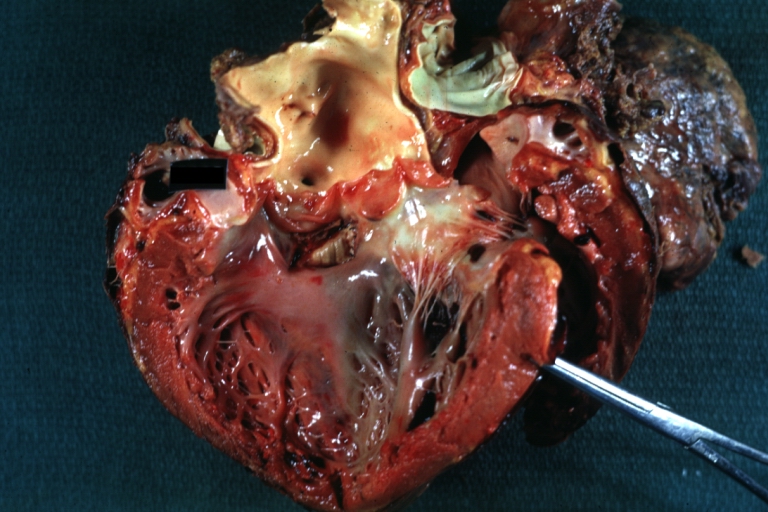
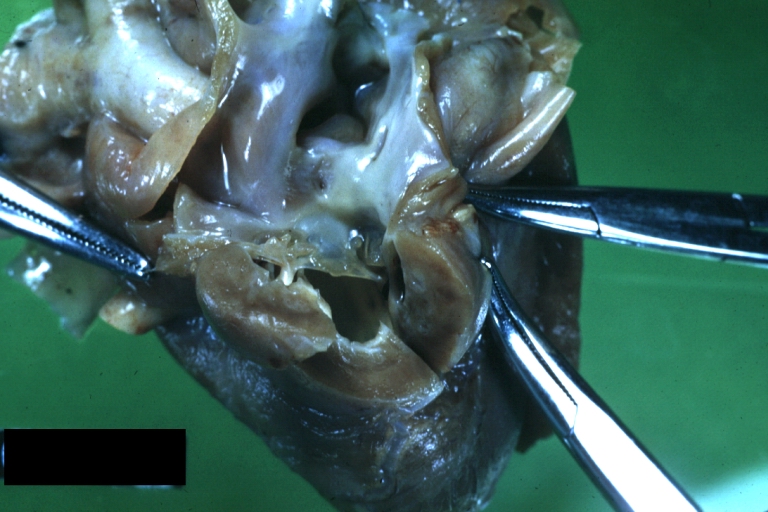
Subvalvular Ventricular Septal Defect: Gross, natural color, close-up view of aortic outflow tract with a large subvalvular defect



-
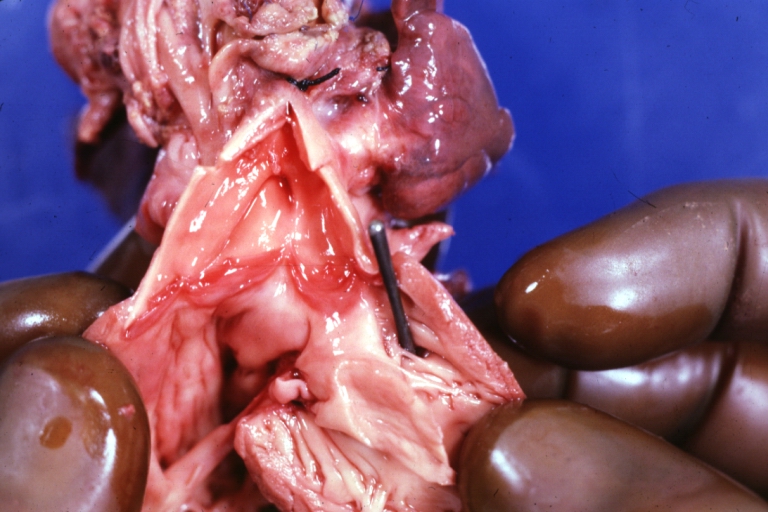
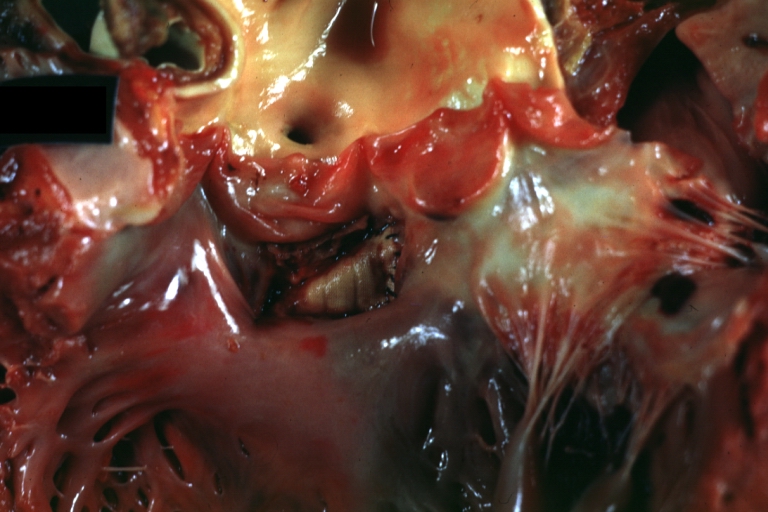
Membranous Interventricular Septal Defect: Gross natural color subvalvular defect with probe immediately inferior to membranous septum
-
Subvalvular Ventricular Septal Defect: Gross, fixed tissue, large subpulmonic defect apparently represent left displacement of the pulmonary artery
-
Interventricular Septal Defect: Gross, fixed tissue, opened right ventricular outflow tract positioned to show perimembranous septal defect (as surgeon would see it during repair)



-
Ventricular Septal Defect Muscular: Gross, natural color, view from right ventricle with probe in defect right ventricular hypertrophy is evident
-
Ventricular Septal Defect Muscular: Gross, natural color, view from left ventricle with probe in defect
-
Interventricular Septal Defect Subvalvular with Patch Repair: Gross natural color 19yo with Tetralogy of Fallot also shows overriding aorta



-
Interventricular Septal Defect Subvalvular with Patch Repair: Gross, natural color, close-up
-
Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, natural color, view from right ventricle. A case of inverted ventricles
-
Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, natural color, view from left ventricular outflow tract



-

Ventricular Septal Defect (Subvalvular): Gross, fixed tissue, small heart with opened aorta and subvalvular defect shown. A case of pulmonary artery atresia
-
Truncus Arteriosus with Subvalvular Ventricular Septal Defect: Gross, natural color, an excellent view of subvalvular defect. Quadricuspid truncus valve and type I origin of pulmonary arteries
-

runcus Arteriosus with Subvalvular Interventricular Septal Defect: Gross, natural color, defect is shown from the right side (view toward right ventricular outlet)



-
Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross natural color excellent view of lesion looking at opened aortic ring with quadricuspid aortic valve. A large subvalvular defect (origin of pulmonary arteries is at forceps)
-
Av Canal with Left Side Bjork Shiley Prosthetic Valve: Gross, natural color, a close-up view of valve and the bridging defect
-
Interventricular Septal Defect (Perimembranous) with Patch Repair: Gross, fixed tissue, a close-up view of patch repair from right ventricle



-

Conduit Right Ventricle to Pulmonary Artery: Gross, fixed tissue, opened conduit showing sutures into ventricle and patch closed perimembranous interventricular septal defect
-
Ventricular Septal Defect (Perimembranous): Gross, natural color, (quite good photo - lesion before the operation)
-
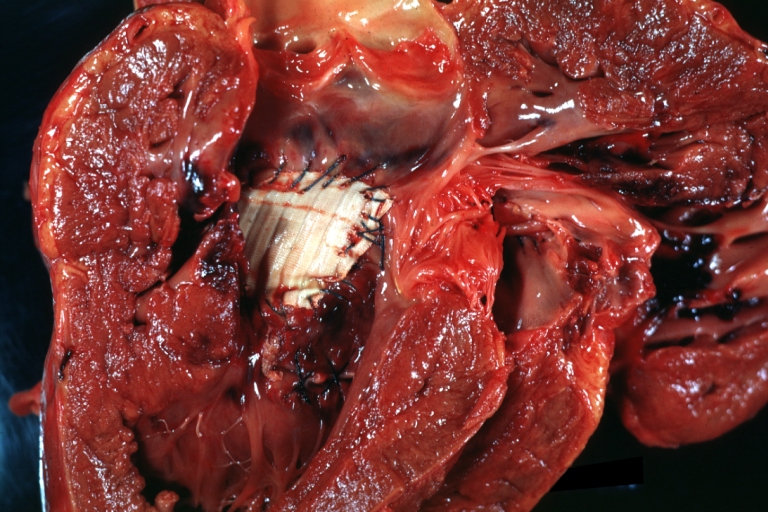
Ventricular Septal Defect (Subvalvular) Repaired: Tetralogy of Fallot; Gross, fixed tissue, close-up view of a large subvalvular defect repaired with a Dacron patch (overgrown with fibrous tissue prominent subaortic shelf with endocardial thickening).



-

Ventricular Septal Defect (Subvalvular) Repaired: Tetralogy of Fallot; Gross, fixed tissue, close-up view of a large subvalvular defect repaired with a Dacron patch
-
Ventricular Septal Defect (Subvalvular) Repaired: Gross, fixed tissue, close-up view of Dacron patch. Nearly completely covered with fibrous tissue
-
Transposition Great Vessels with Interventricular Septal Defect: Gross, fixed tissue, opened left ventricular outflow tract into a pulmonary artery (perimembranous defect)



-
Transposition Great Vessels with Interventricular Septal Defect: Gross, fixed tissue, close-up of interventricular septal defect and pulmonary valve
-

Double Outlet Right Ventricle: Gross, fixed tissue, close-up view of left ventricular outflow tract and patched ventricular septal defect. The override is obvious in this (very good) close-up view
-
Perimembranous Ventricular Septal Defect: Gross, fixed tissue, opened left ventricular outflow tract into aorta. Defect was patched 3 days prior to death



-
Perimembranous Ventricular Septal Defect: Gross, fixed tissue, lesion seen from right ventricle (with patch)
-
Perimembranous Interventricular Septal Defect: Gross, fixed tissue, view from right atrium and ventricle with patch placed three days prior to death.
-

Ventricular septal defect



-
Ventricular septal defect, view from left ventricle
-
Atrial Septal Defect, Septum Primum; View from Right Atrium (a 4 month old baby)
-
Atrial Septal Defect, Septum Primum; Also Cleft in Anterior Cusp of Mitral Valve



-
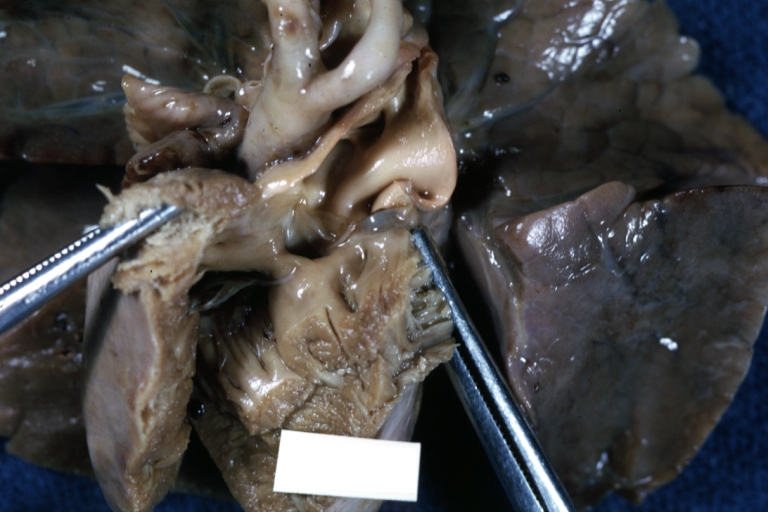
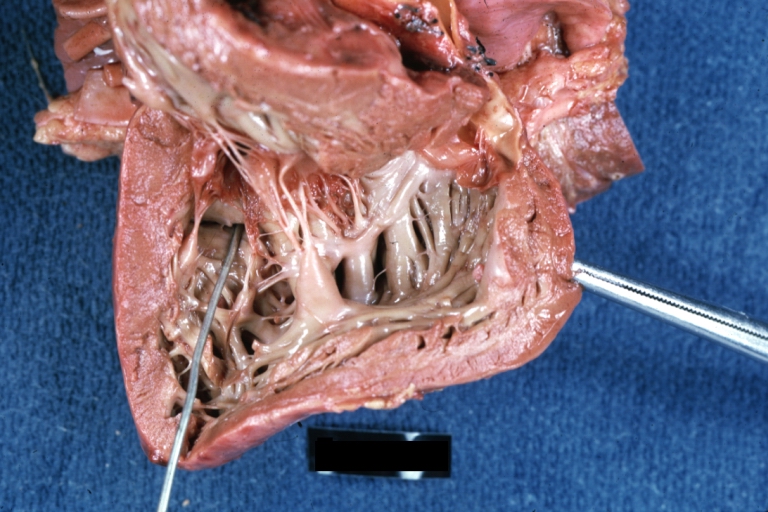
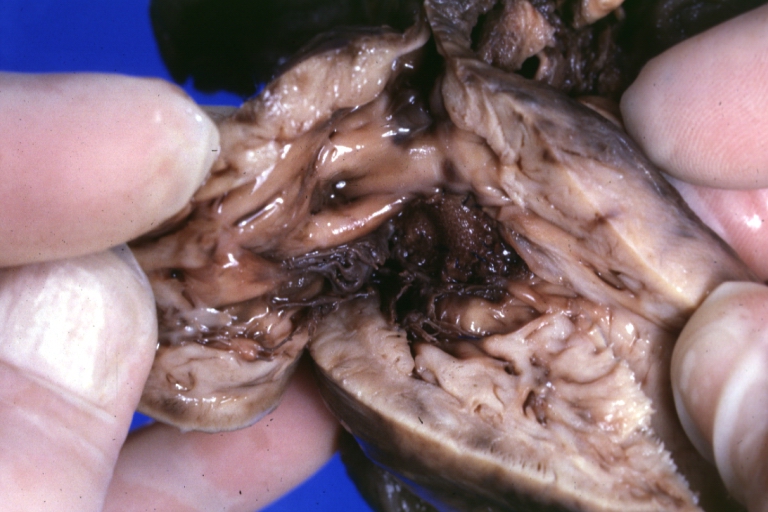
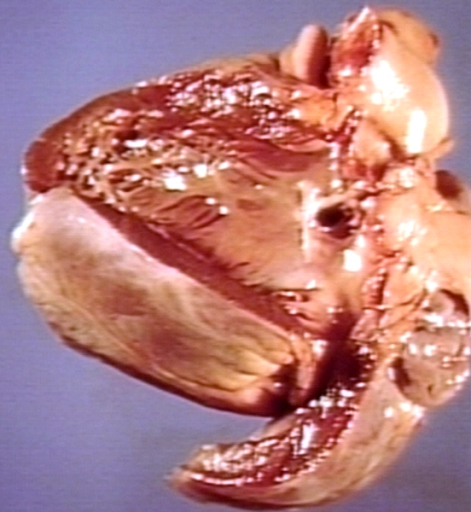
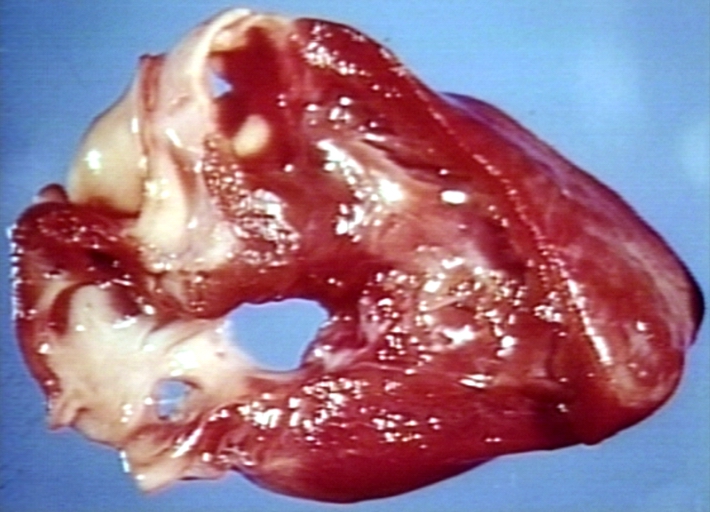
Hypoplastic left ventricle
-
Hypoplastic left ventricle
-
Hypoplastic left ventricle



-
Hypoplastic left ventricle
-
Hypoplastic left ventricle
-
Hypoplastic left ventricle



-
Patent Ductus Arteriosus: Gross example in an infant heart
-

Patent Ductus Arteriosus: Gross fixed tissue probe in ductus


-

Patent Ductus Arteriosus: Gross fixed tissue view of ductus opened from pulmonary artery into aorta with edematous appearing intimal surface
-
Patent Ductus Arteriosus: Gross natural color opened ductus in infant shows apparent intimal edema in ductus.


-
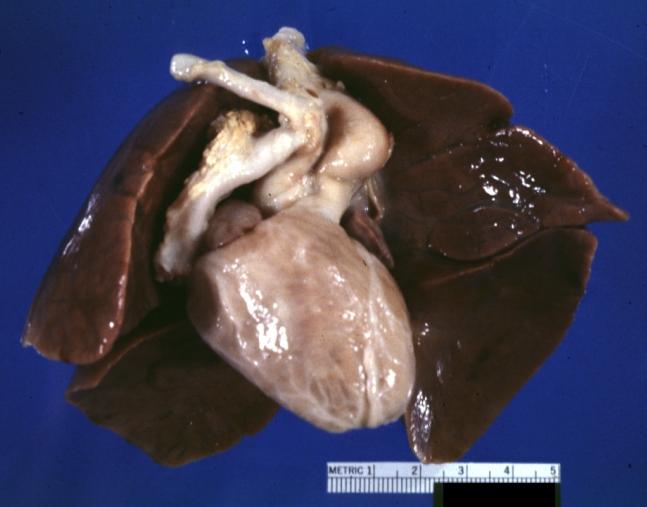
Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue external photo of heart shows the lesion
-

Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue aorta and ductus have been cross sectioned showing arch of aorta and huge ductus in a 5 day old infant


-

Patent Ductus Arteriosus with Aneurysmal Dilation: Gross fixed tissue opened aortic arch and descending thoracic showing very large opening of ductus into aorta
-
Patent Ductus Arteriosus


-

Right Ventricle Hypoplasia: Gross natural color good example showing tiny tricuspid inlet and very small but quite thick right ventricle
-
Right Ventricle Hypoplasia: Gross natural color view from right atrium showing patent foramen ovale and very small tricuspid valve
-
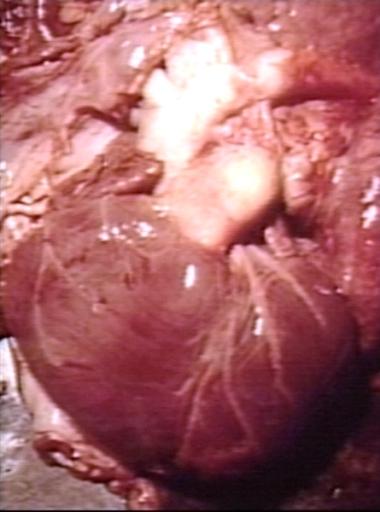
Right Ventricle Hypoplasia: Gross natural color external view of heart showing very large left ventricle and very small right ventricle delineated by anterior descending branch of left coronary artery



Defects
- Aortic stenosis
- Atrial septal defect (ASD)
- Atrioventricular septal defect (AVSD)
- Cardiomyopathy
- Coarctation of the aorta (CoA)
- Dextrocardia
- Ebstein's anomaly
- Hypoplastic left heart syndrome (HLHS)
- Interrupted aortic arch (IAA)
- levo-Transposition of the great arteries (l-TGA)
- Partial anomalous pulmonary venous connection (PAPVC)
- Patent ductus arteriosus (PDA)
- Pulmonary atresia
- Pulmonary stenosis
- Tetralogy of Fallot (ToF)
- Total anomalous pulmonary venous connection (TAPVC)
- dextro-Transposition of the great arteries (d-TGA)
- Tricuspid atresia
- Truncus arteriosus
- Ventricular septal defect (VSD)
- Bicuspid aortic valve
- Mitral Stenosis
References
- ↑ Geodakyan V. A., Sherman A. L. (1970). “Eksperimental’naja hirurgija i anesteziologija (Experimental surgery and anesthesiology) ” 32 N 2, 18–23.
- ↑ Geodakian VA, Sherman AL (1971). "[Relation of congenital anomalies to sex]". Zh. Obshch. Biol. (in Russian). 32 (4): 417–24. PMID 5146394.
- ↑ Rokitarisky K. E. (1875) Die defecte der Scheidewande des Herzens. Wien.
- ↑ Spitzer A. (1923) Arch. Pathol. Anat. 243, 81–272.
- ↑ Krimski L. D. (1963) Pathological anatomy of congenital heart defects and complications after their surgical treatment. M., Medicine.
See Also
External links
- It's My Heart, Inc. - A National Non-Profit Organization who supports and advocates for those affected by Congenital Heart Defects
- Template:DMOZ
- General information about congenital heart defects
- Down's Heart Group. A charity offering support and information relating to heart conditions associated with Down's Syndrome.