Romano-Ward syndrome: Difference between revisions
| Line 123: | Line 123: | ||
* Common [[complications]] of Romano-Ward syndrome include: | * Common [[complications]] of Romano-Ward syndrome include: | ||
** [[Cardiac arrhythmias]] | **[[Cardiac arrhythmias]] | ||
** [[Seizures]] | **[[Cardiac arrest]] | ||
** [[Sudden cardiac death]] | **[[Seizures]] | ||
**[[Sudden cardiac death]] | |||
=== Prognosis === | === Prognosis === | ||
| Line 151: | Line 152: | ||
*[[Presyncope]] | *[[Presyncope]] | ||
*[[Syncope]] | *[[Syncope]] | ||
*[[Palpitation|Palpitations]] | *[[Palpitation|Palpitations]]: All the first three symptoms are normally self limiting and may reoccur most of the time | ||
*[[Tachycardia]] | *[[Tachycardia]] | ||
*[[Ventricular arrhythmias|Ventricular arrhythmia]] | *[[Ventricular arrhythmias|Ventricular arrhythmia]] | ||
| Line 177: | Line 178: | ||
** [[Ventricular fibrillation]] | ** [[Ventricular fibrillation]] | ||
* Stress [[The electrocardiogram|ECG]] or a [[Treadmill test|treadmill]] [[The electrocardiogram|ECG]] | * Stress [[The electrocardiogram|ECG]] or a [[Treadmill test|treadmill]] [[The electrocardiogram|ECG]] testing also may be helpful in the [[diagnosis]] of Romano-Ward syndrome | ||
==Causes== | ==Causes== | ||
Revision as of 14:54, 2 January 2020
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief:
Synonyms and keywords: Autosomal Dominant Long QT syndrome, Long QT syndrome without deafness, LQTS, Romano-Ward Long QT syndrome, RWS, Ward-Romano syndrome, Romano-Ward syndrome
Overview
Romano-Ward syndrome is a rare congenital genetic condition with autosomal dominant inheritance pattern which leads to abnormal ventricular myocardial repolarization which results in long QT syndrome (LQTS). Among all other long QT syndrome (LQTS) Romano-Ward syndrome is the most common one. Romano-Ward syndrome is due to mutation in LQT1, LQT2 and LQT3 genes. Romano-Ward syndrome has a purely cardiac phenotype of QT prolongation in contrast to Jervell and Lange-Nielsen syndrome which has both sensorineural deafness and cardiac events.
Historical Perspective
- In 1963, Romano and in 1964, Ward was the first to discover almost similar condition like Jervell and Lange-Nielsen syndrome and they named it as Romano-Ward syndrome.[1][2][3][4][5][6][7]
- In 1990, LQTS 1, LQTS 2 and LQTS 3 the three main types of LQTS and their genes involved and proteins involved are identified for the first time.
Classification
| LQT | Gene Involved | Chromosome involved | Protein Involved | Ion channel Involved |
|---|---|---|---|---|
| LQT 1 | KCNQ1 | 11p15.5 | Iks a subunit | Iks |
| LQT 2 | HERG | 7q35-36 | Ikr a subunit | Ikr |
| LQT 3 | SCN5A | 3q21-24 | Sodium channel | INa |
| LQT 4 | NOT KNOWN | 4q25-27 | Unknown | Unknown |
| LQT 5 | KCNE1 | 21q22.1-2 | Iks a subunit | Iks |
| LQT 6 | KCNE2 | 21q22.1 | Ikr b subunit | Ikr |
Pathophysiology
- Mutations in the ANK2, KCNE1, KCNE2, KCNH2, KCNQ1, and SCN5A genes cause Romano-Ward syndrome
- The proteins made by most of these genes form channels that transport positively-charged ions, such as potassium and sodium, in and out of cells
- In cardiac muscle, these potassium and sodium ion channels play critical roles in maintaining the heart's normal rhythm
- Mutations in any of these genes alter the structure or function of channels, which changes the flow of ions between cells and results in abnormal heart rhythm
- A disruption in ion transport alters the way the heartbeats, leading to the abnormal heart rhythm characteristic of Romano-Ward syndrome
- Unlike most genes involved in Romano-Ward syndrome, the ANK2 gene does not produce an ion channel but instead the protein made by the ANK2 gene ensures that other proteins, particularly ion channels, are inserted into the cell membrane appropriately
- Then the truncated protein results in impairing potassium channel function, which is known to result in long QT syndrome.
Causes
Genetic Causes
- Romano-Ward syndrome is caused by a mutation in the ANK2, KCNE1, KCNE2, KCNH2, KCNQ1, and SCN5A genes.
Differentiating Romano-Ward syndrome from other Diseases
Romano-Ward syndrome must be differentiated from Jervell and Lange-Nielsen syndrome (JLNS), Timothy syndrome, Andersen-Tawil syndrome, Brugada syndrome, and Sudden infant death syndrome (SIDS).[10][11][12][13][14][15][16]
Epidemiology and Demographics
Incidence
- The incidence of Romano-Ward syndrome is approximately 1 in 2,000 people worldwide individuals worldwide.
Prevalence
- The prevalence of Romano-Ward syndrome is approximately 1:20 000 to 1:5000 individuals worldwide.[17]
- The prevalence of Romano-Ward syndrome is approximately 1 in 2000 live births.
Race
- There is no racial predilection to Romano-Ward syndrome.
Gender
- Romano-Ward syndrome affects men and women equally.
Risk Factors
- Apart from the genetic mutations in ANK2, KCNE1, KCNE2, KCNH2, KCNQ1, and SCN5A genes, there are no other risk factors associated with Romano-Ward syndrome.
- Other common risk factors in the development of Romano-Ward syndrome symptoms include sudden sleep arousal, exercise and intense or sudden emotion which include the following:[18][19]
- Competitive sports
- Amusement park rides
- Frightening movies
- Jumping into cold water
Screening
There is insufficient evidence to recommend routine screening for Romano-Ward syndrome.
Natural History, Complications and Prognosis
Natural History
- The symptoms of (disease name) usually develop in the first/ second/ third decade of life, and start with symptoms such as ___.
- The symptoms of (disease name) typically develop ___ years after exposure to ___.
- If left untreated, [#]% of patients with [disease name] may progress to develop [manifestation 1], [manifestation 2], and [manifestation 3].
Complications
- Common complications of Romano-Ward syndrome include:
Prognosis
- Prognosis is generally excellent/good/poor, and the 1/5/10-year mortality/survival rate of patients with [disease name] is approximately [--]%.
- Depending on the extent of the [tumor/disease progression] at the time of diagnosis, the prognosis may vary. However, the prognosis is generally regarded as poor/good/excellent.
- The presence of [characteristic of disease] is associated with a particularly [good/poor] prognosis among patients with [disease/malignancy].
- [Subtype of disease/malignancy] is associated with the most favorable prognosis.
- The prognosis varies with the [characteristic] of tumor; [subtype of disease/malignancy] have the most favorable prognosis.
Diagnosis
Diagnostic study of choice
- Molecular genetic testing is the gold standard test for the diagnosis of Romano-Ward syndrome which includes single-gene testing, use of a multigene testing panel, and more comprehensive genomic testing.
- The following result of molecular genetic testing is confirmatory of Jervell and Lange-Nielsen syndrome (JLNS):
History and Symptoms
Common Symptoms
Common symptoms of Romano-Ward syndrome include:
- Presyncope
- Syncope
- Palpitations: All the first three symptoms are normally self limiting and may reoccur most of the time
- Tachycardia
- Ventricular arrhythmia
- Torsade de pointes
Less Common Symptoms
Less common symptoms of Romano-Ward syndrome include
Physical Examination

Laboratory Findings
Electrocardiogram
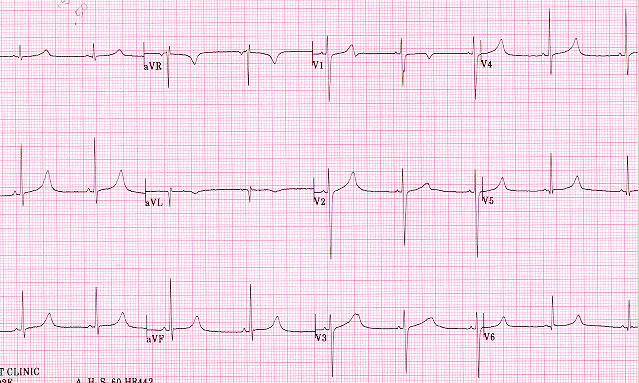
Romano-Ward syndrome with the broad based T pattern. Case courtesy by G. Michael Vincent, MD[21] - Prolongation of the QTc interval greater than 500 msec
- Tachyarrhythmias: due to abnormal cardiac depolarization and cardiac repolarization
- Ventricular tachycardia
- Torsade de pointes ventricular tachycardia
- Ventricular fibrillation

Causes
Mutations in the ANK2, KCNE1, KCNE2, KCNH2, KCNQ1, and SCN5A genes cause Romano-Ward syndrome. The proteins made by most of these genes form channels that transport positively-charged ions, such as potassium and sodium, in and out of cells.
In cardiac muscle, these ion channels play critical roles in maintaining the heart's normal rhythm. Mutations in any of these genes alter the structure or function of channels, which changes the flow of ions between cells.
A disruption in ion transport alters the way the heartbeats, leading to the abnormal heart rhythm characteristic of Romano-Ward syndrome.
Unlike most genes related to Romano-Ward syndrome, the ANK2 gene does not produce an ion channel. The protein made by the ANK2 gene ensures that other proteins, particularly ion channels, are inserted into the cell membrane appropriately.
A mutation in the ANK2 gene likely alters the flow of ions between cells in the heart, which disrupts the heart's normal rhythm and results in the features of Romano-Ward syndrome.
References
- ↑ Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K; et al. (1993). "GeneReviews®". PMID 20301308.
- ↑ Ackerman MJ, Siu BL, Sturner WQ, Tester DJ, Valdivia CR, Makielski JC; et al. (2001). "Postmortem molecular analysis of SCN5A defects in sudden infant death syndrome". JAMA. 286 (18): 2264–9. doi:10.1001/jama.286.18.2264. PMID 11710892.
- ↑ Arnestad M, Crotti L, Rognum TO, Insolia R, Pedrazzini M, Ferrandi C; et al. (2007). "Prevalence of long-QT syndrome gene variants in sudden infant death syndrome". Circulation. 115 (3): 361–7. doi:10.1161/CIRCULATIONAHA.106.658021. PMID 17210839.
- ↑ Schwartz PJ, Priori SG, Spazzolini C, Moss AJ, Vincent GM, Napolitano C; et al. (2001). "Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias". Circulation. 103 (1): 89–95. doi:10.1161/01.cir.103.1.89. PMID 11136691.
- ↑ Wedekind H, Bajanowski T, Friederich P, Breithardt G, Wülfing T, Siebrands C; et al. (2006). "Sudden infant death syndrome and long QT syndrome: an epidemiological and genetic study". Int J Legal Med. 120 (3): 129–37. doi:10.1007/s00414-005-0019-0. PMID 16012827.
- ↑ Juang JJ, Horie M (2016). "Genetics of Brugada syndrome". J Arrhythm. 32 (5): 418–425. doi:10.1016/j.joa.2016.07.012. PMC 5063259. PMID 27761167.
- ↑ Thomas D, Wimmer AB, Karle CA, Licka M, Alter M, Khalil M; et al. (2005). "Dominant-negative I(Ks) suppression by KCNQ1-deltaF339 potassium channels linked to Romano-Ward syndrome". Cardiovasc Res. 67 (3): 487–97. doi:10.1016/j.cardiores.2005.05.003. PMID 15950200.
- ↑ Barhanin J, Lesage F, Guillemare E, Fink M, Lazdunski M, Romey G (1996). "K(V)LQT1 and lsK (minK) proteins associate to form the I(Ks) cardiac potassium current". Nature. 384 (6604): 78–80. doi:10.1038/384078a0. PMID 8900282.
- ↑ Vincent GM (2002) The long QT syndrome. Indian Pacing Electrophysiol J 2 (4):127-42. PMID: 16951729
- ↑ Thomas D, Wimmer AB, Karle CA, Licka M, Alter M, Khalil M; et al. (2005). "Dominant-negative I(Ks) suppression by KCNQ1-deltaF339 potassium channels linked to Romano-Ward syndrome". Cardiovasc Res. 67 (3): 487–97. doi:10.1016/j.cardiores.2005.05.003. PMID 15950200.
- ↑ Juang JJ, Horie M (2016). "Genetics of Brugada syndrome". J Arrhythm. 32 (5): 418–425. doi:10.1016/j.joa.2016.07.012. PMC 5063259. PMID 27761167.
- ↑ Wedekind H, Bajanowski T, Friederich P, Breithardt G, Wülfing T, Siebrands C; et al. (2006). "Sudden infant death syndrome and long QT syndrome: an epidemiological and genetic study". Int J Legal Med. 120 (3): 129–37. doi:10.1007/s00414-005-0019-0. PMID 16012827.
- ↑ Schwartz PJ, Priori SG, Spazzolini C, Moss AJ, Vincent GM, Napolitano C; et al. (2001). "Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias". Circulation. 103 (1): 89–95. doi:10.1161/01.cir.103.1.89. PMID 11136691.
- ↑ Arnestad M, Crotti L, Rognum TO, Insolia R, Pedrazzini M, Ferrandi C; et al. (2007). "Prevalence of long-QT syndrome gene variants in sudden infant death syndrome". Circulation. 115 (3): 361–7. doi:10.1161/CIRCULATIONAHA.106.658021. PMID 17210839.
- ↑ Ackerman MJ, Siu BL, Sturner WQ, Tester DJ, Valdivia CR, Makielski JC; et al. (2001). "Postmortem molecular analysis of SCN5A defects in sudden infant death syndrome". JAMA. 286 (18): 2264–9. doi:10.1001/jama.286.18.2264. PMID 11710892.
- ↑ Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K; et al. (1993). "GeneReviews®". PMID 20301308.
- ↑ Schwartz PJ, Stramba-Badiale M, Crotti L, Pedrazzini M, Besana A, Bosi G; et al. (2009). "Prevalence of the congenital long-QT syndrome". Circulation. 120 (18): 1761–7. doi:10.1161/CIRCULATIONAHA.109.863209. PMC 2784143. PMID 19841298.
- ↑ Schwartz, Peter J.; Spazzolini, Carla; Crotti, Lia; Bathen, Jørn; Amlie, Jan P.; Timothy, Katherine; Shkolnikova, Maria; Berul, Charles I.; Bitner-Glindzicz, Maria; Toivonen, Lauri; Horie, Minoru; Schulze-Bahr, Eric; Denjoy, Isabelle (2006). "The Jervell and Lange-Nielsen Syndrome". Circulation. 113 (6): 783–790. doi:10.1161/CIRCULATIONAHA.105.592899. ISSN 0009-7322.
- ↑ Schwartz PJ, Spazzolini C, Crotti L, Bathen J, Amlie JP, Timothy K; et al. (2006). "The Jervell and Lange-Nielsen syndrome: natural history, molecular basis, and clinical outcome". Circulation. 113 (6): 783–90. doi:10.1161/CIRCULATIONAHA.105.592899. PMID 16461811.
- ↑ "The long QT syndrome".
- ↑ "The Long QT Syndrome".
- ↑ Goldenberg I, Horr S, Moss AJ, Lopes CM, Barsheshet A, McNitt S; et al. (2011). "Risk for life-threatening cardiac events in patients with genotype-confirmed long-QT syndrome and normal-range corrected QT intervals". J Am Coll Cardiol. 57 (1): 51–9. doi:10.1016/j.jacc.2010.07.038. PMC 3332533. PMID 21185501.
- ↑ Goldenberg I, Moss AJ, Peterson DR, McNitt S, Zareba W, Andrews ML; et al. (2008). "Risk factors for aborted cardiac arrest and sudden cardiac death in children with the congenital long-QT syndrome". Circulation. 117 (17): 2184–91. doi:10.1161/CIRCULATIONAHA.107.701243. PMC 3944375. PMID 18427136.
- ↑ Hobbs, Jenny B.; Peterson, Derick R.; Moss, Arthur J.; McNitt, Scott; Zareba, Wojciech; Goldenberg, Ilan; Qi, Ming; Robinson, Jennifer L.; Sauer, Andrew J.; Ackerman, Michael J.; Benhorin, Jesaia; Kaufman, Elizabeth S.; Locati, Emanuela H.; Napolitano, Carlo; Priori, Silvia G.; Towbin, Jeffrey A.; Vincent, G. Michael; Zhang, Li (2006). "Risk of Aborted Cardiac Arrest or Sudden Cardiac Death During Adolescence in the Long-QT Syndrome". JAMA. 296 (10): 1249. doi:10.1001/jama.296.10.1249. ISSN 0098-7484.