WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Aminophylline is a bronchodilator that is FDA approved for the {{{indicationType}}} of adjunct to inhaled beta-2 selective agonists and systemically administered corticosteroids for the treatment of acute exacerbations of the symptoms and reversible airflow obstruction associated with asthma and other chronic lung diseases, e.g., emphysema and chronic bronchitis. Common adverse reactions include severe allergic reactions of the skin, including exfoliative dermatitis.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Intravenous theophylline is indicated as an adjunct to inhaled beta-2 selective agonists and systemically administered corticosteroids for the treatment of acute exacerbations of the symptoms and reversible airflow obstruction associated with asthma and other chronic lung diseases, e.g., emphysema and chronic bronchitis.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Aminophylline in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Aminophylline in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Aminophylline in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Aminophylline in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Aminophylline in pediatric patients.
Contraindications
Aminophylline is contraindicated in patients with a history of hypersensitivity to theophylline or other components in the product including ethylenediamine
Warnings
Concurrent Illness
Theophylline should be used with extreme caution in patients with the following clinical conditions due to the increased risk of exacerbation of the concurrent condition:
Active peptic ulcer disease
Seizure disorders
Cardiac arrhythmias (not including bradyarrhythmias)
Conditions That Reduce Theophylline Clearance
There are several readily identifiable causes of reduced theophylline clearance. If the infusion rate is not appropriately reduced in the presence of these risk factors, severe and potentially fatal theophylline toxicity can occur. Careful consideration must be given to the benefits and risks of theophylline use and the need for more intensive monitoring of serum theophylline concentrations in patients with the following risk factors:
Age
Neonates (term and premature)
Children <1 year
Elderly (>60 years)
Concurrent Diseases
Acute pulmonary edema
Congestive heart failure
Cor pulmonale
Fever; ≥102° for 24 hours or more; or lesser temperature elevations for longer periods
Hypothyroidism
Liver disease; cirrhosis, acute hepatitis
Reduced renal function in infants <3 months of age
Sepsis with multi-organ failure
Shock
Cessation of Smoking
Adverse Reactions
Clinical Trials Experience
There is limited information regarding clinical trial experience of Aminophylline in the drug label.
Postmarketing Experience
Adverse reactions associated with theophylline are generally mild when peak serum theophylline concentrations are <20 mcg/mL and mainly consist of transient caffeine-like adverse effects such as nausea, vomiting, headache, and insomnia.
When peak serum theophylline concentrations exceed 20 mcg/mL, however, theophylline produces a wide range of adverse reactions including persistent vomiting, cardiac arrhythmias, and intractable seizures which can be lethal.
Other adverse reactions that have been reported at serum theophylline concentrations <20 mcg/mL include diarrhea, irritability, restlessness, fine skeletal muscle tremors, and transient diuresis. In patients with hypoxia secondary to COPD, multifocal atrial tachycardia and flutter have been reported at serum theophylline concentrations ≥15 mcg/mL. There have been a few isolated reports of seizures at serum theophylline concentrations <20 mcg/mL in patients with an underlying neurological disease or in elderly patients.
The occurrence of seizures in elderly patients with serum theophylline concentrations <20 mcg/mL may be secondary to decreased protein binding resulting in a larger proportion of the total serum theophylline concentration in the pharmacologically active unbound form. The clinical characteristics of the seizures reported in patients with serum theophylline concentrations <20 mcg/mL have generally been milder than seizures associated with excessive serum theophylline concentrations resulting from an overdose (i.e., they have generally been transient, often stopped without anticonvulsant therapy, and did not result in neurological residua).
Products containing aminophylline may rarely produce severe allergic reactions of the skin, including exfoliative dermatitis, after systemic administration in a patient who has been previously sensitized by topical application of a substance containing ethylenediamine. In such patients skin patch tests are positive for ethylenediamine, a component of aminophylline, and negative for theophylline.
Pharmacists and other individuals who experience repeated skin exposure while physically handling aminophylline may develop a contact dermatitis due to the ethylenediamine component.
This image is provided by the National Library of Medicine.
Drug Interactions
Adding a drug that inhibits theophylline metabolism (e.g., cimetidine, erythromycin, tacrine) or stopping a concurrently administered drug that enhances theophylline metabolism (e.g., carbamazepine, rifampin).
When Signs or Symptoms of Theophylline Toxicity Are Present:
Whenever a patient receiving theophylline develops nausea or vomiting, particularly repetitive vomiting, or other signs or symptoms consistent with theophylline toxicity (even if another cause may be suspected), the intravenous infusion should be stopped and a serum theophylline concentration measured immediately.
Dosage Increases
Increases in the dose of intravenous theophylline should not be made in response to an acute exacerbation of symptoms unless the steady-state serum theophylline concentration is <10 mcg/mL.
As the rate of theophylline clearance may be dose-dependent (i.e., steady-state serum concentrations may increase disproportionately to the increase in dose), an increase in dose based upon a sub-therapeutic serum concentration measurement should be conservative. In general, limiting infusion rate increases to about 25% of the previous infusion rate will reduce the risk of unintended excessive increases in serum theophylline concentration.
There are no adequate and well controlled studies in pregnant women. Additionally, there are no teratogenicity studies in nonrodents (e.g., rabbits). Theophylline was not shown to be teratogenic in CD-1 mice at oral doses up to 400 mg/kg, approximately 2.0 times the human dose on a mg/m2 basis or in CD-1 rats at oral doses up to 260 mg/kg, approximately 3.0 times the recommended human dose on a mg/m2 basis. At a dose of 220 mg/kg, embryotoxicity was observed in rats in the absence of maternal toxicity.
Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Aminophylline in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Aminophylline during labor and delivery.
Nursing Mothers
Theophylline is excreted into breast milk and may cause irritability or other signs of mild toxicity in nursing human infants. The concentration of theophylline in breast milk is about equivalent to the maternal serum concentration. An infant ingesting a liter of breast milk containing 10 ‑ 20 mcg/mL of theophylline per day is likely to receive 10 - 20 mg of theophylline per day. Serious adverse effects in the infant are unlikely unless the mother has toxic serum theophylline concentrations.
Pediatric Use
The clearance of theophylline is very low in neonates. Theophylline clearance reaches maximal values by one year of age, remains relatively constant until about 9 years of age and then slowly decreases by approximately 50% to adult values at about age 16. Renal excretion of unchanged theophylline in neonates amounts to about 50% of the dose, compared to about 10% in children older than three months and in adults. Careful attention to dosage selection and monitoring of serum theophylline concentrations are required in children.
Geriatic Use
The clearance of theophylline is decreased by an average of 30% in healthy elderly adults (>60 yrs.) compared to healthy young adults. Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in elderly patients
Gender
Gender differences in theophylline clearance are relatively small and unlikely to be of clinical significance. Significant reduction in theophylline clearance, however, has been reported in women on the 20th day of the menstrual cycle and during the third trimester of pregnancy.
Race
Pharmacokinetic differences in theophylline clearance due to race have not been studied.
Renal Impairment
Only a small fraction, e.g., about 10%, of the administered theophylline dose is excreted unchanged in the urine of children greater than three months of age and adults.
Since little theophylline is excreted unchanged in the urine and since active metabolites of theophylline (i.e., caffeine, 3-methylxanthine) do not accumulate to clinically significant levels even in the face of end-stage renal disease, no dosage adjustment for renal insufficiency is necessary in adults and children >3 months of age. In contrast, approximately 50% of the administered theophylline dose is excreted unchanged in the urine in neonates. Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in neonates with decreased renal function
Hepatic Impairment
Theophylline clearance is decreased by 50% or more in patients with hepatic insufficiency (e.g., cirrhosis, acute hepatitis, cholestasis). Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with reduced hepatic function.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Aminophylline in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Aminophylline in patients who are immunocompromised.
Miscellaneous
Congestive Heart Failure (CHF) Theophylline clearance is decreased by 50% or more in patients with CHF. The extent of reduction in theophylline clearance in patients with CHF appears to be directly correlated to the severity of the cardiac disease. Since theophylline clearance is independent of liver blood flow, the reduction in clearance appears to be due to impaired hepatocyte function rather than reduced perfusion. Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with CHF.
Smokers Tobacco and marijuana smoking appears to increase the clearance of theophylline by induction of metabolic pathways. Theophylline clearance has been shown to increase by approximately 50% in young adult tobacco smokers and by approximately 80% in elderly tobacco smokers compared to nonsmoking subjects. Passive smoke exposure has also been shown to increase theophylline clearance by up to 50%. Abstinence from tobacco smoking for one week causes a reduction of approximately 40% in theophylline clearance. Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients who stop smoking (see WARNINGS). Use of nicotine gum has been shown to have no effect on theophylline clearance.
Fever, regardless of its underlying cause, can decrease the clearance of theophylline. The magnitude and duration of the fever appear to be directly correlated to the degree of decrease of theophylline clearance. Precise data are lacking, but a temperature of 39°C (102°F) for at least 24 hours is probably required to produce a clinically significant increase in serum theophylline concentrations. Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with sustained fever.
Other factors associated with decreased theophylline clearance include the third trimester of pregnancy, sepsis with multiple organ failure, and hypothyroidism. Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with any of these conditions (see WARNINGS). Other factors associated with increased theophylline clearance include hyperthyroidism and cystic fibrosis.
Administration and Monitoring
Administration
Intravenous
Monitoring
Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in elderly patients
The large fraction of the theophylline dose excreted in the urine as unchanged theophylline and caffeine in neonates requires careful attention to dose reduction and frequent monitoring of serum theophylline concentrations in neonates with reduced renal function.
Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with reduced hepatic function.
Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with CHF.
Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients who stop smoking.
Careful attention to dose reduction and frequent monitoring of serum theophylline concentrations are required in patients with sustained fever
Serum theophylline concentration measurements are readily available and should be used to determine whether the dosage is appropriate. Specifically, the serum theophylline concentration should be measured as follows:
Before making a dose increase to determine whether the serum concentration is sub-therapeutic in a patient who continues to be symptomatic.
Whenever signs or symptoms of theophylline toxicity are present.
Whenever there is a new illness, worsening of an existing concurrent illness or a change in the patient’s treatment regimen that may alter theophylline clearance (e.g., fever >102°F sustained for ≥24 hours, hepatitis, or drugs listed in Table II are added or discontinued).
In patients who have received no theophylline in the previous 24 hours, a serum concentration should be measured 30 minutes after completion of the intravenous loading dose to determine whether the serum concentration is <10 mcg/mL indicating the need for an additional loading dose or >20 mcg/mL indicating the need to delay starting the constant I.V. infusion. Once the infusion is begun, a second measurement should be obtained after one expected half-life (e.g., approximately 4 hours in children 1 to 9 years and 8 hours in non-smoking adults; See Table I for the expected half-life in additional patient populations). The second measurement should be compared to the first to determine the direction in which the serum concentration has changed. The infusion rate can then be adjusted before steady state is reached in an attempt to prevent an excessive or sub-therapeutic theophylline concentration from being achieved.
If a patient has received theophylline in the previous 24 hours, the serum concentration should be measured before administering an intravenous loading dose to make sure that it is safe to do so. If a loading dose is not indicated (i.e., the serum theophylline concentration is ≥10 mcg/mL), a second measurement should be obtained as above at the appropriate time after starting the intravenous infusion. If, on the other hand, a loading dose is indicated, a second blood sample should be obtained after the loading dose and a third sample should be obtained one expected half-life after starting the constant infusion to determine the direction in which the serum concentration has changed.
Once the above procedures related to initiation of intravenous theophylline infusion have been completed, subsequent serum samples for determination of theophylline concentration should be obtained at 24-hour intervals for the duration of the infusion. The theophylline infusion rate should be increased or decreased as appropriate based on the serum theophylline levels.
When signs or symptoms of theophylline toxicity are present, the intravenous infusion should be stopped and a serum sample for theophylline concentration should be obtained as soon as possible, analyzed immediately, and the result reported to the clinician without delay. In patients in whom decreased serum protein binding is suspected (e.g., cirrhosis, women during the third trimester of pregnancy), the concentration of unbound theophylline should be measured and the dosage adjusted to achieve an unbound concentration of 6-12 mcg/mL.
Saliva concentrations of theophylline cannot be used reliably to adjust dosage without special techniques.
Electrocardiographic monitoring should be initiated on presentation and continued until the serum theophylline level has returned to a nontoxic level. Serum electrolytes and glucose should be measured on presentation and at appropriate intervals indicated by clinical circumstances. Fluid and electrolyte abnormalities should be promptly corrected. Monitoring and treatment should be continued until the serum concentration decreases below 20 mcg/mL.
IV Compatibility
There is limited information regarding IV Compatibility of Aminophylline in the drug label.
Overdosage
Acute Overdose
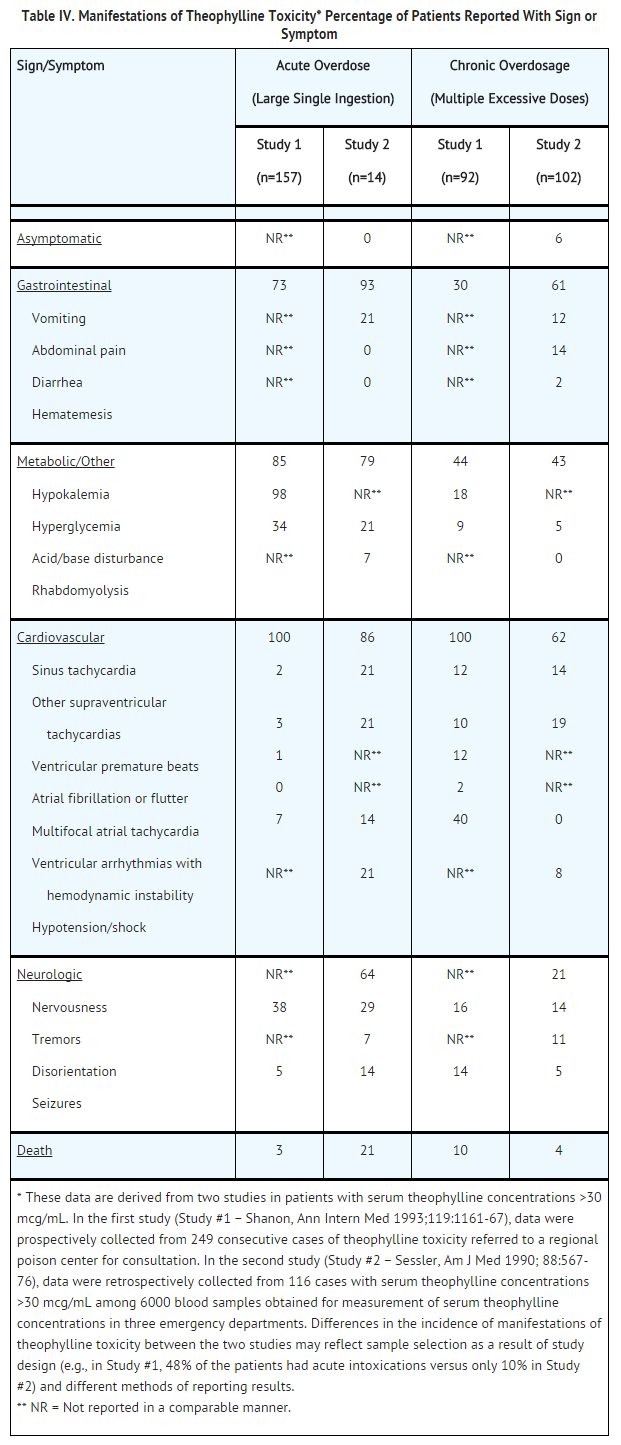
Signs and Symptoms
Description
Management
Description
Chronic Overdose
There is limited information regarding Chronic Overdose of Aminophylline in the drug label.
Pharmacology
There is limited information regarding Aminophylline Pharmacology in the drug label.

{kind=link}