Canakinumab
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Canakinumab is a monoclonal antibody that is FDA approved for the treatment of Cryopyrin-Associated Periodic Syndromes (CAPS), Systemic Juvenile Idiopathic Arthritis (SJIA). Common adverse reactions include Injection site reaction, diarrhea, gastroenteritis , nausea , upper abdominal pain (systemic juvenile idiopathic arthritis, Infectious disease (systemic juvenile idiopathic arthritis, musculoskeletal pain, headache, vertigo, bronchitis, nasopharyngitis , pharyngitis, rhinitis.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Cryopyrin-Associated Periodic Syndromes (CAPS)
- ILARIS (canakinumab) is an interleukin-1β blocker indicated for the treatment of Cryopyrin-Associated Periodic Syndromes (CAPS), in adults and children 4 years of age and older including:
Familial Cold Autoinflammatory Syndrome (FCAS)
- Muckle-Wells Syndrome (MWS)
Systemic Juvenile Idiopathic Arthritis (SJIA)
- ILARIS is indicated for the treatment of active Systemic Juvenile Idiopathic Arthritis (SJIA) in patients aged 2 years and older.
General Dosing Information
- INJECTION FOR SUBCUTANEOUS USE ONLY.
Cryopyrin-Associated Periodic Syndromes (CAPS)
- The recommended dose of ILARIS is 150 mg for CAPS patients with body weight greater than 40 kg. For CAPS patients with body weight greater than or equal to 15 kg and less than or equal to 40 kg, the recommended dose is 2 mg/kg.
- For children 15 to 40 kg with an inadequate response, the dose can be increased to 3 mg/kg.
- ILARIS is administered every eight weeks as a single dose via subcutaneous injection.
Systemic Juvenile Idiopathic Arthritis (SJIA)
- The recommended dose of ILARIS for SJIA patients with a body weight greater than or equal to 7.5 kg is 4 mg/kg (with a maximum of 300 mg) administered every 4 weeks via subcutaneous injection.
Four Steps for Preparation and Administration
- STEP 1: Using aseptic technique, reconstitute each vial of ILARIS by slowly injecting 1 mL of preservative-free Sterile Water for Injection with a 1 mL syringe and an 18 gauge x 2” needle.
- STEP 2: Swirl the vial slowly at an angle of about 45° for approximately 1 minute and allow to stand for 5 minutes. Do not shake. Then gently turn the vial upside down and back again ten times. Avoid touching the rubber stopper with your fingers.
- STEP 3: Allow to stand for about 15 minutes at room temperature to obtain a clear solution. The reconstituted solution has a final concentration of 150 mg/mL. Do not shake. Do not use if particulate matter is present in the solution. Tap the side of the vial to remove any residual liquid from the stopper. The reconstituted solution should be essentially free from particulates, and clear to opalescent. The solution should be colorless or may have a slight brownish-yellow tint. If the solution has a distinctly brown discoloration it should not be used. If not used within 60 minutes of reconstitution, the solution should be stored in the refrigerator at 2°C to 8°C (36°F to 46°F) and used within 4 hours. Slight foaming of the product upon reconstitution is not unusual.
- STEP 4: Using a sterile syringe and needle carefully withdraw the required volume depending on the dose to be administered (0.2 mL to 1 mL) and subcutaneously inject using a 27 gauge x 0.5” needle.
- Injection into scar tissue should be avoided as this may result in insufficient exposure to ILARIS.
- ILARIS 180 mg powder for solution for injection is supplied in a single-use vial. Any unused product or waste material should be disposed of in accordance with local requirements.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Canakinumab in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Canakinumab in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Canakinumab in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Canakinumab in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Canakinumab in pediatric patients.
Contraindications
- Confirmed hypersensitivity to the active substance or to any of the excipients
Warnings
Serious Infections
- ILARIS has been associated with an increased risk of serious infections. Physicians should exercise caution when administering ILARIS to patients with infections, a history of recurring infections or underlying conditions which may predispose them to infections. ILARIS should not be administered to patients during an active infection requiring medical intervention. Administration of ILARIS should be discontinued if a patient develops a serious infection.
- Infections, predominantly of the upper respiratory tract, in some instances serious, have been reported with ILARIS. Generally, the observed infections responded to standard therapy. Isolated cases of unusual or opportunistic infections (e.g., aspergillosis, atypical mycobacterial infections, cytomegalovirus, herpes zoster) were reported during ILARIS treatment. A causal relationship of ILARIS to these events cannot be excluded. In clinical trials, ILARIS has not been administered concomitantly with tumor necrosis factor (TNF) inhibitors. An increased incidence of serious infections has been associated with administration of another IL-1 blocker in combination with TNF inhibitors. Coadministration of ILARIS with TNF inhibitors is not recommended because this may increase the risk of serious infections.
- Drugs that affect the immune system by blocking TNF have been associated with an increased risk of new tuberculosis and reactivation of latent tuberculosis (TB). It is possible that use of IL-1 inhibitors such as ILARIS increases the risk of reactivation of tuberculosis or of opportunistic infections.
- Prior to initiating immunomodulatory therapies, including ILARIS, patients should be evaluated for active and latent tuberculosis infection. Appropriate screening tests should be performed in all patients. ILARIS has not been studied in patients with a positive tuberculosis screen, and the safety of ILARIS in individuals with latent tuberculosis infection is unknown. Patients testing positive in tuberculosis screening should be treated according to standard medical practice prior to therapy with ILARIS. All patients should be instructed to seek medical advice if signs, symptoms, or high risk exposure suggestive of tuberculosis (e.g., persistent cough, weight loss, subfebrile temperature) appear during or after ILARIS therapy.
- Healthcare providers should follow current CDC guidelines both to evaluate for and to treat possible latent tuberculosis infections before initiating therapy with ILARIS.
Immunosuppression
- The impact of treatment with anti-interleukin-1 (IL-1) therapy on the development of malignancies is not known. However, treatment with immunosuppressants, including ILARIS, may result in an increase in the risk of malignancies.
Hypersensitivity
- Hypersensitivity reactions have been reported with ILARIS therapy. During clinical trials, no anaphylactic reactions have been reported. It should be recognized that symptoms of the underlying disease being treated may be similar to symptoms of hypersensitivity. ILARIS should not be administered to any patients with known clinical hypersensitivity to ILARIS.
Immunizations
- Live vaccines should not be given concurrently with ILARIS. Since no data are available on either the efficacy or on the risks of secondary transmission of infection by live vaccines in patients receiving ILARIS, live vaccines should not be given concurrently with ILARIS. In addition, because ILARIS may interfere with normal immune response to new antigens, vaccinations may not be effective in patients receiving ILARIS. No data are available on the effectiveness of vaccinations with inactivated (killed) antigens in patients receiving ILARIS.
- Because IL-1 blockade may interfere with immune response to infections, it is recommended that prior to initiation of therapy with ILARIS, adult and pediatric patients receive all recommended vaccinations, as appropriate, including pneumococcal vaccine and inactivated influenza vaccine.
Macrophage Activation Syndrome
- Macrophage activation syndrome (MAS) is a known, life-threatening disorder that may develop in patients with rheumatic conditions, in particular SJIA, and should be aggressively treated. Physicians should be attentive to symptoms of infection or worsening of SJIA, as these are known triggers for MAS. Eleven cases of MAS were observed in 201 SJIA patients treated with canakinumab in clinical trials. Based on the clinical trial experience, ILARIS does not appear to increase the incidence of MAS in SJIA patients, but no definitive conclusion can be made.
Adverse Reactions
Clinical Trials Experience
- Three hundred ninety-five patients, including approximately 250 children (aged 2 to 17 years) have been treated with ILARIS in interventional trials in CAPS or SJIA. The most frequently reported adverse drug reactions were infections predominantly of the upper respiratory tract. The majority of the events were mild to moderate although serious infections were observed. The type and frequency of adverse drug reactions appeared to be consistent over time.
- Opportunistic infections have also been reported in patients treated with ILARIS.
Clinical Trial Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Treatment of CAPS
- The data described herein reflect exposure to ILARIS in 104 adult and pediatric CAPS patients, including 20 FCAS, 72 MWS, 10 MWS/NOMID (Neonatal Onset Multisystem Inflammatory Disorder) overlap, 1 non-FCAS non-MWS, and 1 misdiagnosed in placebo-controlled (35 patients) and uncontrolled trials. Sixty-two patients were exposed to ILARIS for at least 6 months, 56 for at least 1 year and 4 for at least 3 years. A total of 9 serious adverse reactions were reported for CAPS patients. Among these were vertigo (2 patients), infections (3 patients), including intra-abdominal abscess following appendectomy (1 patient). The most commonly reported adverse reactions associated with ILARIS treatment in the CAPS patients were nasopharyngitis, diarrhea, influenza, headache, and nausea. One patient discontinued treatment due to potential infection.
- CAPS Study 1 investigated the safety of ILARIS in an 8-week, open-label period (Part 1), followed by a 24-week, randomized withdrawal period (Part 2), followed by a 16-week, open-label period (Part 3). All patients were treated with ILARIS 150 mg subcutaneously or 2 mg/kg if body weight was greater than or equal to 15 kg and less than or equal to 40 kg (see Table 1).
- Since all CAPS patients received ILARIS in Part 1, there are no controlled data on adverse events (AEs). Data in Table 1 are for all AEs for all CAPS patients receiving canakinumab. In CAPS Study 1, no pattern was observed for any type or frequency of adverse events throughout the three study periods.

This image is provided by the National Library of Medicine.

Vertigo
- Vertigo has been reported in 9% to 14% of patients in CAPS studies, exclusively in MWS patients, and reported as a serious adverse event in two cases. All events resolved with continued treatment with ILARIS.
Injection Site Reactions
- In CAPS Study 1, subcutaneous injection site reactions were observed in 9% of patients in Part 1 with mild tolerability reactions; in Part 2, one patient each (7%) had a mild or a moderate tolerability reaction and, in Part 3, one patient had a mild local tolerability reaction. No severe injection-site reactions were reported and none led to discontinuation of treatment.
Treatment of SJIA
- A total of 201 SJIA patients aged 2 to less than 20 years have received ILARIS in clinical trials. The safety of ILARIS compared to placebo was investigated in two phase 3 studies. Patients in SJIA Study 1 received a single dose of ILARIS 4 mg/kg (n=43) or placebo (n=41) via subcutaneous injection and were assessed at Day 15 for the efficacy endpoints and had a safety analysis up to Day 29. SJIA Study 2 was a two-part study with an open-label, single-arm active treatment period (Part I) followed by a randomized, double-blind, placebo-controlled, event-driven withdrawal design (Part II). Overall, 177 patients were enrolled into the study and received ILARIS 4 mg/kg (up to 300 mg maximum) in Part I, and 100 patients received ILARIS 4 mg/kg (up to 300 mg maximum) every 4 weeks or placebo in Part II. Adverse drug reactions listed in Table 2 showed higher rates than placebo from both trials. The adverse drug reactions associated with ILARIS treatment in SJIA patients were infections, abdominal pain, and injection site reactions. Serious infections (e.g., pneumonia, varicella, gastroenteritis, measles, sepsis, otitis media, sinusitis, adenovirus, lymph node abscess, pharyngitis) were observed in approximately 4% to 5% (0.02 to 0.17 per 100 patient-days) of patients receiving ILARIS in both studies.
- Adverse reactions are listed according to MedDRA version 15.0 system organ class.

This image is provided by the National Library of Medicine.

Hypersensitivity
- During clinical trials, no anaphylactic reactions have been reported. In CAPS trials one patient discontinued and in SJIA trials no patients discontinued due to hypersensitivity reactions. ILARIS should not be administered to any patients with known clinical hypersensitivity to ILARIS.
Immunogenicity
- A biosensor binding assay or a bridging immunoassay was used to detect antibodies directed against canakinumab in patients who received ILARIS. Antibodies against ILARIS were observed in approximately 1.5% and 3.1% of the patients treated with ILARIS for CAPS and SJIA, respectively. No neutralizing antibodies were detected. No apparent correlation of antibody development to clinical response or adverse events was observed. The CAPS clinical studies employed the biosensor binding assay, and most of the SJIA clinical studies employed the bridging assay. The data obtained in an assay are highly dependent on several factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications, underlying disease, and the number of patients tested. For these reasons, comparison of the incidence of antibodies to canakinumab between the CAPS and SJIA clinical studies or with the incidence of antibodies to other products may be misleading.
Laboratory Findings
Hematology
- During clinical trials with ILARIS, mean values decreased for white blood cells, neutrophils and platelets.
- In the randomized, placebo-controlled portion of SJIA Study 2 decreased white blood cell counts (WBC) less than or equal to 0.8 times lower limit of normal (LLN) were reported in 5 patients (10.4%)in the ILARIS group compared to 2 (4.0%) in the placebo group. Transient decreases in absolute neutrophil count (ANC) to less than 1x109/L were reported in 3 patients (6.0%) in the ILARIS group compared to1 patient (2.0%) in the placebo group. One case of ANC less than 0.5x109/L was observed in the ILARIS group and none in the placebo group.
- Mild (less than LLN and greater than 75x109/L) and transient decreases in platelet counts were observed in 3 (6.3%) ILARIS treated patients versus 1 (2.0%) placebo-treated patient.
Hepatic Transaminases
- Elevations of transaminases have been observed in patients treated with ILARIS.
- In the randomized, placebo-controlled portion of SJIA Study 2, high ALT and/or AST greater than or equal to 3 times upper limit of normal (ULN) were reported in 2 (4.1%) ILARIS-treated patients and 1 (2.0%) placebo patient. All patients had normal values at the next visit.
Bilirubin
- Asymptomatic and mild elevations of serum bilirubin have been observed in patients treated with ILARIS without concomitant elevations of transaminases.
Postmarketing Experience
There is limited information regarding Canakinumab Postmarketing Experience in the drug label.
Drug Interactions
- Interactions between ILARIS and other medicinal products have not been investigated in formal studies.
TNF-Blocker and IL-1 Blocking Agent
- An increased incidence of serious infections and an increased risk of neutropenia have been associated with administration of another IL-1 blocker in combination with TNF inhibitors in another patient population. Use of ILARIS with TNF inhibitors may also result in similar toxicities and is not recommended because this may increase the risk of serious infections.
- The concomitant administration of ILARIS with other drugs that block IL-1 has not been studied. Based upon the potential for pharmacological interactions between ILARIS and a recombinant IL-1ra, concomitant administration of ILARIS and other agents that block IL-1 or its receptors is not recommended.
Immunization
- No data are available on either the effects of live vaccination or the secondary transmission of infection by live vaccines in patients receiving ILARIS. Therefore, live vaccines should not be given concurrently with ILARIS. It is recommended that, if possible, pediatric and adult patients should complete all immunizations in accordance with current immunization guidelines prior to initiating ILARIS therapy.
Cytochrome P450 Substrates
- The formation of CYP450 enzymes is suppressed by increased levels of cytokines (e.g., IL-1) during chronic inflammation. Thus it is expected that for a molecule that binds to IL-1, such as canakinumab, the formation of CYP450 enzymes could be normalized. This is clinically relevant for CYP450 substrates with a narrow therapeutic index, where the dose is individually adjusted (e.g., warfarin). Upon initiation of canakinumab, in patients being treated with these types of medicinal products, therapeutic monitoring of the effect or drug concentration should be performed and the individual dose of the medicinal product may need to be adjusted as needed.
Use in Specific Populations
Pregnancy
- Canakinumab has been shown to produce delays in fetal skeletal development when evaluated in marmoset monkeys using doses 11-fold the maximum recommended human dose (MRHD) and greater (based on a plasma area under the time-concentration curve [AUC] comparison). Doses producing exposures within the clinical exposure range at the MRHD were not evaluated. Similar delays in fetal skeletal development were observed in mice administered a murine analog of canakinumab. There are no adequate and well-controlled studies of ILARIS in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
- Embryofetal developmental toxicity studies were performed in marmoset monkeys and mice. Pregnant marmoset monkeys were administered canakinumab subcutaneously twice-weekly at doses of 15, 50, or 150 mg/kg (representing 11- to 110-fold the human dose based on a plasma AUC comparison at the MRHD) from gestation days 25 to 109 which revealed no evidence of embryotoxicity or fetal malformations. There were increases in the incidence of incomplete ossification of the terminal caudal vertebra and misaligned and/or bipartite vertebra in fetuses at all dose levels when compared to concurrent controls suggestive of delay in skeletal development in the marmoset. Since canakinumab does not cross-react with mouse or rat IL-1, pregnant mice were subcutaneously administered a murine analog of canakinumab at doses of 15, 50, or 150 mg/kg on gestation days 6, 11, and 17. The incidence of incomplete ossification of the parietal and frontal skull bones of fetuses was increased in a dose-dependent manner at all dose levels tested.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Canakinumab in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Canakinumab during labor and delivery.
Nursing Mothers
- It is not known whether canakinumab is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when ILARIS is administered to a nursing woman.
Pediatric Use
- The CAPS trials with ILARIS included a total of 23 pediatric patients with an age range from 4 years to 17 years (11 adolescents were treated subcutaneously with 150 mg , and 12 children were treated with 2 mg/kg based on body weight greater than or equal to 15 kg and less than or equal to 40 kg). The majority of patients achieved improvement in clinical symptoms and objective markers of inflammation (e.g., Serum Amyloid A and C-Reactive Protein). Overall, the efficacy and safety of ILARIS in pediatric and adult patients were comparable. Infections of the upper respiratory tract were the most frequently reported infection. The safety and effectiveness of ILARIS in CAPS patients under 4 years of age has not been established
Geriatic Use
- Clinical studies of ILARIS did not include sufficient numbers of subjects aged 65 years and older to determine whether they respond differently from younger subjects.
Gender
There is no FDA guidance on the use of Canakinumab with respect to specific gender populations.
Race
There is no FDA guidance on the use of Canakinumab with respect to specific racial populations.
Renal Impairment
No formal studies have been conducted to examine the pharmacokinetics of ILARIS administered subcutaneously in patients with renal impairment.
Hepatic Impairment
No formal studies have been conducted to examine the pharmacokinetics of ILARIS administered subcutaneously in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Canakinumab in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Canakinumab in patients who are immunocompromised.
Administration and Monitoring
Administration
- Intravenous
Monitoring
There is limited information regarding Monitoring of Canakinumab in the drug label.
- Description
IV Compatibility
There is limited information regarding IV Compatibility of Canakinumab in the drug label.
Overdosage
- No confirmed case of overdose has been reported. In the case of overdose, it is recommended that the subject be monitored for any signs and symptoms of adverse reactions or effects, and appropriate symptomatic treatment be instituted immediately.
Pharmacology
Mechanism of Action
- Canakinumab is a human monoclonal anti-human IL-1β antibody of the IgG1/κ isotype. Canakinumab binds to human IL-1β and neutralizes its activity by blocking its interaction with IL-1 receptors, but it does not bind IL-1α or IL-1 receptor antagonist (IL-1ra).
- CAPS refer to rare genetic syndromes generally caused by mutations in the NLRP-3 [nucleotide-binding domain, leucine rich family (NLR), pyrin domain containing 3] gene (also known as Cold-Induced Auto-inflammatory Syndrome-1 [CIAS1]). CAPS disorders are inherited in an autosomal dominant pattern with male and female offspring equally affected. Features common to all disorders include fever, urticaria-like rash, arthralgia, myalgia, fatigue, and conjunctivitis.
The NLRP-3 gene encodes the protein cryopyrin, an important component of the inflammasome. Cryopyrin regulates the protease caspase-1 and controls the activation of interleukin-1 beta (IL-1β). Mutations in NLRP-3 result in an overactive inflammasome resulting in excessive release of activated IL-1β that drives inflammation. Systemic juvenile idiopathic arthritis (SJIA) is a severe autoinflammatory disease, driven by innate immunity by means of pro-inflammatory cytokines such as interleukin 1β (IL-1β).
Structure
- Canakinumab is a recombinant, human anti-human-IL-1β monoclonal antibody that belongs to the IgG1/κ isotype subclass. It is expressed in a murine Sp2/0-Ag14 cell line and comprised of two 447- (or 448-) residue heavy chains and two 214-residue light chains, with a molecular mass of 145157 Daltons when deglycosylated. Both heavy chains of canakinumab contain oligosaccharide chains linked to the protein backbone at asparagine 298 (Asn 298).
- The biological activity of canakinumab is measured by comparing its inhibition of IL-1β-dependent expression of the reporter gene luciferase to that of a canakinumab internal reference standard, using a stably transfected cell line.
- ILARIS is supplied in a sterile, single-use, colorless, 6 mL glass vial with coated stopper and aluminum flip-off cap. Each vial contains 180 mg of canakinumab as a white, preservative-free, lyophilized powder. Reconstitution with 1 mL of preservative-free Sterile Water for Injection is required prior to subcutaneous administration of the drug. The reconstituted canakinumab is a 150 mg/mL solution essentially free of particulates, clear to slightly opalescent, and is colorless or may have a slightly brownish-yellow tint. A volume of up to 1 mL can be withdrawn for delivery of 150 mg/mL canakinumab for subcutaneous administration. Each reconstituted vial contains 180 mg canakinumab, sucrose, L-histidine, L-histidine HCL monohydrate, polysorbate 80 and Sterile Water for Injection. No preservatives are present.
Pharmacodynamics
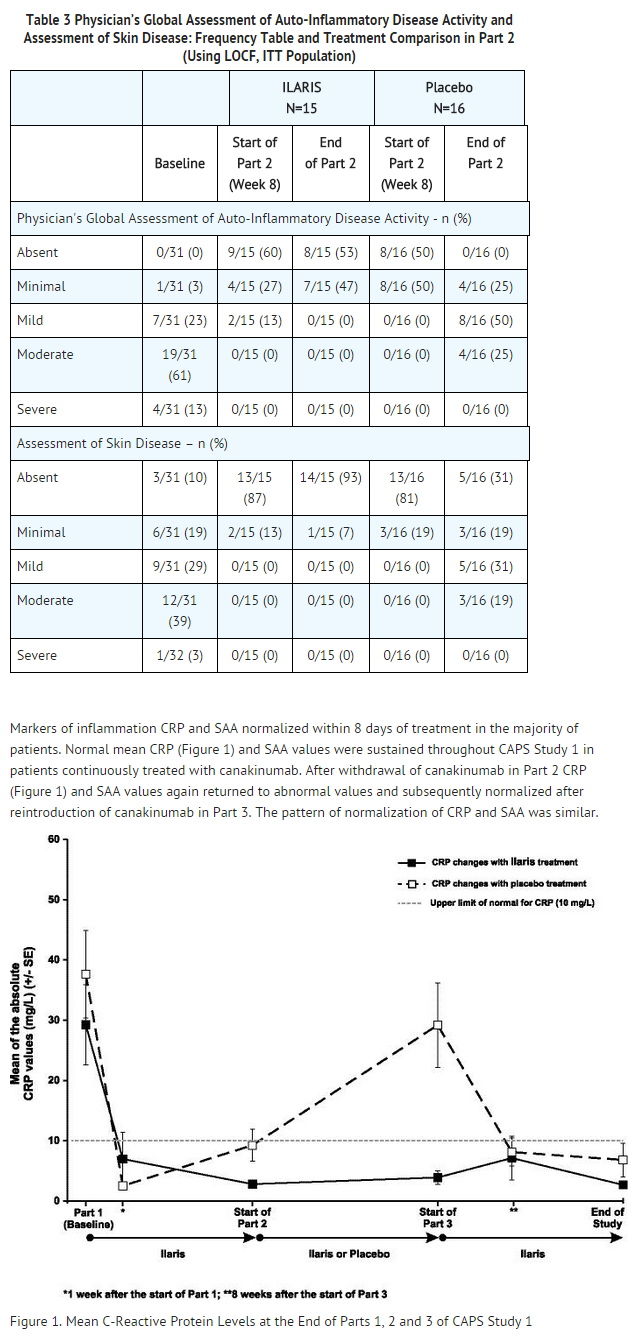
- C-reactive protein and Serum Amyloid A (SAA) are indicators of inflammatory disease activity that are elevated in patients with CAPS. Elevated SAA has been associated with the development of systemic amyloidosis in patients with CAPS. Following ILARIS treatment, CRP and SAA levels normalize within 8 days. In SJIA the median percent reduction in CRP from baseline to Day 15 was 91%. Improvement in pharmacodynamic markers may not be representative of clinical response.
Pharmacokinetics
Absorption
- The peak serum canakinumab concentration (Cmax) of 16 ± 3.5 mcg/mL occurred approximately 7 days after subcutaneous administration of a single, 150 mg dose subcutaneously to adult CAPS patients. The mean terminal half-life was 26 days. The absolute bioavailability of subcutaneous canakinumab was estimated to be 66%. Exposure parameters (such as AUC and Cmax) increased in proportion to dose over the dose range of 0.30 to 10 mg/kg given as intravenous infusion or from 150 to 300 mg as subcutaneous injection.
Distribution
- Canakinumab binds to serum IL-1β. Canakinumab volume of distribution (Vss) varied according to body weight and was estimated to be 6.01 liters in a typical CAPS patient weighing 70 kg, and 3.2 liters in a SJIA patient weighing 33 kg. The expected accumulation ratio was 1.3-fold for CAPS patients and 1.6-fold for SJIA patients following 6 months of subcutaneous dosing of 150 mg ILARIS every 8 weeks and 4 mg/kg every 4 weeks, respectively.
Elimination
- Clearance (CL) of canakinumab varied according to body weight and was estimated to be 0.174 L/day in a typical CAPS patient weighing 70 kg and 0.11 L/day in a SJIA patient weighing 33 kg. There was no indication of accelerated clearance or time-dependent change in the pharmacokinetic properties of canakinumab following repeated administration. No gender- or age-related pharmacokinetic differences were observed after correction for body weight.
Pediatrics
- Pharmacokinetic properties are similar in CAPS and SJIA pediatric populations.
- In CAPS patients, peak concentrations of canakinumab occurred between 2 to 7 days following single subcutaneous administration of ILARIS 150 mg or 2 mg/kg in pediatric patients. The terminal half-life ranged from 22.9 to 25.7 days, similar to the pharmacokinetic properties observed in adults.
- In SJIA, exposure parameters (such as AUC and Cmax) were comparable across age groups from 2 years of age and above following subcutaneous administration of canakinumab 4 mg/kg every 4 weeks.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, Impairment of Fertility
- Long-term animal studies have not been performed to evaluate the carcinogenic potential of canakinumab.
- The mutagenic potential of canakinumab was not evaluated.
- As canakinumab does not cross-react with rodent IL-1β, male and female fertility was evaluated in a mouse model using a murine analog of canakinumab. Male mice were treated weekly beginning 4 weeks prior to mating and continuing through 3 weeks after mating. Female mice were treated weekly for 2 weeks prior to mating through gestation day 3 or 4. The murine analog of canakinumab did not alter either male or female fertility parameters at subcutaneous doses up to 150 mg/kg.
Clinical Studies
Treatment of CAPS
- The efficacy and safety of ILARIS for the treatment of CAPS was demonstrated in CAPS Study 1, a 3-part trial in patients 9 to 74 years of age with the MWS phenotype of CAPS. Throughout the trial, patients weighing more than 40 kg received ILARIS 150 mg and patients weighing 15 to 40 kg received 2 mg/kg. Part 1 was an 8-week open-label, single-dose period where all patients received ILARIS. Patients who achieved a complete clinical response and did not relapse by Week 8 were randomized into Part 2, a 24-week randomized, double-blind, placebo-controlled withdrawal period. Patients who completed Part 2 or experienced a disease flare entered Part 3, a 16-week open-label active treatment phase. A complete response was defined as ratings of minimal or better for physician’s assessment of disease activity (PHY) and assessment of skin disease (SKD) and had serum levels of C-Reactive Protein (CRP) and Serum Amyloid A (SAA) less than 10 mg/L. A disease flare was defined as a CRP and/or SAA values greater than 30 mg/L and either a score of mild or worse for PHY or a score of minimal or worse for PHY and SKD.
- In Part 1, a complete clinical response was observed in 71% of patients one week following initiation of treatment and in 97% of patients by Week 8 (see Figure 1 and Table 3). In the randomized withdrawal period, a total of 81% of the patients randomized to placebo flared as compared to none (0%) of the patients randomized to ILARIS. The 95% confidence interval for treatment difference in the proportion of flares was 53% to 96%. At the end of Part 2, all 15 patients treated with ILARIS had absent or minimal disease activity and skin disease (see Table 3).
- In a second trial, patients 4 to 74 years of age with both MWS and FCAS phenotypes of CAPS were treated in an open-label manner. Treatment with ILARIS resulted in clinically significant improvement of signs and symptoms and in normalization of high CRP and SAA in a majority of patients within 1 week.
This image is provided by the National Library of Medicine.

Treatment of SJIA
- The efficacy of ILARIS for the treatment of active SJIA was assessed in 2 phase 3 studies (SJIA Study 1 and SJIA Study 2). Patients enrolled were aged 2 to less than 20 years (mean age at baseline: 8.5 years) with a confirmed diagnosis of SJIA at least 2 months before enrollment (mean disease duration at baseline: 3.5 years). Patients had active disease defined as greater than or equal to 2 joints with active arthritis (mean number of active joints at baseline: 15.4), documented spiking, intermittent fever (body temperature greater than 38°C) for at least 1 day within 1 week before study drug administration, and CRP greater than 30 mg/L (normal range less than 10 mg/L)(mean CRP at baseline: 200.5 mg/L). Patients were allowed to continue their stable dose of methotrexate, corticosteroids, and/or NSAIDs without change, except for tapering of the corticosteroid dose as per study design in SJIA Study 2 (see below).
- SJIA Study 1 was a randomized, double-blind, placebo-controlled, single-dose 4-week study assessing the short term efficacy of ILARIS in 84 patients randomized to receive a single subcutaneous dose of 4 mg/kg ILARIS or placebo (43 patients received ILARIS and 41 patients received placebo). The primary objective of this study was to demonstrate the superiority of ILARIS versus placebo in the proportion of patients who achieved at least 30% improvement in an adapted pediatric American College of Rheumatology (ACR) response criterion which included both the pediatric ACR core set (ACR30 response) and absence of fever (temperature less than or equal to 38°C in the preceding 7 days) at Day 15.
- Pediatric ACR responses are defined by achieving levels of percentage improvement (30%, 50%, and 70%) from baseline in at least 3 of the 6 core outcome variables, with worsening of greater than or equal to 30% in no more than one of the remaining variables. Core outcome variables included a physician global assessment of disease activity, parent or patient global assessment of wellbeing, number of joints with active arthritis, number of joints with limited range of motion, CRP, and functional ability (Childhood Health Assessment Questionnaire-CHAQ).
- Percentages of patients by pediatric ACR response are presented in Table 4.

This image is provided by the National Library of Medicine.

- Results for the components of the pediatric ACR core set were consistent with the overall ACR response results, for systemic and arthritic components including the reduction in the total number of active joints and joints with limited range of motion. Among the patients who returned for a Day 15 visit, the mean change in patient pain score (0 to 100 mm visual analogue scale) was -50.0 mm on ILARIS (N=43), as compared to +4.5 mm on placebo (N=25). The mean change in pain score among ILARIS treated patients was consistent through Day 29. All patients treated with ILARIS had no fever at Day 3 compared to 87% of patients treated with placebo.
- SJIA Study 2 was a randomized, double-blind, placebo-controlled, withdrawal study of flare prevention by ILARIS in patients with active SJIA. Flare was defined by worsening of greater than or equal to 30% in at least 3 of the 6 core Pediatric ACR response variables combined with improvement of greater than or equal to 30% in no more than 1 of the 6 variables, or reappearance of fever not due to infection for at least 2 consecutive days. The study consisted of 2 major parts. One hundred seventy-seven patients were enrolled in the study and received 4 mg/kg ILARIS subcutaneously every 4 weeks in Part I and 100 of these patients continued into Part II to receive either ILARIS 4 mg/kg or placebo subcutaneously every 4 weeks.
Corticosteroid Dose Tapering
- Of the total 128 patients who entered the open-label portion of Study 2 taking corticosteroids, 92 attempted corticosteroid tapering. Fifty-seven (62%) of the 92 patients who attempted to taper were able to successfully taper their corticosteroid dose and 42 (46%) discontinued corticosteroids.
- Time to Flare
- Part II was a randomized withdrawal design to demonstrate that the time to flare was longer with ILARIS than with placebo. Follow-up stopped when 37 events had been observed resulting in patients being followed for different lengths of time. The probability of experiencing a flare over time in Part II was statistically lower for the ILARIS treatment group than for the placebo group (Figure 2). This corresponded to a 64% relative reduction in the risk of flare for patients in the ILARIS group as compared to those in the placebo group (hazard ratio of 0.36; 95% CI: 0.17 to 0.75).

This image is provided by the National Library of Medicine.

How Supplied
- Carton of 1 vial………………………………………………………………………………………….NDC 0078-0582-61
- Each single-use vial of ILARIS contains a sterile, preservative free, white lyophilized powder containing 180 mg of canakinumab. Each vial is to be reconstituted with 1 mL of preservative-free Sterile Water for Injection resulting in a final concentration of 150 mg/mL.
Storage
- The unopened vial must be stored refrigerated at 2°C to 8°C (36°F to 46° F). Do not freeze. Store in the original carton to protect from light. Do not use beyond the date stamped on the label. After reconstitution, ILARIS should be kept from light, and can be kept at room temperature if used within 60 minutes of reconstitution. Otherwise, it should be refrigerated at 2°C to 8°C (36°F to 46°F) and used within 4 hours of reconstitution. ILARIS does not contain preservatives. Unused portions of ILARIS should be discarded.
- Keep this and all drugs out of the reach of children.
Images
Drug Images
{{#ask: Page Name::Canakinumab |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Canakinumab |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
- Patients should be advised of the potential benefits and risks of ILARIS. Physicians should instruct their patients to read the Medication Guide before starting ILARIS therapy.
Drug Administration
- Patients should be advised that healthcare providers should perform administration of ILARIS, by the subcutaneous injection route.
Infections
- Patients should be cautioned that ILARIS use has been associated with serious infections. Patients should be counseled to contact their healthcare professional immediately if they develop an infection after starting ILARIS. Treatment with ILARIS should be discontinued if a patient develops a serious infection. Patients should be counseled not to take any IL-1 blocking drug, including ILARIS, if they are also taking a drug that blocks TNF such as etanercept, infliximab, or adalimumab. Use of ILARIS with other IL-1 blocking agents, such as rilonacept and anakinra is not recommended. Patients should be cautioned not to receive ILARIS if they have a chronic or active infection, including HIV, Hepatitis B or Hepatitis C.
Vaccinations
- Prior to initiation of therapy with ILARIS, physicians should review with adult and pediatric patients their vaccination history relative to current medical guidelines for vaccine use, including taking into account the potential of increased risk of infection during treatment with ILARIS.
Injection-site Reactions
- Physicians should explain to patients that a very small number of patients in the clinical trials experienced a reaction at the subcutaneous injection site. Injection-site reactions may include pain, erythema, swelling, pruritus, bruising, mass, inflammation, dermatitis, edema, urticaria, vesicles, warmth, and hemorrhage. Healthcare providers should be cautioned to avoid injecting into an area that is already swollen or red. Any persistent reaction should be brought to the attention of the prescribing physician.
Hypersensitivity
- Patients should be counseled to contact their healthcare provider immediately if they develop signs of allergic reaction such as difficulty breathing or swallowing, nausea, dizziness, skin rash, itching, hives, palpitations or low blood pressure.
Precautions with Alcohol
- Alcohol-Canakinumab interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- ILARIS®[1]
Look-Alike Drug Names
There is limited information regarding Canakinumab Look-Alike Drug Names in the drug label.
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
{{#subobject:
|Label Page=Canakinumab |Label Name=Cana 07 Pack.jpg
}}
{{#subobject:
|Label Page=Canakinumab |Label Name=Cana06 Ingredients.png
}}