The pathophysiology of [disease/malignancy] depends on the histological subtype.
The pathophysiology of [disease/malignancy] depends on the histological subtype.
On gross pathology, characteristic findings of elastofibroma include:
* eosinophilic, beaded elastic fibers
On microscopic histopathological analysis, characteristic findings of nasopharyngeal angiofibroma include: <ref name="JenaPatnayak20162">{{cite journal|last1=Jena|first1=Amitabh|last2=Patnayak|first2=Rashmi|last3=Settipalli|first3=Sarla|last4=Nagesh|first4=N|title=Elastofibroma: An uncommon tumor revisited|journal=Journal of Cutaneous and Aesthetic Surgery|volume=9|issue=1|year=2016|pages=34|issn=0974-2077|doi=10.4103/0974-2077.178543}}</ref>
* Eosinophilic, beaded elastic fibers with Verhoeff's elastic stain
*
==Causes==
==Causes==
Line 339:
Line 349:
===Surgery===
===Surgery===
Surgical resection is considered only in symptomatic cases. <ref name="JenaPatnayak2016">{{cite journal|last1=Jena|first1=Amitabh|last2=Patnayak|first2=Rashmi|last3=Settipalli|first3=Sarla|last4=Nagesh|first4=N|title=Elastofibroma: An uncommon tumor revisited|journal=Journal of Cutaneous and Aesthetic Surgery|volume=9|issue=1|year=2016|pages=34|issn=0974-2077|doi=10.4103/0974-2077.178543}}</ref>
Surgical intervention is not recommended for the management of [disease name].
Surgical intervention is not recommended for the management of [disease name].
Elastofibroma was first discovered by Jarvi and Saxen, in 1961.[1]
The association between [important risk factor/cause] and [disease name] was made in/during [year/event].
In [year], [scientist] was the first to discover the association between [risk factor] and the development of [disease name].
In [year], [gene] mutations were first implicated in the pathogenesis of [disease name].
There have been several outbreaks of [disease name], including -----.
In [year], [diagnostic test/therapy] was developed by [scientist] to treat/diagnose [disease name].
Classification
There is no established system for the classification of [disease name].
OR
[Disease name] may be classified according to [classification method] into [number] subtypes/groups: [group1], [group2], [group3], and [group4].
OR
[Disease name] may be classified into [large number > 6] subtypes based on [classification method 1], [classification method 2], and [classification method 3].
[Disease name] may be classified into several subtypes based on [classification method 1], [classification method 2], and [classification method 3].
OR
Based on the duration of symptoms, [disease name] may be classified as either acute or chronic.
OR
If the staging system involves specific and characteristic findings and features:
According to the [staging system + reference], there are [number] stages of [malignancy name] based on the [finding1], [finding2], and [finding3]. Each stage is assigned a [letter/number1] and a [letter/number2] that designate the [feature1] and [feature2].
OR
The staging of [malignancy name] is based on the [staging system].
OR
There is no established system for the staging of [malignancy name].
Pathophysiology
Elastofibroma dorsi is a rare, slow growing, ill-defined soft tissue mass of the chest wall. It occurs most in the periscapular region.It is commonly located beneath latissimus dorsi and rhomboid major muscles near to the inferior angle of the scapula. It is a benign neoplasm with clinical appearence of a malignant tumor. [2]
The exact pathogenesis of elastofibroma dorsi is not fully understood. It is thought that elastofibroma dorsi is the result of subclinical microtrauma, reactive hyperplasia of elastic fibres and increased production of fibrous tissue. [3]
Elastofibroma occurrs predominantly on the right side. Only 10% of patients has bilateral involvement. [4]
OR
[Pathogen name] is usually transmitted via the [transmission route] route to the human host.
OR
Following transmission/ingestion, the [pathogen] uses the [entry site] to invade the [cell name] cell.
OR
[Disease or malignancy name] arises from [cell name]s, which are [cell type] cells that are normally involved in [function of cells].
OR
The progression to [disease name] usually involves the [molecular pathway].
OR
The pathophysiology of [disease/malignancy] depends on the histological subtype.
On gross pathology, characteristic findings of elastofibroma include:
eosinophilic, beaded elastic fibers
On microscopic histopathological analysis, characteristic findings of nasopharyngeal angiofibroma include: [5]
Eosinophilic, beaded elastic fibers with Verhoeff's elastic stain
Causes
Disease name] may be caused by [cause1], [cause2], or [cause3].
The cause of elastofibroma dorsi has not been identified. Subclinical microtrauma could be one of the reasons. [3]
OR
Common causes of [disease] include [cause1], [cause2], and [cause3].
OR
The most common cause of [disease name] is [cause 1]. Less common causes of [disease name] include [cause 2], [cause 3], and [cause 4].
OR
The cause of elastofibroma dorsi has not been identified. To review risk factors for the development of [disease name], click here.
Differentiating Elastofibroma dorsi from Other Diseases
Elastofibroma dorsi must be differentiated from desmoid tumours, neurofibroma and liposarcoma. [6]
Epidemiology and Demographics
The prevalence of elastofibroma is approximately 11200 in men and 24400 in women per 100,000 individuals in each gender autopsies. [7]
In [year], the incidence/prevalence of [disease name] was estimated to be [number range] cases per 100,000 individuals worldwide.
OR
In [year], the incidence of [disease name] is approximately [number range] per 100,000 individuals with a case-fatality rate of [number range]%.
Patients of all age groups may develop [disease name].
OR
The incidence of [disease name] increases with age; the median age at diagnosis is [#] years.
[Chronic disease name] is usually first diagnosed among [age group].
OR
Elastofibroma commonly affects females ranging from 35-94 years. [9]
There is no racial predilection to [disease name].
OR
Elastofibroma usually affects individuals of the [race 1] race. [Race 2] individuals are less likely to develop [disease name].
affects men and women equally.
OR
Female are more commonly affected by elastofibroma than men. The female to male ratio is approximately 2.1
The majority of elastofibroma cases are reported in Japan. [10]
OR
[Disease name] is a common/rare disease that tends to affect [patient population 1] and [patient population 2].
Risk Factors
There are no established risk factors for [disease name].
OR
The most potent risk factor in the development of [disease name] is [risk factor 1]. Other risk factors include [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] include [risk factor 1], [risk factor 2], [risk factor 3], and [risk factor 4].
OR
Common risk factors in the development of [disease name] may be occupational, environmental, genetic, and viral.
Screening
There is insufficient evidence to recommend routine screening for [disease/malignancy].
OR
According to the [guideline name], screening for [disease name] is not recommended.
OR
According to the [guideline name], screening for [disease name] by [test 1] is recommended every [duration] among patients with [condition 1], [condition 2], and [condition 3].
Natural History, Complications, and Prognosis
If left untreated, [#]% of patients with [disease name] may progress to develop [manifestation 1], [manifestation 2], and [manifestation 3].
OR
Common complications of [disease name] include [complication 1], [complication 2], and [complication 3].
OR
Prognosis is generally excellent/good/poor, and the 1/5/10-year mortality/survival rate of patients with [disease name] is approximately [#]%.
Diagnosis
Diagnostic Study of Choice
The diagnosis of [disease name] is made when at least [number] of the following [number] diagnostic criteria are met: [criterion 1], [criterion 2], [criterion 3], and [criterion 4].
OR
The diagnosis of [disease name] is based on the [criteria name] criteria, which include [criterion 1], [criterion 2], and [criterion 3].
OR
The diagnosis of [disease name] is based on the [definition name] definition, which includes [criterion 1], [criterion 2], and [criterion 3].
OR
There are no established criteria for the diagnosis of [disease name].
History and Symptoms
The majority of patients with elastofibroma dorsi are asymptomatic. Elastofibroma may present with:[11]
Painless swelling
Pain ( less than 10% of patients)
Scapular snapping
Limitation of motion,
Clunking sensation in the shoulder adduction-abduction movement[12]
scapular snapping, limitation of motion, clunking sensation in the shoulder adduction-abduction movement., limitation of motion, clunking sensation in the shoulder adduction-abduction movement.
The hallmark of [disease name] is [finding]. A positive history of [finding 1] and [finding 2] is suggestive of [disease name]. The most common symptoms of [disease name] include [symptom 1], [symptom 2], and [symptom 3]. Common symptoms of [disease] include [symptom 1], [symptom 2], and [symptom 3]. Less common symptoms of [disease name] include [symptom 1], [symptom 2], and [symptom 3].
Physical Examination
Patients with [disease name] usually appear [general appearance]. Physical examination of patients with [disease name] is usually remarkable for [finding 1], [finding 2], and [finding 3].
OR
Common physical examination findings of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
The presence of [finding(s)] on physical examination is diagnostic of [disease name].
OR
The presence of [finding(s)] on physical examination is highly suggestive of [disease name].
Laboratory Findings
An elevated/reduced concentration of serum/blood/urinary/CSF/other [lab test] is diagnostic of [disease name].
OR
Laboratory findings consistent with the diagnosis of [disease name] include [abnormal test 1], [abnormal test 2], and [abnormal test 3].
OR
[Test] is usually normal among patients with [disease name].
OR
Some patients with [disease name] may have elevated/reduced concentration of [test], which is usually suggestive of [progression/complication].
OR
There are no diagnostic laboratory findings associated with [disease name].
Electrocardiogram
There are no ECG findings associated with [disease name].
OR
An ECG may be helpful in the diagnosis of [disease name]. Findings on an ECG suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
X-ray
An x-ray may be helpful in the diagnosis of elastofibroma. Findings on an x-ray suggestive of elastofibroma include soft tissue density in the periscapular region. X-ray may be normal. [13]
Echocardiography or Ultrasound
There are no echocardiography/ultrasound findings associated with [disease name].
OR
Echocardiography/ultrasound may be helpful in the diagnosis of [disease name]. Findings on an echocardiography/ultrasound suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
There are no echocardiography/ultrasound findings associated with [disease name]. However, an echocardiography/ultrasound may be helpful in the diagnosis of complications of [disease name], which include [complication 1], [complication 2], and [complication 3].
CT scan
CT scan may be helpful in the diagnosis of elastofibroma dorsi. Findings on CT scan suggestive of elastofibroma dorsi include a heterogenous soft tissue mass with poorly defined margins. [14]
MRI
Magnetic resonance imaging is the most useful diagnostic tool for diagnosis of elastofibroma dorsi. [15]
Findings on MRI suggestive of elastofibroma include solitary heterogeneous, poorly circumscribed, soft-tissue mass.[16]
There are no MRI findings associated with [disease name]. However, a MRI may be helpful in the diagnosis of complications of [disease name], which include [complication 1], [complication 2], and [complication 3].
Other Imaging Findings
Positron emission tomography/computed tomography (PET/CT) may be helpful in the diagnosis of elastofibroma. Findings on PET/CT suggestive of elastofibroma include low to moderate metabolic activity in these patients. PET/CT shows low-grade diffuse 18F fluorodeoxyglucose uptake. [17]
Other Diagnostic Studies
Needle aspiration biopsy is helpful in the diagnosis of elastofibroma and exclude sarcoma. Findings suggestive of/diagnostic of [disease name] include [finding 1], [finding 2], and [finding 3].
OR
Other diagnostic studies for [disease name] include [diagnostic study 1], which demonstrates [finding 1], [finding 2], and [finding 3], and [diagnostic study 2], which demonstrates [finding 1], [finding 2], and [finding 3].
Treatment
Medical Therapy
There is no treatment for [disease name]; the mainstay of therapy is supportive care.
OR
Supportive therapy for [disease name] includes [therapy 1], [therapy 2], and [therapy 3].
OR
The majority of cases of [disease name] are self-limited and require only supportive care.
OR
[Disease name] is a medical emergency and requires prompt treatment.
OR
The mainstay of treatment for [disease name] is [therapy].
OR
The optimal therapy for [malignancy name] depends on the stage at diagnosis.
OR
[Therapy] is recommended among all patients who develop [disease name].
OR
Pharmacologic medical therapy is recommended among patients with [disease subclass 1], [disease subclass 2], and [disease subclass 3].
OR
Pharmacologic medical therapies for [disease name] include (either) [therapy 1], [therapy 2], and/or [therapy 3].
OR
Empiric therapy for [disease name] depends on [disease factor 1] and [disease factor 2].
OR
Patients with [disease subclass 1] are treated with [therapy 1], whereas patients with [disease subclass 2] are treated with [therapy 2].
Surgery
Surgical resection is considered only in symptomatic cases. [18]
Surgical intervention is not recommended for the management of [disease name].
OR
Surgery is not the first-line treatment option for patients with [disease name]. Surgery is usually reserved for symptomatic patients.[19]
OR
The mainstay of treatment for [disease name] is medical therapy. Surgery is usually reserved for patients with either [indication 1], [indication 2], and/or [indication 3].
OR
The feasibility of surgery depends on the stage of [malignancy] at diagnosis.
OR
Surgery is the mainstay of treatment for [disease or malignancy].
Primary Prevention
There are no established measures for the primary prevention of [disease name].
OR
There are no available vaccines against [disease name].
OR
Effective measures for the primary prevention of [disease name] include [measure1], [measure2], and [measure3].
OR
[Vaccine name] vaccine is recommended for [patient population] to prevent [disease name]. Other primary prevention strategies include [strategy 1], [strategy 2], and [strategy 3].
Secondary Prevention
There are no established measures for the secondary prevention of [disease name].
OR
Effective measures for the secondary prevention of [disease name] include [strategy 1], [strategy 2], and [strategy 3].
References
↑JARVI O, SAXEN E (1961). "Elastofibroma dorse". Acta Pathol Microbiol Scand Suppl. 51(Suppl 144): 83–4. PMID13789598.
↑Freixinet J, Rodríguez P, Hussein M, Sanromán B, Herrero J, Gil R (August 2008). "Elastofibroma of the thoracic wall". Interact Cardiovasc Thorac Surg. 7 (4): 626–8. doi:10.1510/icvts.2007.174722. PMID18407963.
↑Järvi OH, Länsimies PH (January 1975). "Subclinical elastofibromas in the scapular region in an autopsy series". Acta Pathol Microbiol Scand A. 83 (1): 87–108. PMID1124654.
↑Nagamine N, Nohara Y, Ito E (November 1982). "Elastofibroma in Okinawa. A clinicopathologic study of 170 cases". Cancer. 50 (9): 1794–805. PMID7116305.
↑Greenberg JA, Lockwood RC (March 1989). "Elastofibroma dorsi. A case report and review of the literature". Orthop Rev. 18 (3): 329–33. PMID2652048.
↑Hoffman JK, Klein MH, McInerney VK (April 1996). "Bilateral elastofibroma: a case report and review of the literature". Clin. Orthop. Relat. Res. (325): 245–50. PMID8998883.
↑Domanski HA, Carlén B, Sloth M, Rydholm A (December 2003). "Elastofibroma dorsi has distinct cytomorphologic features, making diagnostic surgical biopsy unnecessary: cytomorphologic study with clinical, radiologic, and electron microscopic correlations". Diagn. Cytopathol. 29 (6): 327–33. doi:10.1002/dc.10381. PMID14648789.
Elastofibroma is an ill-defined fibroelastic tumor-like condition made up of enlarged and irregular elastic fibers. On gross pathology, ill defined, nonencapsulated, rubbery, and firm, white lesion with interspersed fat are characteristic findings of elastofibroma. On microscopic histopathological analysis, heavy dense bands of collagenous tissue dissected by fat and abnormal elastic fibers are characteristic findings of elastofibroma . The elastic fibers are usually quite large and are easily identified. The elastic fibers are coarse, thick, and darkly eosinophilic, often fragmented into globules, creating a "string of pearls" or "pipe cleaner" appearance. Degeneration will cause the elastic fibers to appear as globules with a serrated or prickled edge. Elastofibroma may be caused by either trauma, genetic mutation, or systemic enzyme defects. Elastofibroma must be differentiated from other diseases that cause soft tissue tumor such as: spindle cell lipoma, nuchal-type fibroma, and fibromatosis colli. Elastofibroma may also be diagnosed using biopsy and histochemistry. Surgery is the mainstay of therapy for elastofibroma.
Pathophysiology
Elastofibroma, also called elastofibroma dorsi, is an ill-defined fibroelastic tumor-like condition made up of enlarged and irregular elastic fibers. [1][2]
The tumor develops very specifically in the subscapular or infrascapular area, deep to the muscle, and can be attached to periosteum of ribs. It is usually between the shoulder blade and the lower neck, with rare tumors reported in the chest wall. [1][3][2]
The genetic mutation in has been associated alterations of short arm of chromosome 1 with the development of elastofibroma.
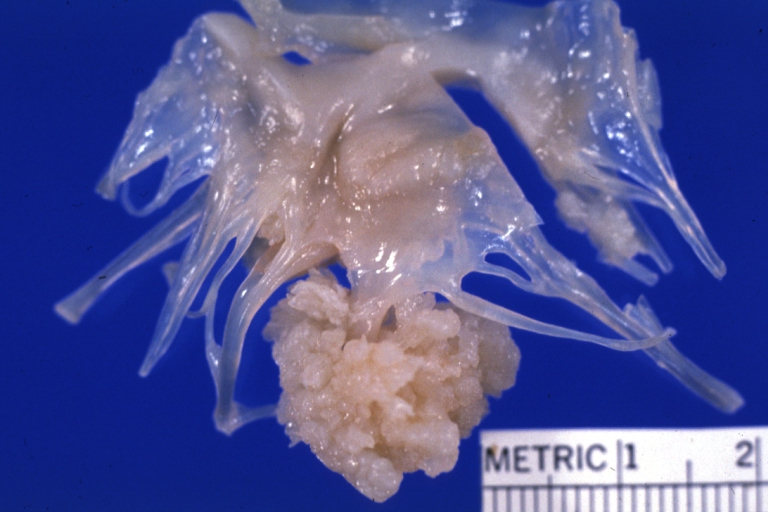
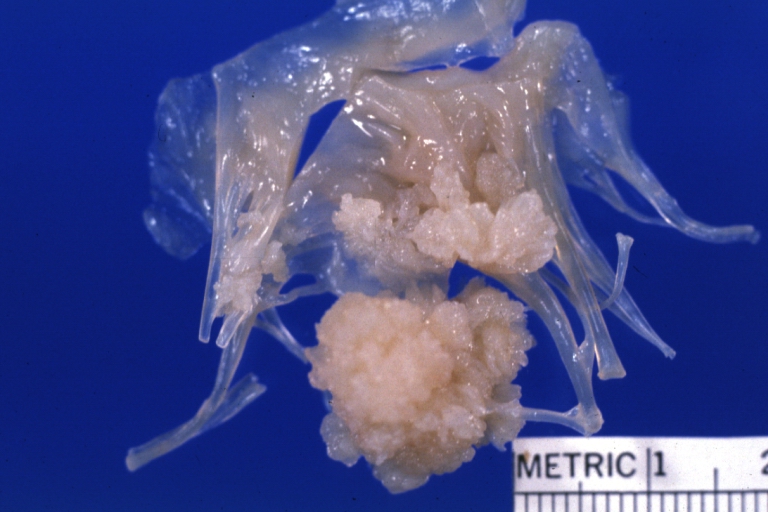
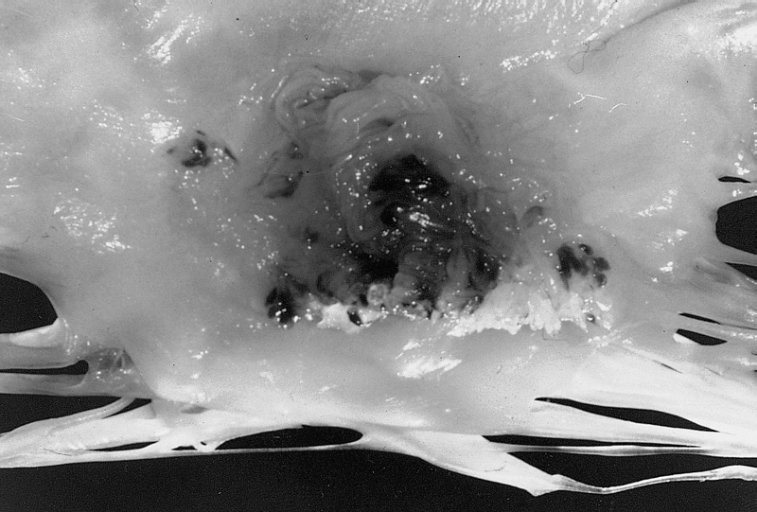
On gross pathology, ill defined, nonencapsulated, rubbery, and firm, white lesion with interspersed fat are characteristic findings of elastofibroma.
On microscopic histopathological analysis, heavy dense bands of collagenous tissue dissected by fat and abnormal elastic fibers are characteristic findings of elastofibroma. The elastic fibers are often quite large and are easily identified. The elastic fibers are coarse, thick, and darkly eosinophilic, often fragmented into globules, creating a "string of pearls" or "pipe cleaner" appearance. Degeneration will cause the elastic fibers to appear as globules with a serrated or prickled edge.
Elastofibroma
Elastofibroma
Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface.
Causes
Elastofibroma may be caused by either trauma, genetic mutation, or systemic enzyme defects.
Differentiating Elastofibroma from other Diseases
Elastofibroma must be differentiated from other diseases that cause soft tissue tumor such as:
↑ 2.02.1Briccoli, A.; Casadei, R.; Di Renzo, M.; Favale, L.; Bacchini, P.; Bertoni, F. (2000). "Elastofibroma dorsi". Surgery today. 30 (2): 147–152. doi:10.1007/pl00010063. PMID10664338.
↑Mortman, K. D.; Hochheiser, G. M.; Giblin, E. M.; Manon-Matos, Y.; Frankel, K. M. (2007). "Elastofibroma Dorsi: Clinicopathologic Review of 6 Cases". The Annals of Thoracic Surgery. 83 (5): 1894–1897. doi:10.1016/j.athoracsur.2006.11.050. PMID17462431.