* There are no adequate and well-controlled studies of ADCETRIS in pregnant women. However, based on its mechanism of action and findings in animals, ADCETRIS can cause fetal harm when administered to a pregnant woman. Brentuximab vedotin caused embryo-fetal toxicities, including significantly decreased embryo viability and fetal malformations, in animals at maternal exposures that were similar to human exposures at the recommended doses for patients with HL and sALCL. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving the drug, the patient should be apprised of the potential hazard to the fetus.
* There are no adequate and well-controlled studies of ADCETRIS in pregnant women. However, based on its mechanism of action and findings in animals, ADCETRIS can cause fetal harm when administered to a pregnant woman. Brentuximab vedotin caused embryo-fetal toxicities, including significantly decreased embryo viability and fetal malformations, in animals at maternal exposures that were similar to human exposures at the recommended doses for patients with HL and sALCL. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving the drug, the patient should be apprised of the potential hazard to the fetus.
|clinicalTrials=The following serious adverse reactions are discussed in greater detail in other sections of the prescribing information:
|clinicalTrials=The following are serious adverse reactions.
* Peripheral neuropathy.
Peripheral neuropathy [see WARNINGS AND PRECAUTIONS (5.1)]
* Anaphylaxis and Infusion Reactions.
Anaphylaxis and Infusion Reactions [see WARNINGS AND PRECAUTIONS (5.2)]
* Hematologic Toxicities.
Hematologic Toxicities [see WARNINGS AND PRECAUTIONS (5.3)]
* Serious Infections and Opportunistic Infections.
Serious Infections and Opportunistic Infections [see WARNINGS AND PRECAUTIONS (5.4)]
* Tumor Lysis Syndrome.
Tumor Lysis Syndrome [see WARNINGS AND PRECAUTIONS (5.5)]
* Increased Toxicity in the Presence of Severe Renal Impairment.
Increased Toxicity in the Presence of Severe Renal Impairment [see WARNINGS AND PRECAUTIONS (5.6)]
* Increased Toxicity in the Presence of Moderate or Severe Hepatic Impairment.
Increased Toxicity in the Presence of Moderate or Severe Hepatic Impairment [see WARNINGS AND PRECAUTIONS (5.7)]
* Hepatotoxicity.
Hepatotoxicity [see WARNINGS AND PRECAUTIONS (5.8)]
* Progressive Multifocal Leukoencephalopathy.
Progressive Multifocal Leukoencephalopathy [see WARNINGS AND PRECAUTIONS (5.9)]
* Serious Dermatologic Reactions.
Serious Dermatologic Reactions [see WARNINGS AND PRECAUTIONS (5.10)]
* Embryo-Fetal Toxicity.
Embryo-Fetal Toxicity [see WARNINGS AND PRECAUTIONS (5.11)]
=====Clinical Trial Experience=====
6.1 Clinical Trial Experience
* Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
* ADCETRIS was studied as monotherapy in 160 patients in two phase 2 trials. Across both trials, the most common adverse reactions (≥20%), regardless of causality, were neutropenia, peripheral sensory neuropathy, fatigue, nausea, anemia, upper respiratory tract infection, diarrhea, pyrexia, rash, thrombocytopenia, cough, and vomiting. The most common adverse reactions occurring in at least 10% of patients in either trial, regardless of causality, using the NCI Common Toxicity Criteria Version 3.0, are shown in TABLE 2.
=====Experience in Hodgkin Lymphoma=====
ADCETRIS was studied as monotherapy in 160 patients in two phase 2 trials. Across both trials, the most common adverse reactions (≥20%), regardless of causality, were neutropenia, peripheral sensory neuropathy, fatigue, nausea, anemia, upper respiratory tract infection, diarrhea, pyrexia, rash, thrombocytopenia, cough, and vomiting. The most common adverse reactions occurring in at least 10% of patients in either trial, regardless of causality, using the NCI Common Toxicity Criteria Version 3.0, are shown in TABLE 2.
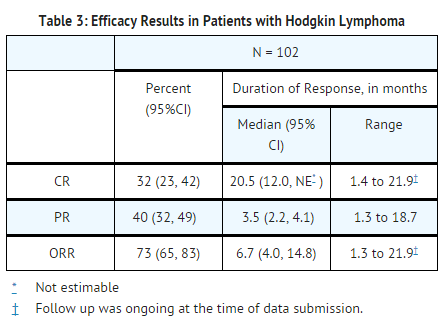
* ADCETRIS was studied in 102 patients with HL in a single arm clinical trial in which the recommended starting dose and schedule was 1.8 mg/kg intravenously every 3 weeks. Median duration of treatment was 27 weeks (range, 3 to 56 weeks).
* The most common adverse reactions (≥20%), regardless of causality, were neutropenia, peripheral sensory neuropathy, fatigue, upper respiratory tract infection, nausea, diarrhea, anemia, pyrexia, thrombocytopenia, rash, abdominal pain, cough, and vomiting.
Experience in Hodgkin Lymphoma
=====Pulmonary Toxicity=====
* In another clinical trial in patients with HL that studied ADCETRIS with bleomycin as part of a combination regimen, the rate of non-infectious pulmonary toxicity was higher than the historical incidence reported with ABVD (adriamycin, bleomycin, vinblastine, dacarbazine). Patients typically reported cough and dyspnea. Interstitial infiltration and/or inflammation were observed on radiographs and computed tomographic imaging of the chest. Most patients responded to corticosteroids. The concomitant use of ADCETRIS with bleomycin is contraindicated.
ADCETRIS was studied in 102 patients with HL in a single arm clinical trial in which the recommended starting dose and schedule was 1.8 mg/kg intravenously every 3 weeks. Median duration of treatment was 27 weeks (range, 3 to 56 weeks) [see CLINICAL STUDIES (14.1)].
* Experience in Systemic Anaplastic Large Cell Lymphoma
* ADCETRIS was studied in 58 patients with sALCL in a single arm clinical trial in which the recommended starting dose and schedule was 1.8 mg/kg intravenously every 3 weeks. Median duration of treatment was 24 weeks (range, 3 to 56 weeks).
The most common adverse reactions (≥20%), regardless of causality, were neutropenia, peripheral sensory neuropathy, fatigue, upper respiratory tract infection, nausea, diarrhea, anemia, pyrexia, thrombocytopenia, rash, abdominal pain, cough, and vomiting.
* The most common adverse reactions (≥20%), regardless of causality, were neutropenia, anemia, peripheral sensory neuropathy, fatigue, nausea, pyrexia, rash, diarrhea, and pain.
=====Combined Experience=====
Pulmonary Toxicity
: [[File:DailyMed - ADCETRIS - brentuximab vedotin injection, powder, lyophilized, for solution .png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
=====Infusion reactions=====
In another clinical trial in patients with HL that studied ADCETRIS with bleomycin as part of a combination regimen, the rate of non-infectious pulmonary toxicity was higher than the historical incidence reported with ABVD (adriamycin, bleomycin, vinblastine, dacarbazine). Patients typically reported cough and dyspnea. Interstitial infiltration and/or inflammation were observed on radiographs and computed tomographic imaging of the chest. Most patients responded to corticosteroids. The concomitant use of ADCETRIS with bleomycin is contraindicated [see CONTRAINDICATIONS (4)].
* Two cases of anaphylaxis were reported in phase 1 trials. There were no Grade 3 or 4 infusion-related reactions reported in the phase 2 trials, however, Grade 1 or 2 infusion-related reactions were reported for 19 patients (12%). The most common adverse reactions (≥2%) associated with infusion-related reactions were chills (4%), nausea (3%), dyspnea (3%), pruritus (3%), pyrexia (2%), and cough (2%).
=====Serious adverse reactions=====
Experience in Systemic Anaplastic Large Cell Lymphoma
* In the phase 2 trials, serious adverse reactions, regardless of causality, were reported in 31% of patients receiving ADCETRIS. The most common serious adverse reactions experienced by patients with HL include peripheral motor neuropathy (4%), abdominal pain (3%), pulmonary embolism (2%), pneumonitis (2%), pneumothorax (2%), pyelonephritis (2%), and pyrexia (2%). The most common serious adverse reactions experienced by patients with sALCL were septic shock (3%), supraventricular arrhythmia (3%), pain in extremity (3%), and urinary tract infection (3%). Other important serious adverse reactions reported include PML, Stevens-Johnson syndrome, and tumor lysis syndrome.
=====Dose modifications=====
ADCETRIS was studied in 58 patients with sALCL in a single arm clinical trial in which the recommended starting dose and schedule was 1.8 mg/kg intravenously every 3 weeks. Median duration of treatment was 24 weeks (range, 3 to 56 weeks) [see CLINICAL STUDIES (14.2)].
* Adverse reactions that led to dose delays in more than 5% of patients were neutropenia (14%) and peripheral sensory neuropathy (11%).
=====Discontinuations=====
The most common adverse reactions (≥20%), regardless of causality, were neutropenia, anemia, peripheral sensory neuropathy, fatigue, nausea, pyrexia, rash, diarrhea, and pain.
* Adverse reactions led to treatment discontinuation in 21% of patients. Adverse reactions that led to treatment discontinuation in 2 or more patients with HL or sALCL were peripheral sensory neuropathy (8%) and peripheral motor neuropathy (3%).
|postmarketing=* The following adverse reactions have been identified during post-approval use of ADCETRIS. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Combined Experience
* Blood and lymphatic system disorders
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
:* Febrile neutropenia
Infusion reactions
* Hepatobiliary disorders
: Hepatotoxicity
Two cases of anaphylaxis were reported in phase 1 trials. There were no Grade 3 or 4 infusion-related reactions reported in the phase 2 trials, however, Grade 1 or 2 infusion-related reactions were reported for 19 patients (12%). The most common adverse reactions (≥2%) associated with infusion-related reactions were chills (4%), nausea (3%), dyspnea (3%), pruritus (3%), pyrexia (2%), and cough (2%).
* Infections
:* PML
Serious adverse reactions
:* Serious infections and opportunistic infections.
* Metabolism and nutrition disorders
In the phase 2 trials, serious adverse reactions, regardless of causality, were reported in 31% of patients receiving ADCETRIS. The most common serious adverse reactions experienced by patients with HL include peripheral motor neuropathy (4%), abdominal pain (3%), pulmonary embolism (2%), pneumonitis (2%), pneumothorax (2%), pyelonephritis (2%), and pyrexia (2%). The most common serious adverse reactions experienced by patients with sALCL were septic shock (3%), supraventricular arrhythmia (3%), pain in extremity (3%), and urinary tract infection (3%). Other important serious adverse reactions reported include PML, Stevens-Johnson syndrome, and tumor lysis syndrome.
:* Hyperglycemia.
* Gastrointestinal disorders
Dose modifications
:* Pancreatitis (including fatal outcomes). Consider the diagnosis of pancreatitis for patients presenting with severe abdominal pain.
* Skin and subcutaneous tissue disorders
Adverse reactions that led to dose delays in more than 5% of patients were neutropenia (14%) and peripheral sensory neuropathy (11%) [see DOSAGE AND ADMINISTRATION (2.2)].
:* Toxic epidermal necrolysis, including fatal outcomes.
=====Immunogenicity=====
Discontinuations
* Patients with HL and sALCL in the phase 2 trials were tested for antibodies to brentuximab vedotin every 3 weeks using a sensitive electrochemiluminescent immunoassay. Approximately 7% of patients in these trials developed persistently positive antibodies (positive test at more than 2 timepoints) and 30% developed transiently positive antibodies (positive in 1 or 2 post-baseline timepoints).
* The anti-brentuximab antibodies were directed against the antibody component of brentuximab vedotin in all patients with transiently or persistently positive antibodies. Two of the patients (1%) with persistently positive antibodies experienced adverse reactions consistent with infusion reactions that led to discontinuation of treatment. Overall, a higher incidence of infusion related reactions was observed in patients who developed persistently positive antibodies.
Adverse reactions led to treatment discontinuation in 21% of patients. Adverse reactions that led to treatment discontinuation in 2 or more patients with HL or sALCL were peripheral sensory neuropathy (8%) and peripheral motor neuropathy (3%).
* A total of 58 patient samples that were either transiently or persistently positive for anti-brentuximab vedotin antibodies were tested for the presence of neutralizing antibodies. Sixty-two percent of these patients had at least one sample that was positive for the presence of neutralizing antibodies. The effect of anti-brentuximab vedotin antibodies on safety and efficacy is not known.
|postmarketing=The following adverse reactions have been identified during post-approval use of ADCETRIS. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
* Immunogenicity assay results are highly dependent on several factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of incidence of antibodies to ADCETRIS with the incidence of antibodies to other products may be misleading.
|drugInteractions=* In vitro data indicate that monomethyl auristatin E (MMAE) is a substrate and an inhibitor of CYP3A4/5. In vitro data indicate that MMAE is also a substrate of the efflux transporter P‑glycoprotein (P-gp).
Blood and lymphatic system disorders: febrile neutropenia [see WARNINGS AND PRECAUTIONS (5.3)].
Hepatobiliary disorders: hepatotoxicity [see WARNINGS AND PRECAUTIONS (5.8)].
Infections: PML [see BOXED WARNING, WARNINGS AND PRECAUTIONS (5.9)], serious infections and opportunistic infections [see WARNINGS AND PRECAUTIONS (5.4)].
Metabolism and nutrition disorders: hyperglycemia.
Gastrointestinal disorders: Pancreatitis (including fatal outcomes). Consider the diagnosis of pancreatitis for patients presenting with severe abdominal pain.
Skin and subcutaneous tissue disorders: Toxic epidermal necrolysis, including fatal outcomes [see WARNINGS AND PRECAUTIONS (5.10)].
6.3 Immunogenicity
Patients with HL and sALCL in the phase 2 trials [see CLINICAL STUDIES (14)] were tested for antibodies to brentuximab vedotin every 3 weeks using a sensitive electrochemiluminescent immunoassay. Approximately 7% of patients in these trials developed persistently positive antibodies (positive test at more than 2 timepoints) and 30% developed transiently positive antibodies (positive in 1 or 2 post-baseline timepoints). The anti-brentuximab antibodies were directed against the antibody component of brentuximab vedotin in all patients with transiently or persistently positive antibodies. Two of the patients (1%) with persistently positive antibodies experienced adverse reactions consistent with infusion reactions that led to discontinuation of treatment. Overall, a higher incidence of infusion related reactions was observed in patients who developed persistently positive antibodies.
A total of 58 patient samples that were either transiently or persistently positive for anti-brentuximab vedotin antibodies were tested for the presence of neutralizing antibodies. Sixty-two percent of these patients had at least one sample that was positive for the presence of neutralizing antibodies. The effect of anti-brentuximab vedotin antibodies on safety and efficacy is not known.
Immunogenicity assay results are highly dependent on several factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of incidence of antibodies to ADCETRIS with the incidence of antibodies to other products may be misleading.
|drugInteractions=* n vitro data indicate that monomethyl auristatin E (MMAE) is a substrate and an inhibitor of CYP3A4/5. In vitro data indicate that MMAE is also a substrate of the efflux transporter P‑glycoprotein (P-gp).
7.1 Effect of Other Drugs on ADCETRIS
7.1 Effect of Other Drugs on ADCETRIS
Line 167:
Line 148:
Co-administration of ADCETRIS did not affect exposure to midazolam, a CYP3A4 substrate. MMAE does not inhibit other CYP enzymes at relevant clinical concentrations [see CLINICAL PHARMACOLOGY (12.3)]. ADCETRIS is not expected to alter the exposure to drugs that are metabolized by CYP3A4 enzymes.
Co-administration of ADCETRIS did not affect exposure to midazolam, a CYP3A4 substrate. MMAE does not inhibit other CYP enzymes at relevant clinical concentrations [see CLINICAL PHARMACOLOGY (12.3)]. ADCETRIS is not expected to alter the exposure to drugs that are metabolized by CYP3A4 enzymes.
|FDAPregCat=D
|FDAPregCat=D
|useInPregnancyFDA=* Risk Summary
|useInPregnancyFDA======Risk Summary=====
* There are no adequate and well-controlled studies with ADCETRIS in pregnant women. However, based on its mechanism of action and findings in animals, ADCETRIS can cause fetal harm when administered to a pregnant woman. Brentuximab vedotin caused embryo-fetal toxicities in animals at maternal exposures that were similar to human exposures at the recommended doses for patients with HL and sALCL. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving this drug, the patient should be apprised of the potential hazard to the fetus.
There are no adequate and well-controlled studies with ADCETRIS in pregnant women. However, based on its mechanism of action and findings in animals, ADCETRIS can cause fetal harm when administered to a pregnant woman. Brentuximab vedotin caused embryo-fetal toxicities in animals at maternal exposures that were similar to human exposures at the recommended doses for patients with HL and sALCL. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving this drug, the patient should be apprised of the potential hazard to the fetus.
=====Animal Data=====
* In an embryo-fetal developmental study, pregnant rats received 2 intravenous doses of 0.3, 1, 3, or 10 mg/kg brentuximab vedotin during the period of organogenesis (once each on Pregnancy Days 6 and 13). Drug-induced embryo-fetal toxicities were seen mainly in animals treated with 3 and 10 mg/kg of the drug and included increased early resorption (≥99%), post-implantation loss (≥99%), decreased numbers of live fetuses, and external malformations (i.e., umbilical hernias and malrotated hindlimbs). Systemic exposure in animals at the brentuximab vedotin dose of 3 mg/kg is approximately the same exposure in patients with HL or sALCL who received the recommended dose of 1.8 mg/kg every three weeks.
Animal Data
In an embryo-fetal developmental study, pregnant rats received 2 intravenous doses of 0.3, 1, 3, or 10 mg/kg brentuximab vedotin during the period of organogenesis (once each on Pregnancy Days 6 and 13). Drug-induced embryo-fetal toxicities were seen mainly in animals treated with 3 and 10 mg/kg of the drug and included increased early resorption (≥99%), post-implantation loss (≥99%), decreased numbers of live fetuses, and external malformations (i.e., umbilical hernias and malrotated hindlimbs). Systemic exposure in animals at the brentuximab vedotin dose of 3 mg/kg is approximately the same exposure in patients with HL or sALCL who received the recommended dose of 1.8 mg/kg every three weeks.
|useInPregnancyAUS=* '''Australian Drug Evaluation Committee (ADEC) Pregnancy Category'''
|useInPregnancyAUS=* '''Australian Drug Evaluation Committee (ADEC) Pregnancy Category'''
Line 254:
Line 232:
<!--Pharmacodynamics-->
<!--Pharmacodynamics-->
|PD=* QT/QTc Prolongation Potential
|PD======QT/QTc Prolongation Potential=====
* The effect of brentuximab vedotin (1.8 mg/kg) on the QTc interval was evaluated in an open-label, single-arm study in 46 evaluable patients with CD30-expressing hematologic malignancies. Administration of brentuximab vedotin did not prolong the mean QTc interval >10 ms from baseline. Small increases in the mean QTc interval (<10 ms) cannot be excluded because this study did not include a placebo arm and a positive control arm.
The effect of brentuximab vedotin (1.8 mg/kg) on the QTc interval was evaluated in an open-label, single-arm study in 46 evaluable patients with CD30-expressing hematologic malignancies. Administration of brentuximab vedotin did not prolong the mean QTc interval >10 ms from baseline. Small increases in the mean QTc interval (<10 ms) cannot be excluded because this study did not include a placebo arm and a positive control arm.
|PK=* The pharmacokinetics of brentuximab vedotin were evaluated in phase 1 trials and in a population pharmacokinetic analysis of data from 314 patients. The pharmacokinetics of three analytes were determined: the ADC, MMAE, and total antibody. Total antibody had the greatest exposure and had a similar PK profile as the ADC. Hence, data on the PK of the ADC and MMAE have been summarized.
|PK=The pharmacokinetics of brentuximab vedotin were evaluated in phase 1 trials and in a population pharmacokinetic analysis of data from 314 patients. The pharmacokinetics of three analytes were determined: the ADC, MMAE, and total antibody. Total antibody had the greatest exposure and had a similar PK profile as the ADC. Hence, data on the PK of the ADC and MMAE have been summarized.
=====Absorption=====
* Maximum concentrations of ADC were typically observed close to the end of infusion. A multiexponential decline in ADC serum concentrations was observed with a terminal half-life of approximately 4 to 6 days. Exposures were approximately dose proportional from 1.2 to 2.7 mg/kg. Steady-state of the ADC was achieved within 21 days with every 3-week dosing of ADCETRIS, consistent with the terminal half-life estimate.
Absorption
* Minimal to no accumulation of ADC was observed with multiple doses at the every 3-week schedule.
* The time to maximum concentration for MMAE ranged from approximately 1 to 3 days. Similar to the ADC, steady‑state of MMAE was achieved within 21 days with every 3 week dosing of ADCETRIS. MMAE exposures decreased with continued administration of ADCETRIS with approximately 50% to 80% of the exposure of the first dose being observed at subsequent doses.
Maximum concentrations of ADC were typically observed close to the end of infusion. A multiexponential decline in ADC serum concentrations was observed with a terminal half-life of approximately 4 to 6 days. Exposures were approximately dose proportional from 1.2 to 2.7 mg/kg. Steady-state of the ADC was achieved within 21 days with every 3-week dosing of ADCETRIS, consistent with the terminal half-life estimate. Minimal to no accumulation of ADC was observed with multiple doses at the every 3-week schedule.
=====Distribution=====
* In vitro, the binding of MMAE to human plasma proteins ranged from 68–82%. MMAE is not likely to displace or to be displaced by highly protein-bound drugs. In vitro, MMAE was a substrate of P-gp and was not a potent inhibitor of P-gp.
The time to maximum concentration for MMAE ranged from approximately 1 to 3 days. Similar to the ADC, steady‑state of MMAE was achieved within 21 days with every 3 week dosing of ADCETRIS. MMAE exposures decreased with continued administration of ADCETRIS with approximately 50% to 80% of the exposure of the first dose being observed at subsequent doses.
* In humans, the mean steady state volume of distribution was approximately 6–10 L for ADC.
=====Metabolism=====
Distribution
* In vivo data in animals and humans suggest that only a small fraction of MMAE released from brentuximab vedotin is metabolized. In vitro data indicate that the MMAE metabolism that occurs is primarily via oxidation by CYP3A4/5. In vitro studies using human liver microsomes indicate that MMAE inhibits CYP3A4/5 but not other CYP isoforms. MMAE did not induce any major CYP450 enzymes in primary cultures of human hepatocytes.
=====Elimination=====
In vitro, the binding of MMAE to human plasma proteins ranged from 68–82%. MMAE is not likely to displace or to be displaced by highly protein-bound drugs. In vitro, MMAE was a substrate of P-gp and was not a potent inhibitor of P-gp.
* MMAE appeared to follow metabolite kinetics, with the elimination of MMAE appearing to be limited by its rate of release from ADC. An excretion study was undertaken in patients who received a dose of 1.8 mg/kg of ADCETRIS. Approximately 24% of the total MMAE administered as part of the ADC during an ADCETRIS infusion was recovered in both urine and feces over a 1-week period. Of the recovered MMAE, approximately 72% was recovered in the feces and the majority of the excreted MMAE was unchanged.
=====Specific Populations=====
In humans, the mean steady state volume of distribution was approximately 6–10 L for ADC.
* Effects of Gender, Age, and Race: Based on the population pharmacokinetic analysis; gender, age, and race do not have a meaningful effect on the pharmacokinetics of brentuximab vedotin.
|nonClinToxic======Carcinogenesis, Mutagenesis, and Impairment of Fertility=====
Metabolism
* Carcinogenicity studies with brentuximab vedotin or the small molecule (MMAE) have not been conducted.
* MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
In vivo data in animals and humans suggest that only a small fraction of MMAE released from brentuximab vedotin is metabolized. In vitro data indicate that the MMAE metabolism that occurs is primarily via oxidation by CYP3A4/5. In vitro studies using human liver microsomes indicate that MMAE inhibits CYP3A4/5 but not other CYP isoforms. MMAE did not induce any major CYP450 enzymes in primary cultures of human hepatocytes.
* Fertility studies with brentuximab vedotin or MMAE have not been conducted. However, results of repeat-dose toxicity studies in rats indicate the potential for brentuximab vedotin to impair male reproductive function and fertility. In a 4-week repeat-dose toxicity study in rats with weekly dosing at 0.5, 5 or 10 mg/kg brentuximab vedotin, seminiferous tubule degeneration, Sertoli cell vacuolation, reduced spermatogenesis, and aspermia were observed. Effects in animals were seen mainly at 5 and 10 mg/kg of brentuximab vedotin. These doses are approximately 3 and 6-fold the human recommended dose of 1.8 mg/kg, respectively, based on body weight.
|clinicalStudies======Carcinogenesis, Mutagenesis, and Impairment of Fertility=====
Elimination
* Carcinogenicity studies with brentuximab vedotin or the small molecule (MMAE) have not been conducted.
* MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
MMAE appeared to follow metabolite kinetics, with the elimination of MMAE appearing to be limited by its rate of release from ADC. An excretion study was undertaken in patients who received a dose of 1.8 mg/kg of ADCETRIS. Approximately 24% of the total MMAE administered as part of the ADC during an ADCETRIS infusion was recovered in both urine and feces over a 1-week period. Of the recovered MMAE, approximately 72% was recovered in the feces and the majority of the excreted MMAE was unchanged.
* Fertility studies with brentuximab vedotin or MMAE have not been conducted. However, results of repeat-dose toxicity studies in rats indicate the potential for brentuximab vedotin to impair male reproductive function and fertility. In a 4-week repeat-dose toxicity study in rats with weekly dosing at 0.5, 5 or 10 mg/kg brentuximab vedotin, seminiferous tubule degeneration, Sertoli cell vacuolation, reduced spermatogenesis, and aspermia were observed. Effects in animals were seen mainly at 5 and 10 mg/kg of brentuximab vedotin. These doses are approximately 3 and 6-fold the human recommended dose of 1.8 mg/kg, respectively, based on body weight.
: [[File:BV 06.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
Specific Populations
=====Systemic Anaplastic Large Cell Lymphoma=====
Effects of Gender, Age, and Race: Based on the population pharmacokinetic analysis;
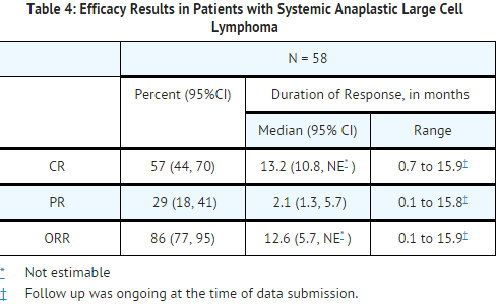
* The efficacy of ADCETRIS in patients with relapsed sALCL was evaluated in one phase 2 open-label, single-arm, multicenter trial. This trial included patients who had sALCL that was relapsed after prior therapy. Fifty-eight patients were treated with 1.8 mg/kg of ADCETRIS administered intravenously over 30 minutes every 3 weeks. An independent review facility performed efficacy evaluations which included overall response rate (ORR = complete remission [CR] + partial remission [PR]) and duration of response as defined by clinical and radiographic measures including computed tomography (CT) and positron-emission tomography (PET) as defined in the 2007 Revised Response Criteria for Malignant Lymphoma (modified).
gender, age, and race do not have a meaningful effect on the pharmacokinetics of
* The 58 patients ranged in age from 14–76 years (median, 52 years) and most were male (57%) and white (83%). Patients had received a median of 2 prior therapies; 26% of patients had received prior autologous stem cell transplant. Fifty percent (50%) of patients were relapsed and 50% of patients were refractory to their most recent prior therapy. Seventy-two percent (72%) were anaplastic lymphoma kinase (ALK)-negative.
brentuximab vedotin.
* The efficacy results are summarized in TABLE 4. Duration of response is calculated from date of first response to date of progression or data cutoff date.
|nonClinToxic=13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
: [[File:BV 07.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
Carcinogenicity studies with brentuximab vedotin or the small molecule (MMAE) have not been conducted.
MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
Fertility studies with brentuximab vedotin or MMAE have not been conducted. However, results of repeat-dose toxicity studies in rats indicate the potential for brentuximab vedotin to impair male reproductive function and fertility. In a 4-week repeat-dose toxicity study in rats with weekly dosing at 0.5, 5 or 10 mg/kg brentuximab vedotin, seminiferous tubule degeneration, Sertoli cell vacuolation, reduced spermatogenesis, and aspermia were observed. Effects in animals were seen mainly at 5 and 10 mg/kg of brentuximab vedotin. These doses are approximately 3 and 6-fold the human recommended dose of 1.8 mg/kg, respectively, based on body weight.
|clinicalStudies=13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility
Carcinogenicity studies with brentuximab vedotin or the small molecule (MMAE) have not been conducted.
MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
Fertility studies with brentuximab vedotin or MMAE have not been conducted. However, results of repeat-dose toxicity studies in rats indicate the potential for brentuximab vedotin to impair male reproductive function and fertility. In a 4-week repeat-dose toxicity study in rats with weekly dosing at 0.5, 5 or 10 mg/kg brentuximab vedotin, seminiferous tubule degeneration, Sertoli cell vacuolation, reduced spermatogenesis, and aspermia were observed. Effects in animals were seen mainly at 5 and 10 mg/kg of brentuximab vedotin. These doses are approximately 3 and 6-fold the human recommended dose of 1.8 mg/kg, respectively, based on body weight.
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
14.2 Systemic Anaplastic Large Cell Lymphoma
The efficacy of ADCETRIS in patients with relapsed sALCL was evaluated in one phase 2 open-label, single-arm, multicenter trial. This trial included patients who had sALCL that was relapsed after prior therapy. Fifty-eight patients were treated with 1.8 mg/kg of ADCETRIS administered intravenously over 30 minutes every 3 weeks. An independent review facility performed efficacy evaluations which included overall response rate (ORR = complete remission [CR] + partial remission [PR]) and duration of response as defined by clinical and radiographic measures including computed tomography (CT) and positron-emission tomography (PET) as defined in the 2007 Revised Response Criteria for Malignant Lymphoma (modified).
The 58 patients ranged in age from 14–76 years (median, 52 years) and most were male (57%) and white (83%). Patients had received a median of 2 prior therapies; 26% of patients had received prior autologous stem cell transplant. Fifty percent (50%) of patients were relapsed and 50% of patients were refractory to their most recent prior therapy. Seventy-two percent (72%) were anaplastic lymphoma kinase (ALK)-negative.
The efficacy results are summarized in TABLE 4. Duration of response is calculated from date of first response to date of progression or data cutoff date.
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
|howSupplied=* ADCETRIS (brentuximab vedotin) for Injection is supplied as a sterile, white to off-white preservative-free lyophilized cake or powder in individually-boxed single-use vials:
|howSupplied=* ADCETRIS (brentuximab vedotin) for Injection is supplied as a sterile, white to off-white preservative-free lyophilized cake or powder in individually-boxed single-use vials:
Line 308:
Line 267:
16.3 Special Handling
16.3 Special Handling
ADCETRIS is an antineoplastic product. Follow special handling and disposal procedures1.
ADCETRIS is an antineoplastic product. Follow special handling and disposal procedures1.
|storage=16.2 Storage
|storage=
Store vial at 2–8°C (36–46°F) in the original carton to protect from light.
* Store vial at 2–8°C (36–46°F) in the original carton to protect from light.
|packLabel=<!--Patient Counseling Information-->
|packLabel=<!--Patient Counseling Information-->
|fdaPatientInfo=* Peripheral neuropathy
|fdaPatientInfo======Peripheral Neuropathy=====
* Advise patients that ADCETRIS can cause a peripheral neuropathy. They should be advised to report to their health care provider any numbness or tingling of the hands or feet or any muscle weakness.
Advise patients that ADCETRIS can cause a peripheral neuropathy. They should be advised to report to their health care provider any numbness or tingling of the hands or feet or any muscle weakness [see WARNINGS AND PRECAUTIONS (5.1)].
=====Fever/Neutropenia=====
* Advise patients to contact their health care provider if a fever of 100.5°F or greater or other evidence of potential infection such as chills, cough, or pain on urination develops.
• Fever/Neutropenia
=====Infusion reactions=====
Advise patients to contact their health care provider if a fever of 100.5°F or greater or other evidence of potential infection such as chills, cough, or pain on urination develops [see WARNINGS AND PRECAUTIONS (5.3)].
* Advise patients to contact their health care provider if they experience signs and symptoms of infusion reactions including fever, chills, rash, or breathing problems within 24 hours of infusion.
=====Hepatotoxicity=====
• Infusion reactions
* Advise patients to report symptoms that may indicate liver injury, including fatigue, anorexia, right upper abdominal discomfort, dark urine, or jaundice.
Advise patients to contact their health care provider if they experience signs and symptoms of infusion reactions including fever, chills, rash, or breathing problems within 24 hours of infusion [see WARNINGS AND PRECAUTIONS (5.2)].
* Instruct patients receiving ADCETRIS to immediately report if they have any of the following neurological, cognitive, or behavioral signs and symptoms or if anyone close to them notices these signs and symptoms.
:• changes in mood or usual behavior
• Hepatotoxicity
:• confusion, thinking problems, loss of memory
:• changes in vision, speech, or walking
Advise patients to report symptoms that may indicate liver injury, including fatigue, anorexia, right upper abdominal discomfort, dark urine, or jaundice [see WARNINGS AND PRECAUTIONS (5.8)].
:• decreased strength or weakness on one side of the body
=====Pancreatitis=====
• Progressive multifocal leukoencephalopathy
* Advise patients to contact their health care provider if they develop severe abdominal pain.
=====Pregnancy and Nursing=====
Instruct patients receiving ADCETRIS to immediately report if they have any of the following neurological, cognitive, or behavioral signs and symptoms or if anyone close to them notices these signs and symptoms [see BOXED WARNING, WARNINGS AND PRECAUTIONS (5.9)].
* ADCETRIS can cause fetal harm. Advise women receiving ADCETRIS to avoid pregnancy. Advise patients to report pregnancy immediately. Advise patients to avoid nursing while receiving ADCETRIS.
• changes in mood or usual behavior
• confusion, thinking problems, loss of memory
• changes in vision, speech, or walking
• decreased strength or weakness on one side of the body
• Pancreatitis
Advise patients to contact their health care provider if they develop severe abdominal pain [see ADVERSE REACTIONS (6.2)].
• Pregnancy and Nursing
ADCETRIS can cause fetal harm. Advise women receiving ADCETRIS to avoid pregnancy. Advise patients to report pregnancy immediately [see WARNINGS AND PRECAUTIONS (5.11)]. Advise patients to avoid nursing while receiving ADCETRIS
|alcohol=* Alcohol-{{PAGENAME}} interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
|alcohol=* Alcohol-{{PAGENAME}} interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
See full prescribing information for complete Boxed Warning.
* JC virus infection resulting in PML and death can occur in patients receiving ADCETRIS
Overview
Brentuximab vedotin is a antibody-drug conjugate that is FDA approved for the treatment of Hodgkin Lymphoma, Systemic Anaplastic Large Cell Lymphoma. There is a Black Box Warning for this drug as shown here. Common adverse reactions include neutropenia, sensory neuropathy.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Hodgkin Lymphoma
ADCETRIS (brentuximab vedotin) is indicated for treatment of patients with Hodgkin lymphoma (HL) after failure of autologous stem cell transplant (ASCT) or after failure of at least two prior multi-agent chemotherapy regimens in patients who are not ASCT candidates.
This indication is approved under accelerated approval based on overall response rate. An improvement in patient-reported outcomes or survival has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
Systemic Anaplastic Large Cell Lymphoma
ADCETRIS is indicated for treatment of patients with systemic anaplastic large cell lymphoma (sALCL) after failure of at least one prior multi-agent chemotherapy regimen.
This indication is approved under accelerated approval based on overall response rate. An improvement in patient-reported outcomes or survival has not been established. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
Administer ADCETRIS as an intravenous infusion over 30 minutes every 3 weeks until disease progression or unacceptable toxicity.
This image is provided by the National Library of Medicine.
Dose Modification
Peripheral Neuropathy
For new or worsening Grade 2 or 3 neuropathy, dosing should be held until neuropathy improves to Grade 1 or baseline and then restarted at 1.2 mg/kg. For Grade 4 peripheral neuropathy, ADCETRIS should be discontinued.
Neutropenia
The dose of ADCETRIS should be held for Grade 3 or 4 neutropenia until resolution to baseline or Grade 2 or lower. Consider G-CSF prophylaxis for subsequent cycles in patients who experience Grade 3 or 4 neutropenia in the previous cycle. In patients with recurrent Grade 4 neutropenia despite the use of G-CSF prophylaxis, consider discontinuation or dose reduction of ADCETRIS to1.2 mg/kg.
Instructions for Preparation and Administration
Administration
Administer ADCETRIS as an intravenous infusion only.
Do not mix ADCETRIS with, or administer as an infusion with, other medicinal products.
Reconstitution
Follow procedures for proper handling and disposal of anticancer drugs.
Use appropriate aseptic technique for reconstitution and preparation of dosing solutions.
Determine the number of 50 mg vials needed based on the patient’s weight and the prescribed dose.
Reconstitute each 50 mg vial of ADCETRIS with 10.5 mL of Sterile Water for Injection, USP, to yield a single-use solution containing 5 mg/mL brentuximab vedotin.
Direct the stream toward the wall of vial and not directly at the cake or powder.
Gently swirl the vial to aid dissolution. DO NOT SHAKE.
Inspect the reconstituted solution for particulates and discoloration. The reconstituted solution should be clear to slightly opalescent, colorless, and free of visible particulates.
Following reconstitution, dilute immediately into an infusion bag. If not diluted immediately, store the solution at 2–8°C (36–46°F) and use within 24 hours of reconstitution. DO NOT FREEZE.
Discard any unused portion left in the vial.
Dilution
Calculate the required volume of 5 mg/mL reconstituted ADCETRIS solution needed.
Withdraw this amount from the vial and immediately add it to an infusion bag containing a minimum volume of 100 mL of 0.9% Sodium Chloride Injection, 5% Dextrose Injection or Lactated Ringer's Injection to achieve a final concentration of 0.4 mg/mL to 1.8 mg/mL brentuximab vedotin.
Gently invert the bag to mix the solution.
Following dilution, infuse the ADCETRIS solution immediately. If not used immediately, store the solution at 2–8°C (36–46°F) and use within 24 hours of reconstitution. DO NOT FREEZE.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Brentuximab vedotin in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Brentuximab vedotin in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Brentuximab vedotin in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Brentuximab vedotin in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Brentuximab vedotin in pediatric patients.
Contraindications
ADCETRIS is contraindicated with concomitant bleomycin due to pulmonary toxicity (e.g., interstitial infiltration and/or inflammation)
See full prescribing information for complete Boxed Warning.
* JC virus infection resulting in PML and death can occur in patients receiving ADCETRIS
Peripheral Neuropathy
ADCETRIS treatment causes a peripheral neuropathy that is predominantly sensory. Cases of peripheral motor neuropathy have also been reported. ADCETRIS-induced peripheral neuropathy is cumulative. In the HL and sALCL clinical trials, 54% of patients experienced any grade of neuropathy. Of these patients, 49% had complete resolution, 31% had partial improvement, and 20% had no improvement. Of the patients who reported neuropathy, 51% had residual neuropathy at the time of their last evaluation. Monitor patients for symptoms of neuropathy, such as hypoesthesia, hyperesthesia, paresthesia, discomfort, a burning sensation, neuropathic pain, or weakness.
Patients experiencing new or worsening peripheral neuropathy may require a delay, change in dose, or discontinuation of ADCETRIS.
Anaphylaxis and Infusion Reactions
Infusion-related reactions, including anaphylaxis, have occurred with ADCETRIS. Monitor patients during infusion. If anaphylaxis occurs, immediately and permanently discontinue administration of ADCETRIS and administer appropriate medical therapy. If an infusion-related reaction occurs, the infusion should be interrupted and appropriate medical management instituted. Patients who have experienced a prior infusion-related reaction should be premedicated for subsequent infusions. Premedication may include acetaminophen, an antihistamine, and a corticosteroid.
Hematologic Toxicities
Prolonged (≥1 week) severe neutropenia and Grade 3 or Grade 4 thrombocytopenia or anemia can occur with ADCETRIS. Febrile neutropenia has been reported with treatment with ADCETRIS. Complete blood counts should be monitored prior to each dose of ADCETRIS and more frequent monitoring should be considered for patients with Grade 3 or 4 neutropenia. Monitor patients for fever. If Grade 3 or 4 neutropenia develops, consider dose delays, reductions, discontinuation, or G-CSF prophylaxis with subsequent ADCETRIS doses.
Serious Infections and Opportunistic Infections
Serious infections and opportunistic infections such as pneumonia, bacteremia, and sepsis or septic shock (including fatal outcomes) have been reported in patients treated with ADCETRIS. Patients should be closely monitored during treatment for the emergence of possible bacterial, fungal, or viral infections.
Tumor Lysis Syndrome
Patients with rapidly proliferating tumor and high tumor burden may be at increased risk of tumor lysis syndrome. Monitor closely and take appropriate measures.
Increased Toxicity in the Presence of Severe Renal Impairment
The frequency of ≥Grade 3 adverse reactions and deaths was greater in patients with severe renal impairment compared to patients with normal renal function. Due to higher MMAE exposure, ≥Grade 3 adverse reactions may be more frequent in patients with severe renal impairment compared to patients with normal renal function. Avoid the use of ADCETRIS in patients with severe renal impairment [creatinine clearance (CLcr) <30 mL/min].
Increased Toxicity in the Presence of Moderate or Severe Hepatic Impairment
The frequency of ≥Grade 3 adverse reactions and deaths was greater in patients with moderate and severe hepatic impairment compared to patients with normal hepatic function. Avoid the use of ADCETRIS in patients with moderate (Child-Pugh B) or severe (Child-Pugh C) hepatic impairment.
Hepatotoxicity
Serious cases of hepatotoxicity, including fatal outcomes, have occurred in patients receiving ADCETRIS. Cases were consistent with hepatocellular injury, including elevations of transaminases and/or bilirubin. Cases have occurred after the first dose of ADCETRIS or after ADCETRIS rechallenge. Preexisting liver disease, elevated baseline liver enzymes, and concomitant medications may also increase the risk. Monitor liver enzymes and bilirubin. Patients experiencing new, worsening, or recurrent hepatotoxicity may require a delay, change in dose, or discontinuation of ADCETRIS.
Progressive Multifocal Leukoencephalopathy
JC virus infection resulting in PML and death has been reported in ADCETRIS-treated patients. In addition to ADCETRIS therapy, other possible contributory factors include prior therapies and underlying disease that may cause immunosuppression. Consider the diagnosis of PML in any patient presenting with new-onset signs and symptoms of central nervous system abnormalities.
Hold ADCETRIS dosing for any suspected case of PML and discontinue ADCETRIS dosing if a diagnosis of PML is confirmed.
Serious Dermatologic Reactions
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), including fatal outcomes, have been reported with ADCETRIS. If SJS or TEN occurs, discontinue ADCETRIS and administer appropriate medical therapy.
Embryo-Fetal Toxicity
There are no adequate and well-controlled studies of ADCETRIS in pregnant women. However, based on its mechanism of action and findings in animals, ADCETRIS can cause fetal harm when administered to a pregnant woman. Brentuximab vedotin caused embryo-fetal toxicities, including significantly decreased embryo viability and fetal malformations, in animals at maternal exposures that were similar to human exposures at the recommended doses for patients with HL and sALCL. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving the drug, the patient should be apprised of the potential hazard to the fetus.
Adverse Reactions
Clinical Trials Experience
The following are serious adverse reactions.
Peripheral neuropathy.
Anaphylaxis and Infusion Reactions.
Hematologic Toxicities.
Serious Infections and Opportunistic Infections.
Tumor Lysis Syndrome.
Increased Toxicity in the Presence of Severe Renal Impairment.
Increased Toxicity in the Presence of Moderate or Severe Hepatic Impairment.
Hepatotoxicity.
Progressive Multifocal Leukoencephalopathy.
Serious Dermatologic Reactions.
Embryo-Fetal Toxicity.
Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
ADCETRIS was studied as monotherapy in 160 patients in two phase 2 trials. Across both trials, the most common adverse reactions (≥20%), regardless of causality, were neutropenia, peripheral sensory neuropathy, fatigue, nausea, anemia, upper respiratory tract infection, diarrhea, pyrexia, rash, thrombocytopenia, cough, and vomiting. The most common adverse reactions occurring in at least 10% of patients in either trial, regardless of causality, using the NCI Common Toxicity Criteria Version 3.0, are shown in TABLE 2.
Experience in Hodgkin Lymphoma
ADCETRIS was studied in 102 patients with HL in a single arm clinical trial in which the recommended starting dose and schedule was 1.8 mg/kg intravenously every 3 weeks. Median duration of treatment was 27 weeks (range, 3 to 56 weeks).
The most common adverse reactions (≥20%), regardless of causality, were neutropenia, peripheral sensory neuropathy, fatigue, upper respiratory tract infection, nausea, diarrhea, anemia, pyrexia, thrombocytopenia, rash, abdominal pain, cough, and vomiting.
Pulmonary Toxicity
In another clinical trial in patients with HL that studied ADCETRIS with bleomycin as part of a combination regimen, the rate of non-infectious pulmonary toxicity was higher than the historical incidence reported with ABVD (adriamycin, bleomycin, vinblastine, dacarbazine). Patients typically reported cough and dyspnea. Interstitial infiltration and/or inflammation were observed on radiographs and computed tomographic imaging of the chest. Most patients responded to corticosteroids. The concomitant use of ADCETRIS with bleomycin is contraindicated.
Experience in Systemic Anaplastic Large Cell Lymphoma
ADCETRIS was studied in 58 patients with sALCL in a single arm clinical trial in which the recommended starting dose and schedule was 1.8 mg/kg intravenously every 3 weeks. Median duration of treatment was 24 weeks (range, 3 to 56 weeks).
The most common adverse reactions (≥20%), regardless of causality, were neutropenia, anemia, peripheral sensory neuropathy, fatigue, nausea, pyrexia, rash, diarrhea, and pain.
Combined Experience
This image is provided by the National Library of Medicine.
Infusion reactions
Two cases of anaphylaxis were reported in phase 1 trials. There were no Grade 3 or 4 infusion-related reactions reported in the phase 2 trials, however, Grade 1 or 2 infusion-related reactions were reported for 19 patients (12%). The most common adverse reactions (≥2%) associated with infusion-related reactions were chills (4%), nausea (3%), dyspnea (3%), pruritus (3%), pyrexia (2%), and cough (2%).
Serious adverse reactions
In the phase 2 trials, serious adverse reactions, regardless of causality, were reported in 31% of patients receiving ADCETRIS. The most common serious adverse reactions experienced by patients with HL include peripheral motor neuropathy (4%), abdominal pain (3%), pulmonary embolism (2%), pneumonitis (2%), pneumothorax (2%), pyelonephritis (2%), and pyrexia (2%). The most common serious adverse reactions experienced by patients with sALCL were septic shock (3%), supraventricular arrhythmia (3%), pain in extremity (3%), and urinary tract infection (3%). Other important serious adverse reactions reported include PML, Stevens-Johnson syndrome, and tumor lysis syndrome.
Dose modifications
Adverse reactions that led to dose delays in more than 5% of patients were neutropenia (14%) and peripheral sensory neuropathy (11%).
Discontinuations
Adverse reactions led to treatment discontinuation in 21% of patients. Adverse reactions that led to treatment discontinuation in 2 or more patients with HL or sALCL were peripheral sensory neuropathy (8%) and peripheral motor neuropathy (3%).
Postmarketing Experience
The following adverse reactions have been identified during post-approval use of ADCETRIS. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and lymphatic system disorders
Febrile neutropenia
Hepatobiliary disorders
Hepatotoxicity
Infections
PML
Serious infections and opportunistic infections.
Metabolism and nutrition disorders
Hyperglycemia.
Gastrointestinal disorders
Pancreatitis (including fatal outcomes). Consider the diagnosis of pancreatitis for patients presenting with severe abdominal pain.
Skin and subcutaneous tissue disorders
Toxic epidermal necrolysis, including fatal outcomes.
Immunogenicity
Patients with HL and sALCL in the phase 2 trials were tested for antibodies to brentuximab vedotin every 3 weeks using a sensitive electrochemiluminescent immunoassay. Approximately 7% of patients in these trials developed persistently positive antibodies (positive test at more than 2 timepoints) and 30% developed transiently positive antibodies (positive in 1 or 2 post-baseline timepoints).
The anti-brentuximab antibodies were directed against the antibody component of brentuximab vedotin in all patients with transiently or persistently positive antibodies. Two of the patients (1%) with persistently positive antibodies experienced adverse reactions consistent with infusion reactions that led to discontinuation of treatment. Overall, a higher incidence of infusion related reactions was observed in patients who developed persistently positive antibodies.
A total of 58 patient samples that were either transiently or persistently positive for anti-brentuximab vedotin antibodies were tested for the presence of neutralizing antibodies. Sixty-two percent of these patients had at least one sample that was positive for the presence of neutralizing antibodies. The effect of anti-brentuximab vedotin antibodies on safety and efficacy is not known.
Immunogenicity assay results are highly dependent on several factors including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of incidence of antibodies to ADCETRIS with the incidence of antibodies to other products may be misleading.
Drug Interactions
In vitro data indicate that monomethyl auristatin E (MMAE) is a substrate and an inhibitor of CYP3A4/5. In vitro data indicate that MMAE is also a substrate of the efflux transporter P‑glycoprotein (P-gp).
7.1 Effect of Other Drugs on ADCETRIS
CYP3A4 Inhibitors/Inducers: MMAE is primarily metabolized by CYP3A [see CLINICAL PHARMACOLOGY (12.3)]. Co-administration of ADCETRIS with ketoconazole, a potent CYP3A4 inhibitor, increased exposure to MMAE by approximately 34%. Patients who are receiving strong CYP3A4 inhibitors concomitantly with ADCETRIS should be closely monitored for adverse reactions. Co-administration of ADCETRIS with rifampin, a potent CYP3A4 inducer, reduced exposure to MMAE by approximately 46%.
P-gp Inhibitors: Co-administration of ADCETRIS with P-gp inhibitors may increase exposure to MMAE. Patients who are receiving P-gp inhibitors concomitantly with ADCETRIS should be closely monitored for adverse reactions.
7.2 Effect of ADCETRIS on Other Drugs
Co-administration of ADCETRIS did not affect exposure to midazolam, a CYP3A4 substrate. MMAE does not inhibit other CYP enzymes at relevant clinical concentrations [see CLINICAL PHARMACOLOGY (12.3)]. ADCETRIS is not expected to alter the exposure to drugs that are metabolized by CYP3A4 enzymes.
There are no adequate and well-controlled studies with ADCETRIS in pregnant women. However, based on its mechanism of action and findings in animals, ADCETRIS can cause fetal harm when administered to a pregnant woman. Brentuximab vedotin caused embryo-fetal toxicities in animals at maternal exposures that were similar to human exposures at the recommended doses for patients with HL and sALCL. If this drug is used during pregnancy, or if the patient becomes pregnant while receiving this drug, the patient should be apprised of the potential hazard to the fetus.
Animal Data
In an embryo-fetal developmental study, pregnant rats received 2 intravenous doses of 0.3, 1, 3, or 10 mg/kg brentuximab vedotin during the period of organogenesis (once each on Pregnancy Days 6 and 13). Drug-induced embryo-fetal toxicities were seen mainly in animals treated with 3 and 10 mg/kg of the drug and included increased early resorption (≥99%), post-implantation loss (≥99%), decreased numbers of live fetuses, and external malformations (i.e., umbilical hernias and malrotated hindlimbs). Systemic exposure in animals at the brentuximab vedotin dose of 3 mg/kg is approximately the same exposure in patients with HL or sALCL who received the recommended dose of 1.8 mg/kg every three weeks.
Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Brentuximab vedotin in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Brentuximab vedotin during labor and delivery.
Nursing Mothers
It is not known whether brentuximab vedotin is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from ADCETRIS a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
The safety and effectiveness of ADCETRIS have not been established in the pediatric population. Clinical trials of ADCETRIS included only 9 pediatric patients and this number is not sufficient to determine whether they respond differently than adult patients.
Geriatic Use
Clinical trials of ADCETRIS did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. Safety and efficacy have not been established.
Gender
There is no FDA guidance on the use of Brentuximab vedotin with respect to specific gender populations.
Race
There is no FDA guidance on the use of Brentuximab vedotin with respect to specific racial populations.
Renal Impairment
Avoid the use of ADCETRIS in patients with severe renal impairment (CLcr <30 mL/min) [See WARNINGS AND PRECAUTIONS (5.6)].
The kidney is a route of excretion for monomethyl auristatin E (MMAE). The pharmacokinetics and safety of brentuximab vedotin and MMAE were evaluated after the administration of 1.2 mg/kg of ADCETRIS to patients with mild (CLcr >50-80 mL/min; n=4), moderate (CLcr 30-50 mL/min; n=3) and severe (CLcr <30 mL/min; n=3) renal impairment. In patients with severe renal impairment, the rate of Grade 3 or worse adverse events was 3/3 (100%) compared to 3/8 (38%) in patients with normal renal function. Additionally, the AUC of MMAE (component of ADCETRIS) was approximately 2-fold higher in patients with severe renal impairment compared to patients with normal renal function. Due to higher MMAE exposure, ≥Grade 3 adverse reactions may be more frequent in patients with severe renal impairment compared to patients with normal renal function.
Hepatic Impairment
Avoid the use of ADCETRIS in patients with moderate or severe hepatic impairment [See WARNINGS AND PRECAUTIONS (5.7)].
The liver is a route of clearance for MMAE. The pharmacokinetics and safety of brentuximab vedotin and MMAE were evaluated after the administration of 1.2 mg/kg of ADCETRIS to patients with mild (Child-Pugh A; n=1), moderate (Child-Pugh B; n=5) and severe (Child-Pugh C; n=1) hepatic impairment. In patients with moderate and severe hepatic impairment, the rate of ≥Grade 3 adverse reactions was 6/6 (100%) compared to 3/8 (38%) in patients with normal hepatic function. Additionally, the AUC of MMAE was approximately 2.2-fold higher in patients with hepatic impairment compared to patients with normal hepatic function.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Brentuximab vedotin in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Brentuximab vedotin in patients who are immunocompromised.
Administration and Monitoring
Administration
Intravenous
Monitoring
Complete blood counts should be monitored prior to each dose of ADCETRIS and more frequent monitoring should be considered for patients with Grade 3 or 4 neutropenia
IV Compatibility
There is limited information regarding IV Compatibility of Brentuximab vedotin in the drug label.
Overdosage
There is no known antidote for overdosage of ADCETRIS. In case of overdosage, the patient should be closely monitored for adverse reactions, particularly neutropenia, and supportive treatment should be administered.
Brentuximab vedotin is an ADC. The antibody is a chimeric IgG1 directed against CD30. The small molecule, MMAE, is a microtubule disrupting agent. MMAE is covalently attached to the antibody via a linker. Nonclinical data suggest that the anticancer activity of ADCETRIS is due to the binding of the ADC to CD30-expressing cells, followed by internalization of the ADC‑CD30 complex, and the release of MMAE via proteolytic cleavage. Binding of MMAE to tubulin disrupts the microtubule network within the cell, subsequently inducing cell cycle arrest and apoptotic death of the cells.
The effect of brentuximab vedotin (1.8 mg/kg) on the QTc interval was evaluated in an open-label, single-arm study in 46 evaluable patients with CD30-expressing hematologic malignancies. Administration of brentuximab vedotin did not prolong the mean QTc interval >10 ms from baseline. Small increases in the mean QTc interval (<10 ms) cannot be excluded because this study did not include a placebo arm and a positive control arm.
Pharmacokinetics
The pharmacokinetics of brentuximab vedotin were evaluated in phase 1 trials and in a population pharmacokinetic analysis of data from 314 patients. The pharmacokinetics of three analytes were determined: the ADC, MMAE, and total antibody. Total antibody had the greatest exposure and had a similar PK profile as the ADC. Hence, data on the PK of the ADC and MMAE have been summarized.
Absorption
Maximum concentrations of ADC were typically observed close to the end of infusion. A multiexponential decline in ADC serum concentrations was observed with a terminal half-life of approximately 4 to 6 days. Exposures were approximately dose proportional from 1.2 to 2.7 mg/kg. Steady-state of the ADC was achieved within 21 days with every 3-week dosing of ADCETRIS, consistent with the terminal half-life estimate.
Minimal to no accumulation of ADC was observed with multiple doses at the every 3-week schedule.
The time to maximum concentration for MMAE ranged from approximately 1 to 3 days. Similar to the ADC, steady‑state of MMAE was achieved within 21 days with every 3 week dosing of ADCETRIS. MMAE exposures decreased with continued administration of ADCETRIS with approximately 50% to 80% of the exposure of the first dose being observed at subsequent doses.
Distribution
In vitro, the binding of MMAE to human plasma proteins ranged from 68–82%. MMAE is not likely to displace or to be displaced by highly protein-bound drugs. In vitro, MMAE was a substrate of P-gp and was not a potent inhibitor of P-gp.
In humans, the mean steady state volume of distribution was approximately 6–10 L for ADC.
Metabolism
In vivo data in animals and humans suggest that only a small fraction of MMAE released from brentuximab vedotin is metabolized. In vitro data indicate that the MMAE metabolism that occurs is primarily via oxidation by CYP3A4/5. In vitro studies using human liver microsomes indicate that MMAE inhibits CYP3A4/5 but not other CYP isoforms. MMAE did not induce any major CYP450 enzymes in primary cultures of human hepatocytes.
Elimination
MMAE appeared to follow metabolite kinetics, with the elimination of MMAE appearing to be limited by its rate of release from ADC. An excretion study was undertaken in patients who received a dose of 1.8 mg/kg of ADCETRIS. Approximately 24% of the total MMAE administered as part of the ADC during an ADCETRIS infusion was recovered in both urine and feces over a 1-week period. Of the recovered MMAE, approximately 72% was recovered in the feces and the majority of the excreted MMAE was unchanged.
Specific Populations
Effects of Gender, Age, and Race: Based on the population pharmacokinetic analysis; gender, age, and race do not have a meaningful effect on the pharmacokinetics of brentuximab vedotin.
Nonclinical Toxicology
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Carcinogenicity studies with brentuximab vedotin or the small molecule (MMAE) have not been conducted.
MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
Fertility studies with brentuximab vedotin or MMAE have not been conducted. However, results of repeat-dose toxicity studies in rats indicate the potential for brentuximab vedotin to impair male reproductive function and fertility. In a 4-week repeat-dose toxicity study in rats with weekly dosing at 0.5, 5 or 10 mg/kg brentuximab vedotin, seminiferous tubule degeneration, Sertoli cell vacuolation, reduced spermatogenesis, and aspermia were observed. Effects in animals were seen mainly at 5 and 10 mg/kg of brentuximab vedotin. These doses are approximately 3 and 6-fold the human recommended dose of 1.8 mg/kg, respectively, based on body weight.
Clinical Studies
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Carcinogenicity studies with brentuximab vedotin or the small molecule (MMAE) have not been conducted.
MMAE was genotoxic in the rat bone marrow micronucleus study through an aneugenic mechanism. This effect is consistent with the pharmacological effect of MMAE as a microtubule disrupting agent. MMAE was not mutagenic in the bacterial reverse mutation assay (Ames test) or the L5178Y mouse lymphoma forward mutation assay.
Fertility studies with brentuximab vedotin or MMAE have not been conducted. However, results of repeat-dose toxicity studies in rats indicate the potential for brentuximab vedotin to impair male reproductive function and fertility. In a 4-week repeat-dose toxicity study in rats with weekly dosing at 0.5, 5 or 10 mg/kg brentuximab vedotin, seminiferous tubule degeneration, Sertoli cell vacuolation, reduced spermatogenesis, and aspermia were observed. Effects in animals were seen mainly at 5 and 10 mg/kg of brentuximab vedotin. These doses are approximately 3 and 6-fold the human recommended dose of 1.8 mg/kg, respectively, based on body weight.
This image is provided by the National Library of Medicine.
Systemic Anaplastic Large Cell Lymphoma
The efficacy of ADCETRIS in patients with relapsed sALCL was evaluated in one phase 2 open-label, single-arm, multicenter trial. This trial included patients who had sALCL that was relapsed after prior therapy. Fifty-eight patients were treated with 1.8 mg/kg of ADCETRIS administered intravenously over 30 minutes every 3 weeks. An independent review facility performed efficacy evaluations which included overall response rate (ORR = complete remission [CR] + partial remission [PR]) and duration of response as defined by clinical and radiographic measures including computed tomography (CT) and positron-emission tomography (PET) as defined in the 2007 Revised Response Criteria for Malignant Lymphoma (modified).
The 58 patients ranged in age from 14–76 years (median, 52 years) and most were male (57%) and white (83%). Patients had received a median of 2 prior therapies; 26% of patients had received prior autologous stem cell transplant. Fifty percent (50%) of patients were relapsed and 50% of patients were refractory to their most recent prior therapy. Seventy-two percent (72%) were anaplastic lymphoma kinase (ALK)-negative.
The efficacy results are summarized in TABLE 4. Duration of response is calculated from date of first response to date of progression or data cutoff date.
This image is provided by the National Library of Medicine.
How Supplied
ADCETRIS (brentuximab vedotin) for Injection is supplied as a sterile, white to off-white preservative-free lyophilized cake or powder in individually-boxed single-use vials:
NDC (51144-050-01), 50 mg brentuximab vedotin.
16.3 Special Handling
ADCETRIS is an antineoplastic product. Follow special handling and disposal procedures1.
Storage
Store vial at 2–8°C (36–46°F) in the original carton to protect from light.
Images
Drug Images
{{#ask: Page Name::Brentuximab vedotin
|?Pill Name
|?Drug Name
|?Pill Ingred
|?Pill Imprint
|?Pill Dosage
|?Pill Color
|?Pill Shape
|?Pill Size (mm)
|?Pill Scoring
|?NDC
|?Drug Author
|format=template
|template=DrugPageImages
|mainlabel=-
|sort=Pill Name
}}
Advise patients that ADCETRIS can cause a peripheral neuropathy. They should be advised to report to their health care provider any numbness or tingling of the hands or feet or any muscle weakness.
Fever/Neutropenia
Advise patients to contact their health care provider if a fever of 100.5°F or greater or other evidence of potential infection such as chills, cough, or pain on urination develops.
Infusion reactions
Advise patients to contact their health care provider if they experience signs and symptoms of infusion reactions including fever, chills, rash, or breathing problems within 24 hours of infusion.
Hepatotoxicity
Advise patients to report symptoms that may indicate liver injury, including fatigue, anorexia, right upper abdominal discomfort, dark urine, or jaundice.
Progressive multifocal leukoencephalopathy
Instruct patients receiving ADCETRIS to immediately report if they have any of the following neurological, cognitive, or behavioral signs and symptoms or if anyone close to them notices these signs and symptoms.
• changes in mood or usual behavior
• confusion, thinking problems, loss of memory
• changes in vision, speech, or walking
• decreased strength or weakness on one side of the body
Pancreatitis
Advise patients to contact their health care provider if they develop severe abdominal pain.
Pregnancy and Nursing
ADCETRIS can cause fetal harm. Advise women receiving ADCETRIS to avoid pregnancy. Advise patients to report pregnancy immediately. Advise patients to avoid nursing while receiving ADCETRIS.
Precautions with Alcohol
Alcohol-Brentuximab vedotin interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.






{kind=link}
{kind=link}