Mastitis overview
|
Mastitis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mastitis overview On the Web |
|
American Roentgen Ray Society Images of Mastitis overview |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Prince Tano Djan, BSc, MBChB [2]
Overview
Mastitis is the inflammation of the breast. Mastitis commonly affects breastfeeding mothers. This is referred to as puerperal mastitis. Non-puerperal mastitis occurs in non-breastfeeding mothers. Mastitis rarely occurs in men. Inflammatory breast cancer has symptoms very similar to mastitis and so appropriate history and investigation is needed to rule it out.
The use of the term mastitis varies by geographic region. In the United States the term mastitis usually refers to puerperal (occurring to breastfeeding mothers) mastitis with symptoms of systemic infection whereas outside the U.S. it is commonly used for puerperal and non-puerperal cases. The term Chronic cystic mastitis, also called fibrocystic disease, is characterized by noncancerous lumps in the breast.
Historical Perspective
Mastitis was first described by Dr. G. Ranney of Michigan in a paper read before the Section of Obstetrics Medicine at the Brighton meeting of the British Medical Association and in 1887 Dr. Charles J. Wright documented its treatment in the British Medical Journal.[1] From the 1930s to the 1960s an epidemic form of puerperal mastitis occurred frequently in hospital nurseries in industrialized countries.[2] During this period, hospital deliveries became more frequent, breastfeeding was not promoted, and the antibiotic era was only just beginning. The dominant role of staphylococcal infections and transmission between nursery personnel, infants and mothers was repeatedly demonstrated. Epidemic mastitis has been regarded as a hospital acquired disease caused by highly virulent strains of penicillin-resistant Staphylococcus aureus.[2]
Classification
Mastitis can be classified according to several subtypes based on the etiology, the duration of the disease, anatomical location, immunological association and age of the patient. Examples of this classification include puerperal or non-puerperal mastitis, chronic or acute mastitis, periductal or ductal, autoimmune or non-autoimmune (e.g. granulomatous and lupus mastitis)[3][4][5] and pre-pubertal mastitis.
Pathophysiology
Most clinically significant cases of nonpeurperal mastitis start as inflammation of the ductal and lobular system (galactophoritis) and possibly the immediately surrounding tissue (refer to the image below). Development of Nonpeurperal mastitis is the result of Secretory stasis whereas Peurperal mastitis occurs when bacteria, often from patients skin or the baby's mouth/nostrils [6] enters a milk duct through a crack in the nipple.
-
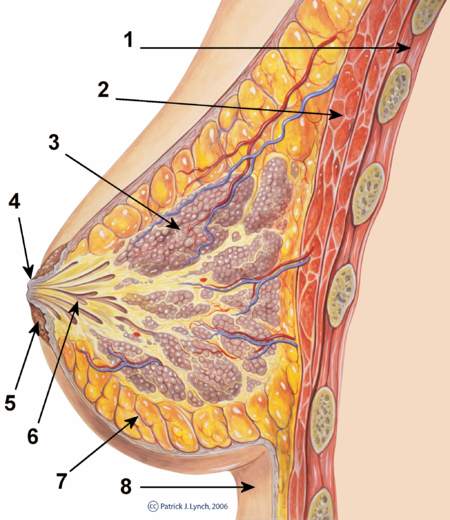
cross-section of the breast

1. Chest wall 2. Pectoralis muscles 3. Lobules 4. Nipple 5. Areola 6. Milk duct 7. Fatty tissue 8. Skin
-
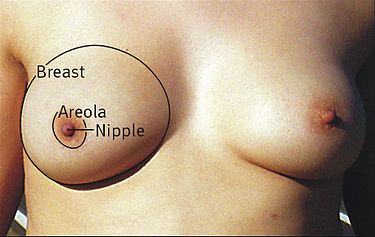
surface anatomy of the breast

Causes
Mastitis is caused by bacteria mostly Staphylococcus aureus[7] found on normal skin, Staphylococcus epidermidis, Streptococcus, E. coli, and Mycoplasma as well as Fungus mostly Candida sp. that may be found in the oral cavity of the baby.
Differentiating Mastitis overview from Other Diseases
Mastitis must be differentiated from other diseases that cause breast pain and/or swelling example; galactocele [8] [9], breast engorgement[10] [11] [12], mastodynia [13] [14] [15], fibrocystic breast disease, breast cancer, fibroadenoma, mondor disease[16] [17] and breast trauma.
Epidemiology and Demographics
Worldwide, the prevalence of mastitis ranges from a low of 1000 per 100,000 persons to a high of 10000 per 100,000 persons with an average prevalence of 4700 per 100,000 persons.[18] Worldwide, the incidence of Puerperal mastitis ranges from a low of 2900 per 100,000 persons to a high of 9500 per 100,000 persons with an average incidence of 6200 per 100,000 delieveries within the first seven weeks after delivery.[19] [20] [21]. Out of this, the incidence of those with mastitis needing hospitalization is 93 per 100,000 persons.[22]. The percentage of those with mastitis who develop breast abscess varies from 3% to 11%.[23] Mastitis commonly affects breastfeeding mothers between the ages of 21 to 35 with the highest occurrence between 30 to 34 years even when parity and full-time employment are controlled.[2] However, there is no difference between mastitis and breast abscess groups regarding age.[24] Women are more commonly affected with mastitis than men. There is no racial predilection to mastitis. Georgraphically the incidence of mastitis is higher in developing countries. [2]
Risk Factors
Mastitis usually occur in women who are breastfeeding. Women who are breastfeeding are at risk for developing mastitis especially if they have sore or cracked nipples or have had mastitis before while breastfeeding another baby. Also, the chances of getting mastitis increases if women use only one position to breastfeed or wear a tight-fitting bra, which may restrict milk flow. Mastitis that are not related to breastfeeding might be a rare form of breast cancer. Women with diabetes, chronic illness, AIDS, or an impaired immune system may be more susceptible to the development of mastitis.
Screening
According to the World Health Organization, there is no screening modality available for mastitis.[2]
Natural History, Complications, and Prognosis
If left untreated, up to 11% of patients with puerperal mastitis may progress to develop breast abscess. [25] Complications that may arise from mastitis include: recurrence, milk stasis and abscess formation. The prognosis is usually good and mastitis clears quickly with antibiotic therapy. Majority of smokers; (73%) [26] have the worst prognosis especially Nonpeurperal mastitis and higher rate of recurrence of breast abscesses.
Diagnosis
The diagnosis of mastitis is mostly clinical. In most cases, patients may present after few days of delivery with breast complaints local to a part of the breast, often close to the nipple and areola, more often the upper inner side of the breast, rarely whole breast affected and mostly only one breast.
History and Symptoms
In most cases, patients may present after few days of delivery with breast complaints local to a part of the breast, often close to the nipple and areola, more often the upper inner side of the breast, rarely whole breast affected and mostly only one breast.
The most common symptoms of mastitis include:[27][28] redness of the area, pain local to affected area and local differential warmth. Less commonly, some patients may also experience flu-like symptoms such as aches, shivering, and chills.
Physical Examination
Common physical examination findings of mastitis include low to high grade fever, breast tenderness, and swelling.[29]
Laboratory Findings
Some patients with mastitis have positive bacteria culture of breast milk.[29] Culture is rarely used to confirm bacterial infection of the milk because positive cultures can result from normal bacterial colonization, and negative cultures do not rule out mastitis. Culture has been recommended when the infection is severe, unusual, or hospital acquired, or if it fails to respond to two days' treatment with appropriate antibiotics.[2] Complete blood count may show elevated neutrophil count, though this is not specific to mastitis.
Electrocardiogram
There are no characteristic ECG findings of mastitis, however, mastitis has been reported to unmask type 1 Brugada Syndrome in which the ECG finding resolved when mastitis resolved.[30]
X-RAY
There are no characteristic ECG findings of mastitis, however, mastitis has been reported to unmask type 1 Brugada Syndrome in which the ECG finding resolved when mastitis resolved.[30]
CT SCAN
There are no CT scan findings diagnostic of mastitis. CT scan is helpful only when there is suspicious metastatic inflammatory breast disease.[31]
MRI
On contrast-enhanced MRI, most nonpuerperal mastitis are characterised by non-mass-like lesion with heterogeneous signal intensity. The observation of rim or rim-like enhancement on contrast-enhanced MRI with central hypointensity areas showing as hyperintensity on T2-weighted imaging is suggestive of the possibility of nonpuerperal mastitis.[32]
On MRI, most patients with granulomatous mastitis are characterised by segmental T2 hyperintensity with contrast-enhancement on T1[33] however, enhancing T2 hypointense mass with irregular margin was present in minority of patients with granulomatous mastitis.[33] [34] Among the available radiological modalities, MRI is the most specific in the diagnosis of mastitis.[35]
Ultrasound
On ultrasound mastitis may show edema of the fatty tissue, hypoechoic areas in the breast tissue, dilated ducts, fluid collections[36]or irregular hypoechoic masses suspicious for malignancy[37] [33]or hypoechoic mass-like lesions.[35]
Other Imaging Findings
On mammography, bacterial (puerperal or non-puerperal) mastitis usually shows ill-defined regions of increased density and skin thickening[34][35] [36]as shown below:.
-
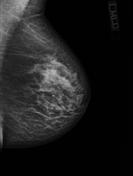
Mammogram of Mastitis

Treatment
Medical Therapy
Supportive care is the mainstay of therapy for peurperal mastitis. Supportive therapy includes massage, heat application, cold compresses and frequent breastfeeding. The treatment for non-peurperal mastitis is based on the underlying condition. Pharmacologic therapies for non-peurperal mastitis include Prolactin inhibiting agents, antimicrobial therapy, and nonsteroidal anti-inflammatory drugs (NSAIDS). Granulomatous mastitis has been treated with some success by a combination of steroids and Prolactin inhibiting medications.
Surgery
Surgical intervention is usually not the first line treatment option for patients with mastitis. Surgery is usually reserved for complicated mastitis with abscess formation that needs to be drained and granulomatous mastitis that may need excision.[38][39][40][41]
Prevention
Effective measures for the primary prevention of mastitis include avoidance of the risk factors as well as adhering to the following[2]:
- Early contact of infants with their mothers, and early start of breastfeeding usually within the first hour.
- Infants should stay in the same bed as their mother, or close to her in the same room.
- Breastfeeding mothers should receive skilled help and support for proper breastfeeding technique, whether or not she has breastfed before, to ensure good attachment, effective suckling and efficient milk removal;
- Every mother should be encouraged to breastfeed ‘on demand’, whenever the infant shows signs of readiness to feed, such as opening the mouth and searching for the breast.
- Every mother should understand the importance of unrestricted and exclusive breastfeeding and of avoiding the use of supplementary feeds, bottles and pacifiers.
- Women should receive skilled help to maintain lactation if their infants are too small or weak to suckle effectively.
- When a mother is in hospital, she needs skilled help at the first feed and for as many of the subsequent feeds as necessary.
- When a mother is at home, she needs skilled help during the first day after delivery, several times during the first two weeks, and subsequently as needed until she is breastfeeding effectively and confidently.
References
- ↑ Wright CJ (1887). "The Treatment of Mastitis". Br Med J. 2 (1386): 174. PMC 2534969. PMID 20752004.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 Department of Child and Adolescent Health and Development. Mastitis: causes and management. Geneva, Switzerland: World Health Organization; 2000. http://whqlibdoc.who.int/hq/2000/WHO_FCH_CAH_00.13.pdf.
- ↑ Altintoprak F, Kivilcim T, Yalkin O, Uzunoglu Y, Kahyaoglu Z, Dilek ON (2015). "Topical Steroids Are Effective in the Treatment of Idiopathic Granulomatous Mastitis". World J Surg. 39 (11): 2718–23. doi:10.1007/s00268-015-3147-9. PMID 26148520.
- ↑ Ocal K, Dag A, Turkmenoglu O, Kara T, Seyit H, Konca K (2010). "Granulomatous mastitis: clinical, pathological features, and management". Breast J. 16 (2): 176–82. doi:10.1111/j.1524-4741.2009.00879.x. PMID 20030652.
- ↑ Summers TA, Lehman MB, Barner R, Royer MC (2009). "Lupus mastitis: a clinicopathologic review and addition of a case". Adv Anat Pathol. 16 (1): 56–61. doi:10.1097/PAP.0b013e3181915ff7. PMID 19098467.
- ↑ Amir LH, Garland SM, Lumley J. (2006). "A case-control study of mastitis: nasal carriage of Staphylococcus aureus". BMC Family Practice. 7: 57. doi:10.1186/1471-2296-7-57.
- ↑ Montague EC, Hilinski J, Andresen D, Cooley A (2013). "Evaluation and treatment of mastitis in infants". Pediatr Infect Dis J. 32 (11): 1295–6. doi:10.1097/INF.0b013e3182a06448. PMID 24145956.
- ↑ Langer A, Mohallem M, Berment H, Ferreira F, Gog A, Khalifa D; et al. (2015). "Breast lumps in pregnant women". Diagn Interv Imaging. 96 (10): 1077–87. doi:10.1016/j.diii.2015.07.005. PMID 26341843.
- ↑ Canlorbe G, Bendifallah S (2015). "[Rare benign breast tumors including Abrikossoff tumor (granular cell tumor), erosive adenomatosis of the nipple, cytosteatonecrosis, fibromatosis (desmoid tumor), galactocele, hamartoma, hemangioma, lipoma, juvenile papillomatosis, pseudoangiomatous hyperplasia, and syringomatous adenoma: Guidelines for clinical practice]". J Gynecol Obstet Biol Reprod (Paris). 44 (10): 1030–48. doi:10.1016/j.jgyn.2015.09.034. PMID 26530177.
- ↑ Pustotina O (2016). "Management of mastitis and breast engorgement in breastfeeding women". J Matern Fetal Neonatal Med. 29 (19): 3121–5. doi:10.3109/14767058.2015.1114092. PMID 26513602.
- ↑ Leung SS (2016). "Breast pain in lactating mothers". Hong Kong Med J. doi:10.12809/hkmj154762. PMID 27313273.
- ↑ Anderson L, Kynoch K (2016). "Implementation of an education package on breast engorgement aimed at lactation consultants and midwives to prevent conflicting information for postnatal mothers". Int J Evid Based Healthc. doi:10.1097/XEB.0000000000000090. PMID 27465926.
- ↑ van Bogaert LJ (1986). "[Mastodynia and fibrocystic disease of the breast. Perspectives and methods of medical treatment]". J Gynecol Obstet Biol Reprod (Paris). 15 (6): 805–11. PMID 3794218.
- ↑ Songtish D, Akranurakkul P (2015). "Mastalgia: Characteristics and Associated Factors in Thai Women". J Med Assoc Thai. 98 Suppl 9: S9–15. PMID 26817204.
- ↑ Sen M, Kilic MO, Cemeroglu O, Icen D (2015). "Can mastalgia be another somatic symptom in fibromyalgia syndrome?". Clinics (Sao Paulo). 70 (11): 733–7. doi:10.6061/clinics/2015(11)03. PMC 4642489. PMID 26602519.
- ↑ Cox EM, Siegel DM (1997). "Mondor disease: an unusual consideration in a young woman with a breast mass". J Adolesc Health. 21 (3): 183–5. doi:10.1016/S1054-139X(97)00044-X. PMID 9283940.
- ↑ Belleflamme M, Penaloza A, Thoma M, Hainaut P, Thys F (2012). "Mondor disease: a case report in ED". Am J Emerg Med. 30 (7): 1325.e1–3. doi:10.1016/j.ajem.2011.06.031. PMID 21855258.
- ↑ Axelsson D, Blomberg M (2014). "Prevalence of postpartum infections: a population-based observational study". Acta Obstet Gynecol Scand. 93 (10): 1065–8. doi:10.1111/aogs.12455. PMID 25132521.
- ↑ Committee on Health Care for Underserved Women, American College of Obstetricians and Gynecologists (2007). "ACOG Committee Opinion No. 361: Breastfeeding: maternal and infant aspects". Obstet Gynecol. 109 (2 Pt 1): 479–80. PMID 17267864.
- ↑ Kaufmann R, Foxman B (1991). "Mastitis among lactating women: occurrence and risk factors". Soc Sci Med. 33 (6): 701–5. PMID 1957190.
- ↑ Foxman B, D'Arcy H, Gillespie B, Bobo JK, Schwartz K (2002). "Lactation mastitis: occurrence and medical management among 946 breastfeeding women in the United States". Am J Epidemiol. 155 (2): 103–14. PMID 11790672.
- ↑ Stafford I, Hernandez J, Laibl V, Sheffield J, Roberts S, Wendel G (2008). "Community-acquired methicillin-resistant Staphylococcus aureus among patients with puerperal mastitis requiring hospitalization". Obstet Gynecol. 112 (3): 533–7. doi:10.1097/AOG.0b013e31818187b0. PMID 18757649.
- ↑ Amir LH, Forster D, McLachlan H, Lumley J (2004). "Incidence of breast abscess in lactating women: report from an Australian cohort". BJOG. 111 (12): 1378–81. PMID 15663122.
- ↑ Dener C, Inan A (2003). "Breast abscesses in lactating women". World J Surg. 27 (2): 130–3. doi:10.1007/s00268-002-6563-6. PMID 12616423.
- ↑ Liu YY, Chen WC, Chen SL (2016). "[The Continued Breastfeeding Experiences of Women Who Suffer From Breast Abscess]". Hu Li Za Zhi. 63 (2): 49–57. doi:10.6224/JN.63.2.49. PMID 27026557.
- ↑ Risager R, Bentzon N (2010). "[Smoking and increased risk of mastitis]". Ugeskr Laeger. 172 (33): 2218–21. PMID 20727287.
- ↑ Kent JC, Ashton E, Hardwick CM, Rowan MK, Chia ES, Fairclough KA; et al. (2015). "Nipple Pain in Breastfeeding Mothers: Incidence, Causes and Treatments". Int J Environ Res Public Health. 12 (10): 12247–63. doi:10.3390/ijerph121012247. PMC 4626966. PMID 26426034.
- ↑ An JK, Woo JJ, Lee SA (2016). "Non-puerperal mastitis masking pre-existing breast malignancy: importance of follow-up imaging". Ultrasonography. 35 (2): 159–63. doi:10.14366/usg.15024. PMC 4825209. PMID 26169080.
- ↑ 29.0 29.1 Eglash A, Plane MB, Mundt M (2006). "History, physical and laboratory findings, and clinical outcomes of lactating women treated with antibiotics for chronic breast and/or nipple pain". J Hum Lact. 22 (4): 429–33. doi:10.1177/0890334406293431. PMID 17062789.
- ↑ 30.0 30.1 Ambardekar AV, Lewkowiez L, Krantz MJ (2009). "Mastitis unmasks Brugada syndrome". Int J Cardiol. 132 (3): e94–6. doi:10.1016/j.ijcard.2007.07.154. PMID 18036675.
- ↑ de Bazelaire C, Groheux D, Chapellier M, Sabatier F, Scémama A, Pluvinage A; et al. (2012). "Breast inflammation: indications for MRI and PET-CT". Diagn Interv Imaging. 93 (2): 104–15. doi:10.1016/j.diii.2011.12.004. PMID 22305594.
- ↑ Liu H, Peng W (2011). "Morphological manifestations of nonpuerperal mastitis on magnetic resonance imaging". J Magn Reson Imaging. 33 (6): 1369–74. doi:10.1002/jmri.22464. PMID 21591005.
- ↑ 33.0 33.1 33.2 Yildiz S, Aralasmak A, Kadioglu H, Toprak H, Yetis H, Gucin Z; et al. (2015). "Radiologic findings of idiopathic granulomatous mastitis". Med Ultrason. 17 (1): 39–44. doi:10.11152/mu.2013.2066.171.rfm. PMID 25745656.
- ↑ 34.0 34.1 Gautier N, Lalonde L, Tran-Thanh D, El Khoury M, David J, Labelle M; et al. (2013). "Chronic granulomatous mastitis: Imaging, pathology and management". Eur J Radiol. 82 (4): e165–75. doi:10.1016/j.ejrad.2012.11.010. PMID 23200627.
- ↑ 35.0 35.1 35.2 Tan H, Li R, Peng W, Liu H, Gu Y, Shen X (2013). "Radiological and clinical features of adult non-puerperal mastitis". Br J Radiol. 86 (1024): 20120657. doi:10.1259/bjr.20120657. PMC 3635790. PMID 23392197.
- ↑ 36.0 36.1 Jari I, Naum AG, Ursaru M, Manafu EG, Gheorghe L, Negru D (2015). "BREAST INFECTIONS: DIAGNOSIS WITH ULTRASOUND AND MAMMOGRAPHY". Rev Med Chir Soc Med Nat Iasi. 119 (2): 419–24. PMID 26204646.
- ↑ Cheng L, Reddy V, Solmos G, Watkins L, Cimbaluk D, Bitterman P; et al. (2015). "Mastitis, a Radiographic, Clinical, and Histopathologic Review". Breast J. 21 (4): 403–9. doi:10.1111/tbj.12430. PMID 25940456.
- ↑ Rogmans G (2003). "[Mastitis puerperalis]". Zentralbl Gynakol. 125 (2): 35–7. doi:10.1055/s-2003-40369. PMID 12836116.
- ↑ Stromps JP, Na HS, Grieb G, Orlikowsky T, Kuhl C, Pallua N (2014). "Surgical treatment of neonatal mastitis by periareolar drainage". Curr Pediatr Rev. 10 (4): 304–8. PMID 25594530.
- ↑ Yabanoğlu H, Çolakoğlu T, Belli S, Aytac HO, Bolat FA, Pourbagher A; et al. (2015). "A Comparative Study of Conservative versus Surgical Treatment Protocols for 77 Patients with Idiopathic Granulomatous Mastitis". Breast J. 21 (4): 363–9. doi:10.1111/tbj.12415. PMID 25858348.
- ↑ Yau FM, Macadam SA, Kuusk U, Nimmo M, Van Laeken N (2010). "The surgical management of granulomatous mastitis". Ann Plast Surg. 64 (1): 9–16. doi:10.1097/SAP.0b013e3181a20cae. PMID 20023450.