Renal infarct: Difference between revisions
No edit summary |
No edit summary |
||
| Line 1: | Line 1: | ||
{{Search infobox}} | {{Search infobox}} | ||
{{ | {{CMG}} | ||
==Risk factors== | ==Risk factors== | ||
*[[Coagulopathy]] | *[[Coagulopathy]] | ||
*[[Cocaine]] | *[[Cocaine]] | ||
| Line 14: | Line 12: | ||
*[[Stent]] placement | *[[Stent]] placement | ||
*[[Trauma]] | *[[Trauma]] | ||
==Diagnosis== | ==Diagnosis== | ||
Revision as of 21:51, 31 July 2012
Template:Search infobox Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Risk factors
- Coagulopathy
- Cocaine
- Ehlers-Danlos syndrome
- Fibromuscular dysplasia
- Marfan syndrome
- Renal transplant
- Stent placement
- Trauma
Diagnosis
History and Symptoms
The patient may compain of persistent flank pain, low back pain or even abdominal pain.
There is usually a history of thormboembolic risk factors (cancer) or a prior history of embolization. Atherosclerotic risk factors are often present.
Laboratory Findings
Urinalysis
Hematuria is present in 74% of cases
Blood
Elevated LDH is sensitive but non-specific for renal infarction.
Imaging Studies
The diagnostic study of choice is a contrast CT. Ultrasound can evaluate if obstructive uropathy is present as a cause of back pain and renal insufficiency, but it lacks senstitivity in the detection of renal infarction.
-
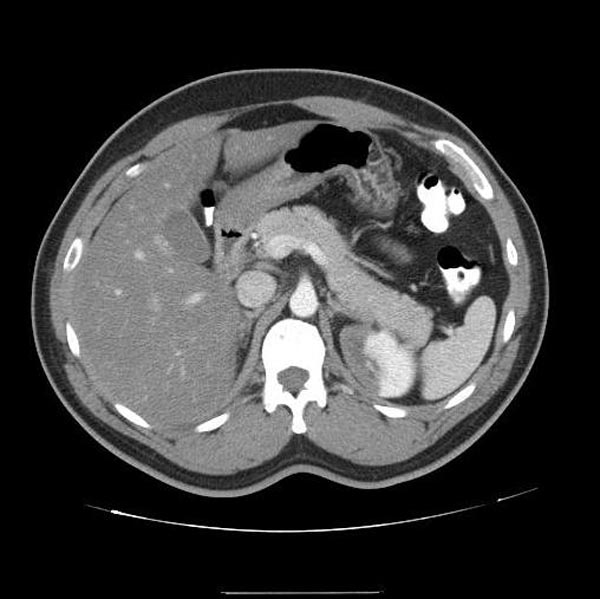
CT demonstrates a left renal infarction patient#1 Image courtesy of RadsWiki and copylefted
-

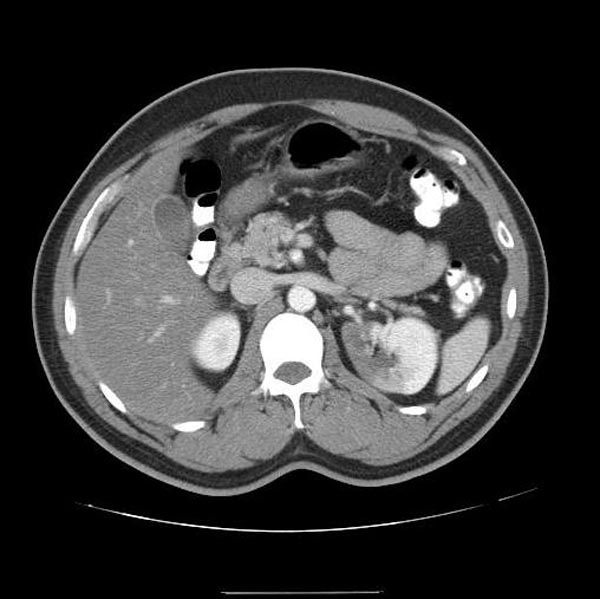
CT demonstrates a left renal infarction patient#1 Image courtesy of RadsWiki and copylefted
-
CT demonstrates a left renal infarction patient#1 Image courtesy of RadsWiki and copylefted



-

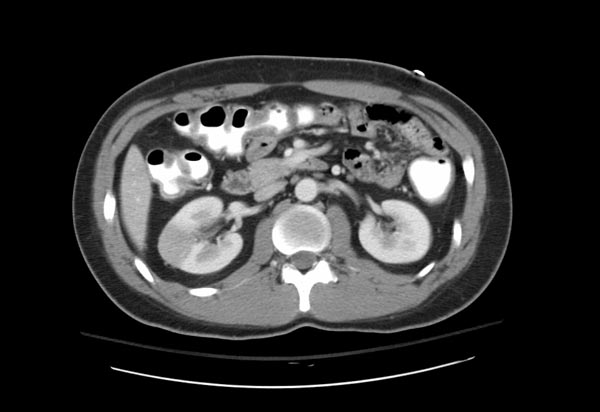
CT demonstrates a right renal infarction patient#2 Image courtesy of RadsWiki and copylefted
-

CT demonstrates a right renal infarction patient#2 Image courtesy of RadsWiki and copylefted
-
CT demonstrates a right renal infarction patient#2 Image courtesy of RadsWiki and copylefted



Treatment
Prompt recognition is critical so that thrombolysis, anticoagulation, or embolectomy can be undertaken to minimize the loss in renal function. It should be noted that these patients are at high risk of recurrent thromboembolism, and long-term anticoagulation may be of benefit.