Gallbladder
|
WikiDoc Resources for Gallbladder |
|
Articles |
|---|
|
Most recent articles on Gallbladder Most cited articles on Gallbladder |
|
Media |
|
Powerpoint slides on Gallbladder |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Gallbladder at Clinical Trials.gov Clinical Trials on Gallbladder at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Gallbladder
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Gallbladder Discussion groups on Gallbladder Patient Handouts on Gallbladder Directions to Hospitals Treating Gallbladder Risk calculators and risk factors for Gallbladder
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Gallbladder |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The gallbladder (or cholecyst, sometimes gall bladder) is a pear-shaped organ that stores about 50 ml of bile (or "gall") until the body needs it for digestion.
Anatomy
The gallbladder is about 100 to 120 mm long in humans and appears dark green because of its contents (bile), rather than its tissue. It is connected to the liver and the duodenum by the biliary tract.
- The cystic duct connects the gallbladder to the common hepatic duct to form the common bile duct.
- The common bile duct then joins the pancreatic duct, and enters through the hepatopancreatic ampulla at the major duodenal papilla.[1][2]
- The fundus of the gallbladder is the part farthest from the duct, located by the lower border of the liver [3]. It's at the same level as the transpyloric plane.
Microscopic anatomy
The different layers of the gallbladder are as follows:
- The gallbladder has a simple columnar epithelial lining characterized by recesses called Aschoff's recesses, which are pouches inside the lining.
- Under the epithelium there is a layer of connective tissue (lamina propria).
- Beneath the connective tissue is a wall of smooth muscle (muscularis externa) that contracts in response to cholecystokinin, a peptide hormone secreted by the duodenum.
- There is essentially no submucosa separating the connective tissue from serosa and adventitia.
Section References[4]
Function
The gallbladder stores about 50 ml (1.7 US fluid ounces / 1.8 Imperial fluid ounces) of bile, which is released when food containing fat enters the digestive tract, stimulating the secretion of cholecystokinin (CCK). The bile, produced in the liver, emulsifies fats and neutralizes acids in partly digested food.
After being stored in the gallbladder the bile becomes more concentrated than when it left the liver, increasing its potency and intensifying its effect on fats. Most digestion occurs in the duodenum.
Role in disease

- Cholestasis is the blockage in the supply of bile into the digestive tract. It can be "intrahepatic" (the obstruction is in the liver) or "extrahepatic" (outside the liver). It can lead to jaundice, and is identified by the presence of elevated bilirubin level that is mainly conjugated.
- Biliary colic is when a gallstone blocks either the common bile duct or the duct leading into it from the gallbladder.
- Up to 25% of all people have gallstones (cholelithiasis), composed of lecithin and bile acids. These can cause abdominal pain, usually in relation with a meal, as the gallbladder contracts and gallstones pass through the bile duct.
- Acute or chronic inflammation of the gallbladder (cholecystitis) causes abdominal pain. 90% of cases of acute cholecystitis are caused by the presence of gallstones. The actual inflammation is due to secondary infection with bacteria of an obstructed gallbladder, with the obstruction caused by the gallstone.
- When gallstones obstruct the common bile duct (choledocholithiasis), the patient develops jaundice and liver cell damage. It can be a medical emergency, requiring endoscopic or surgical treatment such as a cholecystectomy. Most gallstones are eventually passed naturally, though the passing is typically quite painful.
- A rare clinical entity is ileus (bowel) obstruction by a large gallstone, or gallstone ileus. This condition develops in patients with longstanding gallstone disease, in which the gallbladder forms a fistula with the digestive tract. Large stones pass into the bowel, and generally block the gut at the level of Treitz' ligament or the ileocecal valve, two narrow points in the digestive tract. The treatment is surgical.
- Cancer of the gallbladder is a rare but highly fatal disease. It has been associated with gallstone disease, estrogens, cigarette smoking, alcohol consumption and obesity. Despite aggressive modern surgical approaches, advanced imaging techniques, and endoscopy, nearly 90% of patients die from advanced stages of the disease and experience pain, jaundice, weight loss, and ascites.
- Polyps (growths) are sometimes detected during diagnostic tests for gallbladder disease. Small gallbladder polyps (up to 10 mm) pose little or no risk, but large ones (greater than 15 mm) pose some risk for cancer, so the gallbladder should be removed. Patients with polyps 10 mm to 15 mm have a lower risk but they should still discuss removal of their gallbladder with their physician. Of special note is a condition called primary sclerosing cholangitis, which causes inflammation and scarring in the bile duct. It is associated with a lifetime risk of 7% to 12% for gallbladder cancer. The cause is unknown, although primary sclerosing cholangitis tends to strike younger men who have ulcerative colitis. Polyps are often detected in this condition and have a very high likelihood of malignancy.
Additional images
-
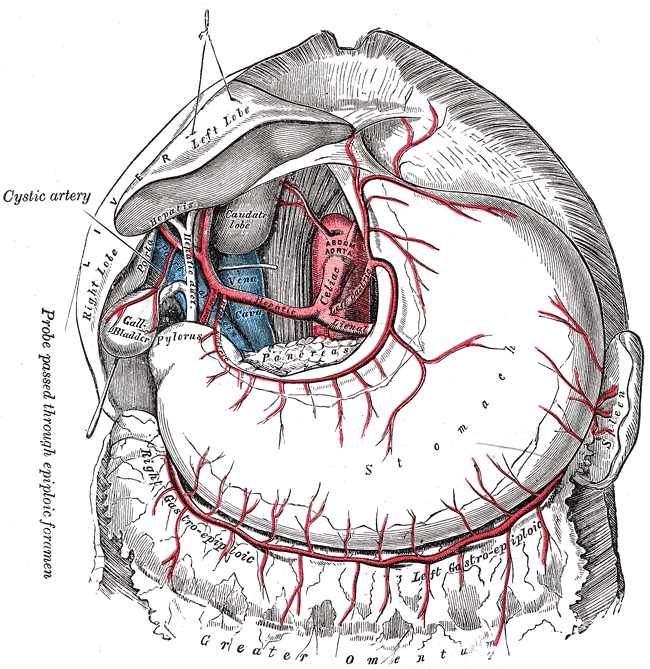 The celiac artery and its branches.
The celiac artery and its branches. -
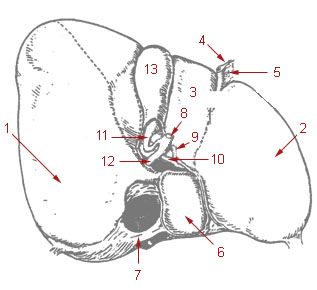
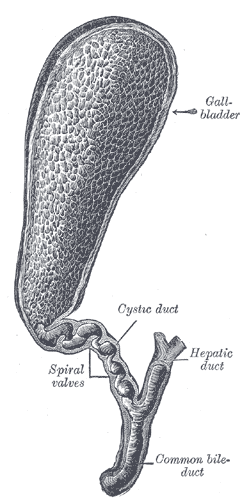 Gall bladder
Gall bladder -
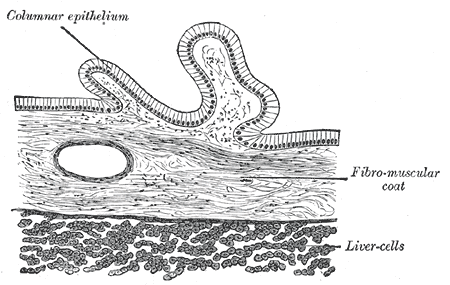 Transverse section of gall-bladder.
Transverse section of gall-bladder.



-
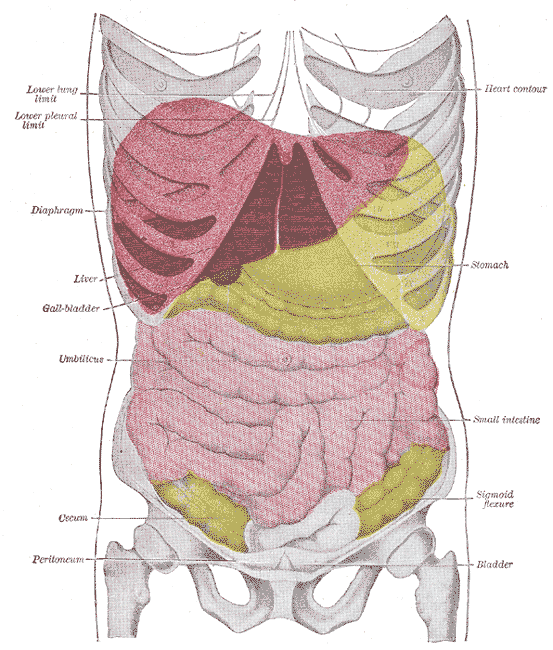 Topography of thoracic and abdominal viscera.
Topography of thoracic and abdominal viscera. -
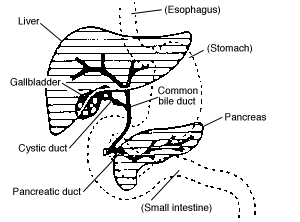 Digestive system diagram showing the bile duct
Digestive system diagram showing the bile duct -
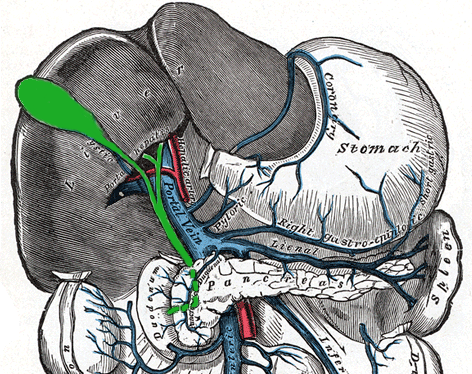 The portal vein and its tributaries.
The portal vein and its tributaries.



-
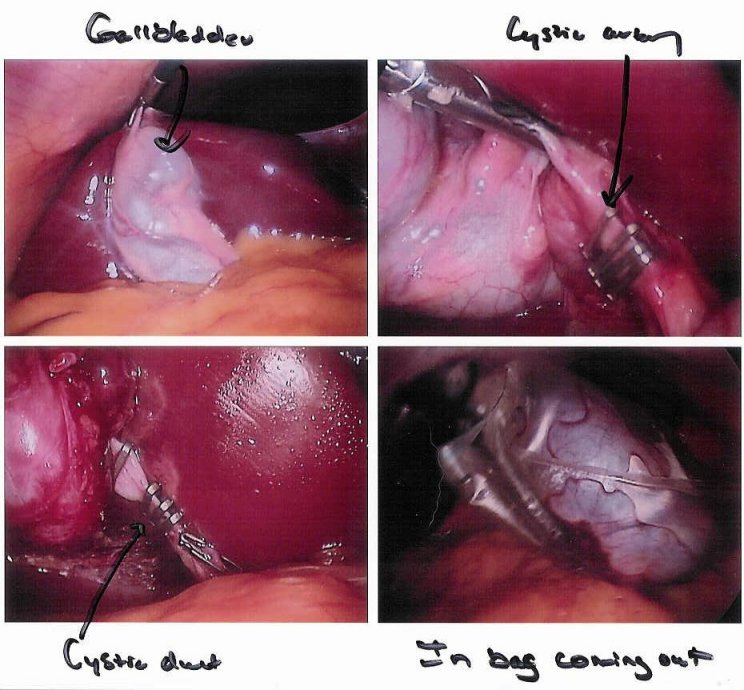 Cholecystectomy seen through a laparoscope
Cholecystectomy seen through a laparoscope -


References
- ↑ "Laboratory 38. Stomach, Spleen and Liver, Step 14. The Gallbladder and the Bile System". Human Anatomy (Laboratory Dissections). SUNY Downstate Medical Center, Brooklyn, NY. 2003-11-17. Retrieved 2007-06-29.
- ↑ "Abdominal dissection, gall bladder position emphasized" (JPG). Human Anatomy (Laboratory Dissections). SUNY Downstate Medical Center, Brooklyn, NY. 2003-11-17. Retrieved 2007-06-29.
- ↑ medical-dictionary.thefreedictionary.com - fundus of gallbladder
- ↑ "Slide 5: Gall Bladder". JayDoc HistoWeb. University of Kansas. Retrieved 2007-06-29.
{kind=link}
See also
External links
Template:Digestive glands
Template:Gastroenterology
cs:Žlučník cy:Coden fustl de:Gallenblase dv:ފިތް el:Χοληδόχος κύστη eu:Behazun xixku hr:Žuč id:Kantung empedu is:Gallblaðra it:Cistifellea he:כיס המרה la:Vesica biliaris lt:Tulžies pūslė hu:Epehólyag mt:Marrara ms:Pundi hempedu nl:Galblaas no:Galleblæren ps:تريخی simple:Gallbladder sk:Žlčník sl:Žolčnik su:Hampru fi:Sappirakko sv:Gallblåsa te:పిత్తాశయం th:ถุงน้ำดี