Arteriovenous fistula
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
An arteriovenous fistula is an abnormal connection or passageway between an artery and a vein. It may be congenital, surgically created for hemodialysis treatments, or acquired due to pathologic process, such as trauma or erosion of an arterial aneurysm.
Vascular Access for Hemodialysis
Patients with end stage renal failure are treated with hemodialysis. In dialysis, blood is withdrawn from an artery or vein, purified, and returned to a vein. The volume of blood is too great for veins to handle, so a vein must be enlarged. An artery and vein, usually in the arm above or below the elbow, are sewn together, to create a fistula, and arterial pressure eventually enlarges the vein. The enlarged vein can accommodate a cannula or large needle.
Pathophysiology
When an arteriovenous fistula is formed involving a major artery like the abdominal aorta, it can lead to a large decrease in peripheral resistance. This lowered peripheral resistance causes the heart to increase cardiac output in order to maintain proper blood flow to all tissues. The physical manifestations of this would be a relatively normal systolic blood pressure with a decreased diastolic blood pressure resulting in a wide (large) pulse pressure.
Normal blood flow in the brachial artery is 85 to 110 milliliters per minute (mL/min). After the creation of a fistula, the blood flow increases to 400 to 500 mL/min immediately, and 700 to 1,000 mL/min within 1 month. A bracheocephalic fistula above the elbow has a greater flow rate than a radiocephalic fistula at the wrist. Both the artery and the vein dilate and elongate in response to the greater blood flow and shear stress, but the vein dilates more and becomes "arterialized". In one study, the cephalic vein increased from 2.3 mm to 6.3 mm diameter after 2 months. When the vein is large enough to allow cannulation, the fistula is defined as "mature." [1]
Diagnosis
Doppler Echocardiography
(Images shown below are courtesy of RadsWiki)
-
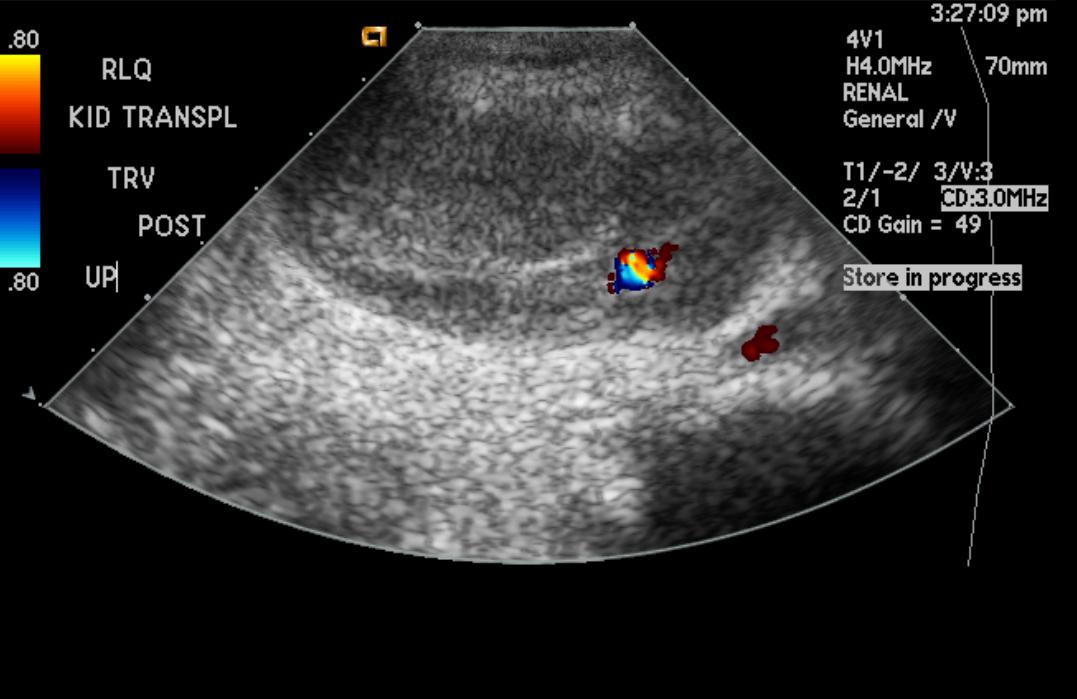
Renal arteriovenous fistula
-
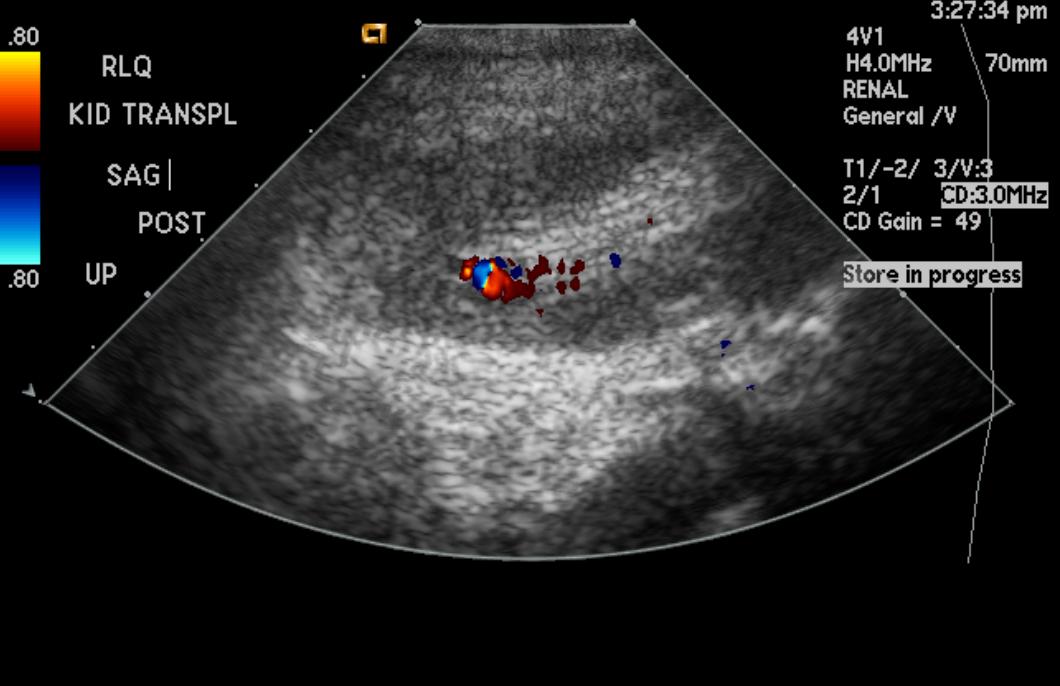
Renal arteriovenous fistula
-
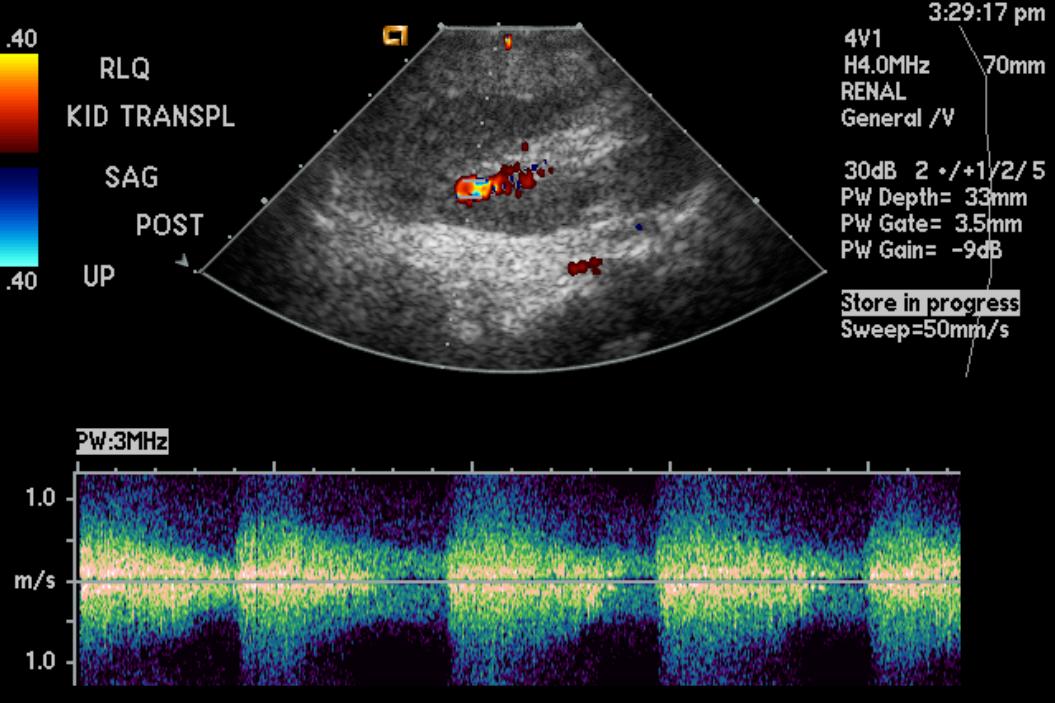
Renal arteriovenous fistula



Treatment
Congenital fistulas, if small, usually do not need treatment. Acquired fistulas can be treated by surgery.
Contraindicated medications
Compensatory hypertension due to Arteriovenous fistula is considered an absolute contraindication to the use of the following medications:
Related Chapters
External Links
{{#ev:youtube|hIw3IKB7LIs}}
{{#ev:youtube|If7lZCIpZgU}}
2008 ACC/AHA Guidelines for the Management of Adults With Congenital Heart Disease (DO NOT EDIT)[2]
Coronary Arteriovenous Fistula (DO NOT EDIT)[2]
| Class I |
| "1. If a continuous murmur is present, its origin should be defined either by echocardiography, MRI, CT angiography, or cardiac catheterization. (Level of Evidence: C)" |
| ”2. A large coronary arteriovenous fistula (CAVF), regardless of symptomatology, should be closed via either a transcatheter or surgical route after delineation of its course and its potential to fully obliterate the fistula. (Level of Evidence: C)" |
| ”3. A small to moderate CAVF in the presence of documented myocardial ischemia, arrhythmia, otherwise unexplained ventricular systolic or diastolic dysfunction or enlargement, or endarteritis should be closed via either a transcatheter or surgical approach after delineation of its course and its potential to fully obliterate the fistula. (Level of Evidence: C)" |
| Class III |
| "1. Patients with small, asymptomatic CAVF should not undergo closure of CAVF. (Level of Evidence: C)" |
| Class IIa |
| "1. Clinical follow-up with echocardiography every 3 to 5 years can be useful for patients with small, asymptomatic CAVF to exclude development of symptoms or arrhythmias or progression of size or chamber enlargement that might alter management. (Level of Evidence: C)" |
Management Strategies for CAVF(DO NOT EDIT)[2]
| Class I |
| "1. Surgeons with training and expertise in CHD should perform operations for management of patients with CAVF. (Level of Evidence: C)" |
| ”2. Transcatheter closure of CAVF should be performed only in centers with expertise in such procedures. (Level of Evidence: C)" |
| ”3. Transcatheter delineation of CAVF course and access to distal drainage should be performed in all patients with audible continuous murmur and recognition of CAVF. (Level of Evidence: C)" |
References
- ↑ Vascular, Vol. 14, Supl. 1, Nov. 2006, p. S1
- ↑ 2.0 2.1 2.2 Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM, Dearani JA; et al. (2008). "ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons". J Am Coll Cardiol. 52 (23): e1–121. doi:10.1016/j.jacc.2008.10.001. PMID 19038677.