Pulmonary edema chest x ray: Difference between revisions
No edit summary |
|||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{CMG}} | {{CMG}} | ||
Revision as of 20:40, 5 September 2011
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The chest x-ray is the diagnostic modality of choice in the evaluation of the patient with suspected pulmonary edema. Chest x-ray findings include:
- Kerley B lines or thickening of the interlobular septa
- Peribronchial cuffing
- Thickening of the fissures
- Increased vascular markings
- Pleural effusions.
Cardiogenic Versus Noncardiogenic Pulmonary Edema
Cardiogenic pulmonary edema can be distinguished from noncardiogenic pulmonary edema by the presence of redistribution of blood flow to the upper lobes (increased blood flow to the higher parts of the lung). In contrast, patchy alveolar infiltrates with air bronchograms are more indicative of noncardiogenic edema.
Correlation of Chest X-Ray Findings with Pulmonary Capillary Wedge Pressure
- Normal:5-10 mm Hg
- Cephalization: 10-15 mm Hg
- Kerley B Lines: 15-20 mm Hg
- Pulmonary Interstitial Edema: 20-25 mm Hg
- Pulmonary Alveolar Edema: > 25 mm Hg
Peribronchial Cuffing

Peribronchial cuffing is an abnormality on a chest x-ray whereby the usually thin bronchial walls are thickened and take on a doughnut-like appearance.
Kerley B Lines
Kerley B lines are short parallel lines at the lung periphery. These lines represent distended interlobular septa, which are usually less than 1 cm in length and parallel to one another at right angles to the pleura. They are located peripherally in contact with the pleura, but are generally absent along fissural surfaces. They may be seen in any zone but are most frequently observed at the lung bases at the costophrenic angles on the PA radiograph, and in the substernal region on lateral radiographs.
-
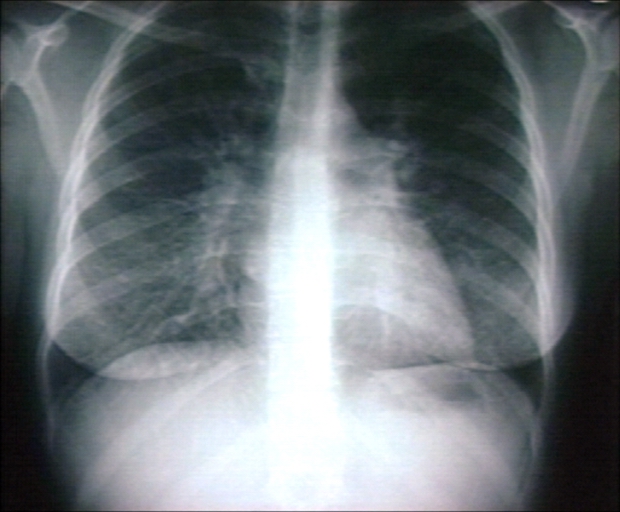
Plain film: Mitral stenosis, Kerley B lines
-
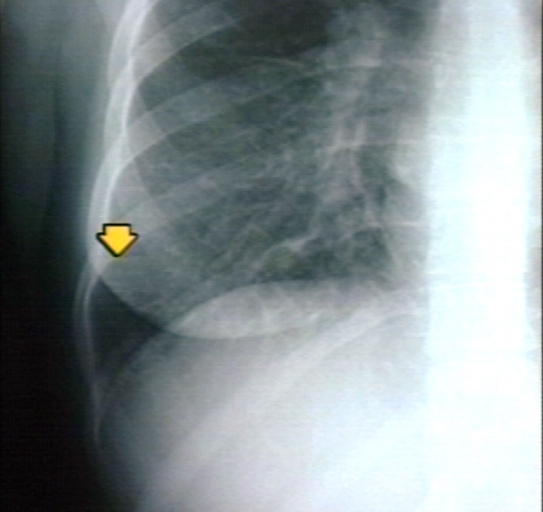
Plain film: Mitral stenosis, Kerley B lines
-

Plain film: Mitral stenosis, Kerley B lines


