Acute myeloid leukemia: Difference between revisions
mNo edit summary |
m (Robot: Changing Category:Mature chapter to Category:Overview complete) |
||
| Line 373: | Line 373: | ||
[[Category:Types of cancer]] | [[Category:Types of cancer]] | ||
[[Category:Oncology]] | [[Category:Oncology]] | ||
[[Category: | [[Category:Overview complete]] | ||
Revision as of 18:26, 17 April 2012
For patient information click here
Template:DiseaseDisorder infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Acute myeloid leukemia (AML), also known as acute myelogenous leukemia, is a cancer of the myeloid line of white blood cells, characterized by the rapid proliferation of abnormal cells which accumulate in the bone marrow and interfere with the production of normal blood cells. AML is the most common acute leukemia affecting adults, and its incidence increases with age. Although AML is a relatively rare disease, accounting for approximately 1.2% of cancer deaths in the United States,[1] its incidence is expected to increase as the population ages.
The symptoms of AML are caused by replacement of normal bone marrow with leukemic cells, resulting in a drop in red blood cells, platelets, and normal white blood cells. These symptoms include fatigue, shortness of breath, easy bruising and bleeding, and increased risk of infection. Although several risk factors for AML have been identified, the specific cause of AML remains unclear. As an acute leukemia, AML progresses rapidly and is typically fatal within weeks or months if left untreated.
Acute myeloid leukemia is a potentially curable disease; but only a minority of patients are cured with current therapy. AML is treated initially with chemotherapy aimed at inducing a remission; some patients may go on to receive a hematopoietic stem cell transplant.
Areas of active research in acute myeloid leukemia include further elucidation of the cause of AML, identification of better prognostic indicators, development of new methods of detecting residual disease after treatment, and the development of new drugs and targeted therapies.
History
The first published description of a case of leukemia in medical literature dates to 1827, when a French physician named Alfred-Armand-Louis-Marie Velpeau described a 63-year-old florist who developed an illness characterized by fever, weakness, urinary stones, and substantial enlargement of the liver and spleen. Velpeau noted that the blood of this patient had a consistency "like gruel", and speculated that the appearance of the blood was due to white corpuscles.[2] In 1845, a series of patients who died with enlarged spleens and changes in the "colors and consistencies of their blood" was reported by the Edinburgh-based pathologist J.H. Bennett; he used the term "leucocythemia" to describe this pathological condition.[3]
The term "leukemia" was coined by Rudolf Virchow, the renowned German pathologist, in 1856. As a pioneer in the use of the light microscope in pathology, Virchow was the first to describe the abnormal excess of white blood cells in patients with the clinical syndrome described by Velpeau and Bennett. As Virchow was uncertain of the cause of the white blood cell excess, he used the purely descriptive term "leukemia" (Greek: "white blood") to refer to the condition.[4]
Further advances in the understanding of acute myeloid leukemia occurred rapidly with the development of new technology. In 1877, Paul Ehrlich developed a technique of staining blood films which allowed him to describe in detail normal and abnormal white blood cells. Wilhelm Ebstein introduced the term "acute leukemia" in 1889 to differentiate rapidly progressive and fatal leukemias from the more indolent chronic leukemias.[5] The term "myeloid" was coined by Neumann in 1869, as he was the first to recognize that white blood cells were made in the bone marrow (Greek: µυєλός, myelos = (bone) marrow) as opposed to the spleen. The technique of bone marrow examination to diagnose leukemia was first described in 1879 by Mosler.[6] Finally, in 1900 the myeloblast, which is the malignant cell in AML, was characterized by Naegeli, who divided the leukemias into myeloid and lymphocytic.[7] [8]
Signs and symptoms
Most signs and symptoms of AML are due to an increased number of malignant white blood cells displacing or otherwise interfering with production of normal blood cells in the bone marrow. A lack of normal white blood cell production makes the patient susceptible to infections (while the leukemic cells themselves are derived from white blood cell precursors, they have no infection-fighting capacity).[9] A lack of red blood cells (anemia) can cause fatigue, paleness, and shortness of breath. A lack of platelets can lead to easy bruising or bleeding with minor trauma.
The early signs of AML are often non-specific, and may be similar to those of influenza or other common illnesses. Some generalized symptoms include fever, fatigue, weight loss or loss of appetite, shortness of breath with exertion, anemia, easy bruising or bleeding, petechiae (flat, pin-head sized spots under the skin caused by bleeding), bone pain and joint pain and persistent or frequent infections.[9]
Enlargement of the spleen may occur in AML, but it is typically mild and asymptomatic. Lymph node swelling is rare in AML, in contrast to acute lymphoblastic leukemia. The skin is involved about 10% of the time in the form of leukemia cutis. Rarely, Sweet's syndrome, a paraneoplastic inflammation of the skin, can occur with AML.[9]
Some patients with AML may experience swelling of the gums because of infiltration of leukemic cells into the gum tissue. Rarely, the first sign of leukemia may be the development of a solid leukemic mass or tumor outside of the bone marrow, called a chloroma. Occasionally, a person may show no symptoms, and the leukemia may be discovered incidentally during a routine blood test.[10]
Causes
A number of risk factors for developing AML have been identified, including:
- "Pre-leukemic" blood disorders such as myelodysplastic or myeloproliferative syndromes can evolve into AML; the exact risk depends on the type of MDS/MPS.[11]
- Exposure to anti-cancer chemotherapy, in particular alkylating agents, can increase the risk for the subsequent development of AML. The risk is highest about 3–5 years after chemotherapy.[12] Other chemotherapy agents, specifically epipodophyllotoxins and anthracyclines, have also been associated with treatment-related leukemia. These treatment-related leukemias are often associated with specific chromosomal abnormalities in the leukemic cells.[13]
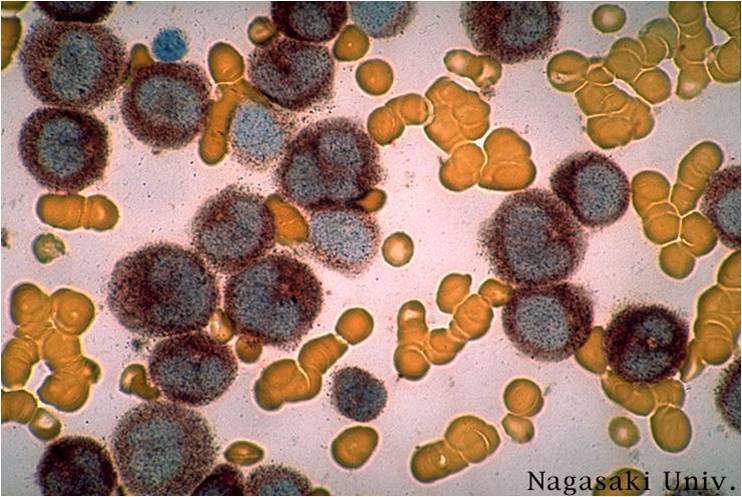
- Ionizing radiation exposure can increase the risk of AML. Survivors of the atomic bombings of Hiroshima and Nagasaki had an increased rate of AML,[14] as did radiologists exposed to high levels of X-rays prior to the adoption of modern radiation safety practices.[15]
- Occupational chemical exposure to benzene and other aromatic organic solvents is controversial as a cause of AML. Benzene and many of its derivatives are known to be carcinogenic in vitro. While some studies have suggested a link between occupational exposure to benzene and increased risk of AML,[16] others have suggested that the attributable risk, if any, is slight.[17]
- Several congenital conditions may increase the risk of leukemia; the most common is probably Down syndrome, which is associated with a 10- to 18-fold increase in the risk of AML.[18]
Epidemiology
Acute myeloid leukemia is a relatively rare cancer. There are approximately 10,500 new cases each year in the United States, and the incidence rate has remained stable from 1995 through 2005. AML accounts for 1.2% of all cancer deaths in the United States.[1]
The incidence of AML increases with age; the median age at diagnosis is 63 years. AML accounts for about 90% of all acute leukemias in adults, but is rare in children.[1] The rate of therapy-related AML (that is, AML caused by previous chemotherapy) is rising; therapy-related disease currently accounts for about 10–20% of all cases of AML.[19] AML is slightly more common in men, with a male-to-female ratio of 1.3:1.[20]
There is some geographic variation in the incidence of AML. In adults, the highest rates are seen in North America, Europe, and Oceania, while adult AML is rarer in Asia and Latin America.[21][22] In contrast, childhood AML is less common in North America and India than in other parts of Asia.[23] These differences may be due to population genetics, environmental factors, or a combination of the two.
A hereditary risk for AML appears to exist. There are numerous reports of multiple cases of AML developing in a family at a rate higher than predicted by chance alone.[24][25][26][27] The risk of developing AML is increased threefold in first-degree relatives of patients with AML.[28]
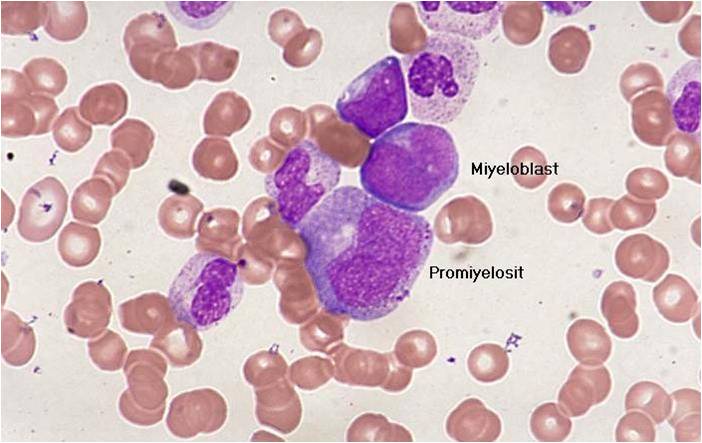
Pathophysiology
The malignant cell in AML is the myeloblast. In normal hematopoiesis, the myeloblast is an immature precursor of myeloid white blood cells; a normal myeloblast will gradually mature into a mature white blood cell. However, in AML, a single myeloblast accumulates genetic changes which "freeze" the cell in its immature state and prevent differentiation.[29] Such a mutation alone does not cause leukemia; however, when such a "differentiation arrest" is combined with other mutations which disrupt genes controlling proliferation, the result is the uncontrolled growth of an immature clone of cells, leading to the clinical entity of AML.[30]
Much of the diversity and heterogeneity of AML stems from the fact that leukemic transformation can occur at a number of different steps along the differentiation pathway.[31] Modern classification schemes for AML recognize that the characteristics and behavior of the leukemic cell (and the leukemia) may depend on the stage at which differentiation was halted.
Specific cytogenetic abnormalities can be found in many patients with AML; the types of chromosomal abnormalities often have prognostic significance.[32] The chromosomal translocations encode abnormal fusion proteins, usually transcription factors whose altered properties may cause the "differentiation arrest."[33] For example, in acute promyelocytic leukemia, the t(15;17) translocation produces a PML-RARα fusion protein which binds to the retinoic acid receptor element in the promoters of several myeloid-specific genes and inhibits myeloid differentiation.[34]
The clinical signs and symptoms of AML result from the fact that, as the leukemic clone of cells grows, it tends to displace or interfere with the development of normal blood cells in the bone marrow.[35] This leads to neutropenia, anemia, and thrombocytopenia. The symptoms of AML are in turn often due to the low numbers of these normal blood elements. In rare cases, patients can develop a chloroma, or solid tumor of leukemic cells outside the bone marrow, which can cause various symptoms depending on its location.[9]
Diagnosis
The first clue to a diagnosis of AML is typically an abnormal result on a complete blood count. While an excess of abnormal white blood cells (leukocytosis) is a common finding, and leukemic blasts are sometimes seen, AML can also present with isolated decreases in platelets, red blood cells, or even with a low white blood cell count (leukopenia).[36] While a presumptive diagnosis of AML can be made via examination of the peripheral blood smear when there are circulating leukemic blasts, a definitive diagnosis usually requires an adequate bone marrow aspiration and biopsy
A bone marrow examination is often performed to identify the type of abnormal blood cells; however, if there are many leukemic cells circulating in the peripheral blood, a bone marrow biopsy may not be necessary. Marrow or blood is examined via light microscopy as well as flow cytometry to diagnose the presence of leukemia, to differentiate AML from other types of leukemia (e.g. acute lymphoblastic leukemia), and to classify the subtype of disease (see below). A sample of marrow or blood is typically also tested for chromosomal translocations by routine cytogenetics or fluorescent in situ hybridization.
The diagnosis and classification of AML can be challenging, and should be performed by a qualified hematopathologist or hematologist. In straightforward cases, the presence of certain morphologic features (such as Auer rods) or specific flow cytometry results can distinguish AML from other leukemias; however, in the absence of such features, diagnosis may be more difficult.[37]
According to the widely used WHO criteria, the diagnosis of AML is established by demonstrating involvement of more than 20% of the blood and/or bone marrow by leukemic myeloblasts.[38] AML must be carefully differentiated from "pre-leukemic" conditions such as myelodysplastic or myeloproliferative syndromes, which are treated differently.
Because acute promyelocytic leukemia (APL) has the highest curability and requires a unique form of treatment, it is important to quickly establish or exclude the diagnosis of this subtype of leukemia. Fluorescent in situ hybridization performed on blood or bone marrow is often used for this purpose, as it readily identifies the chromosomal translocation (t[15;17]) that characterizes APL.[39]
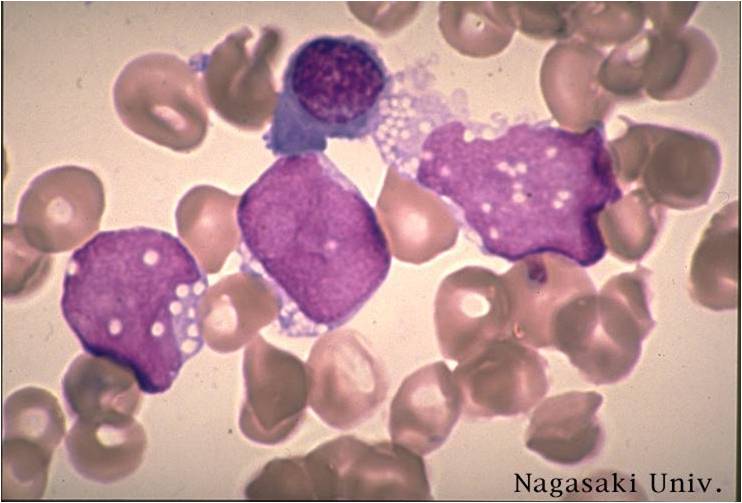
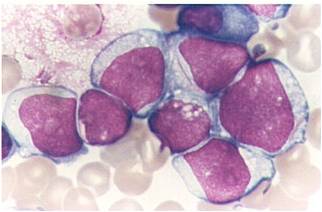
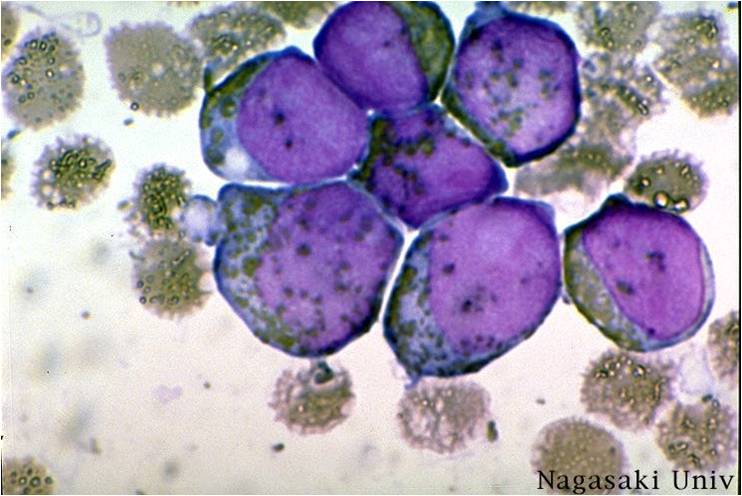
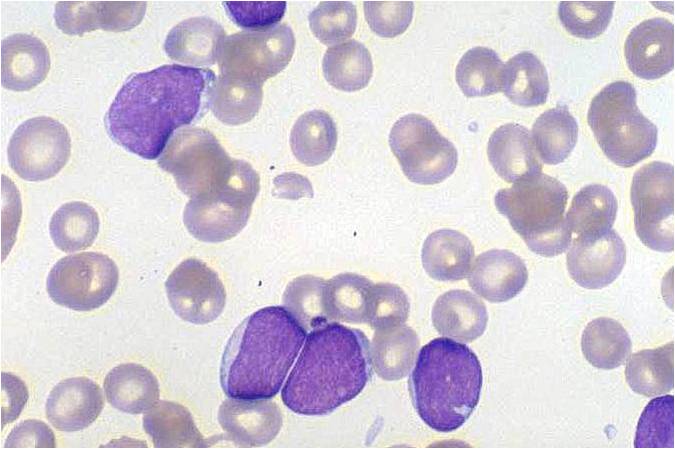
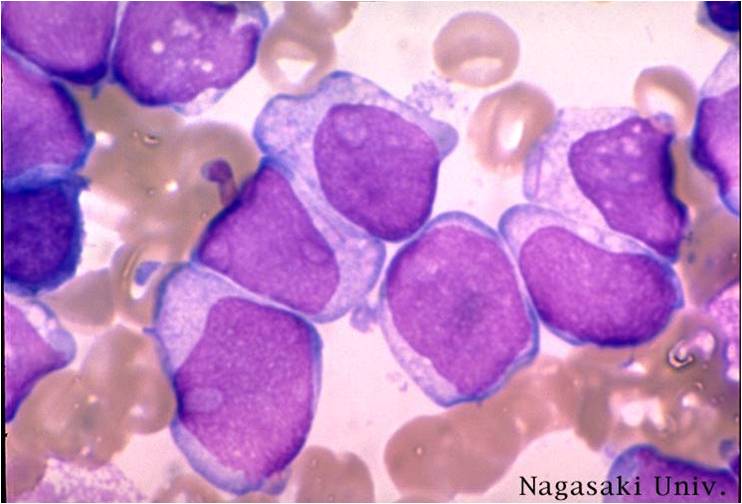
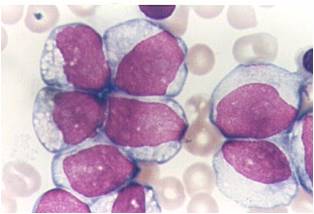
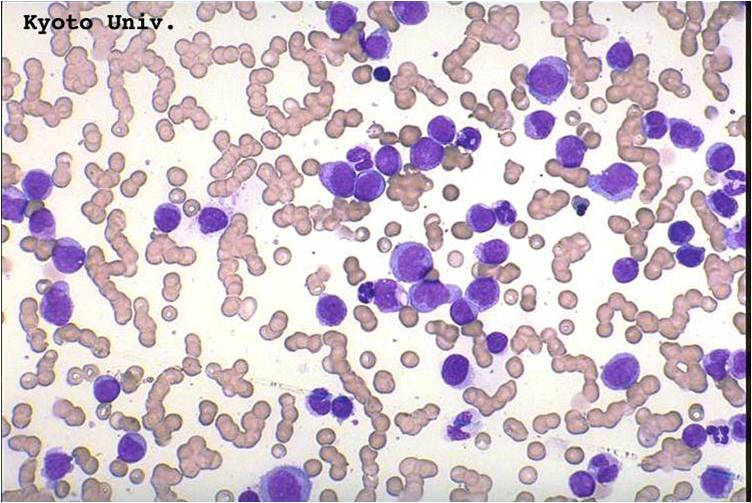
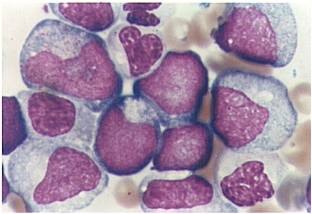
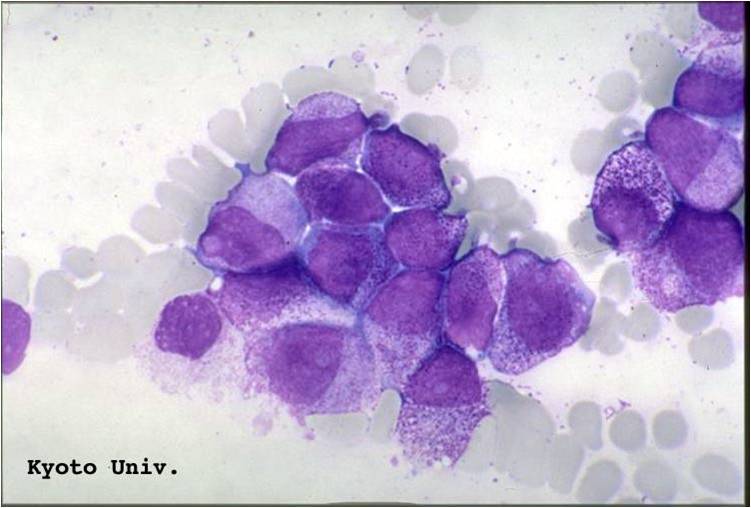
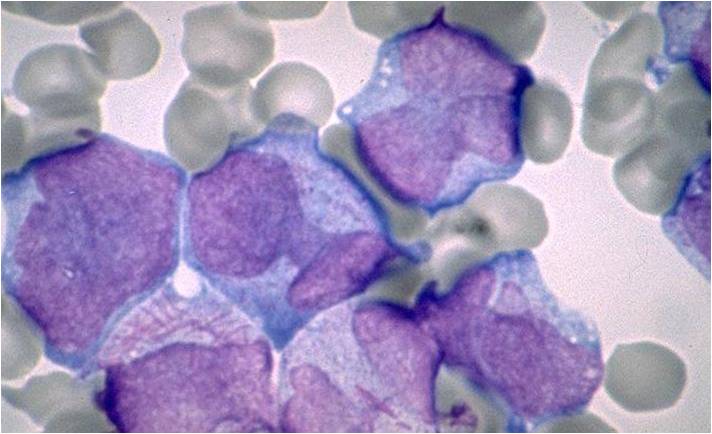
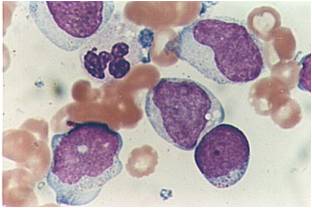
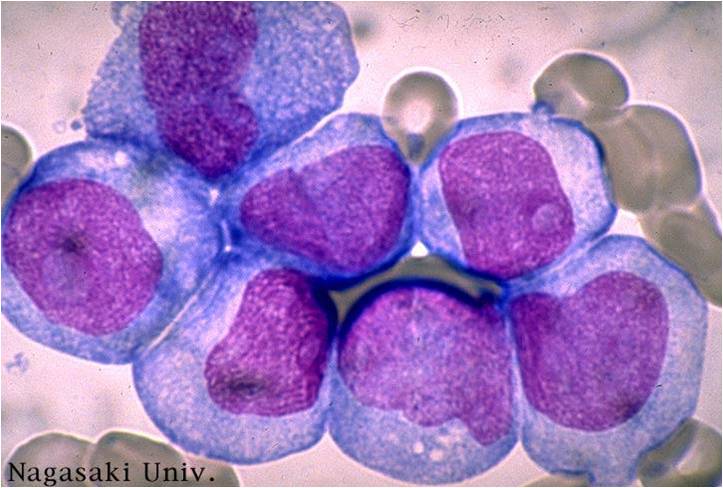
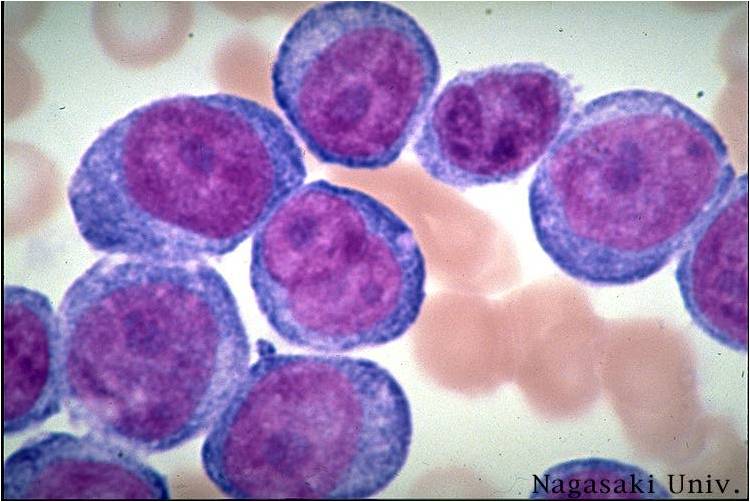
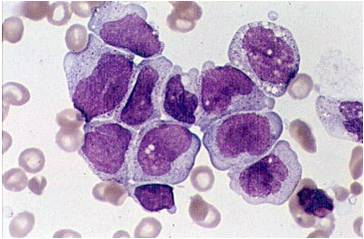
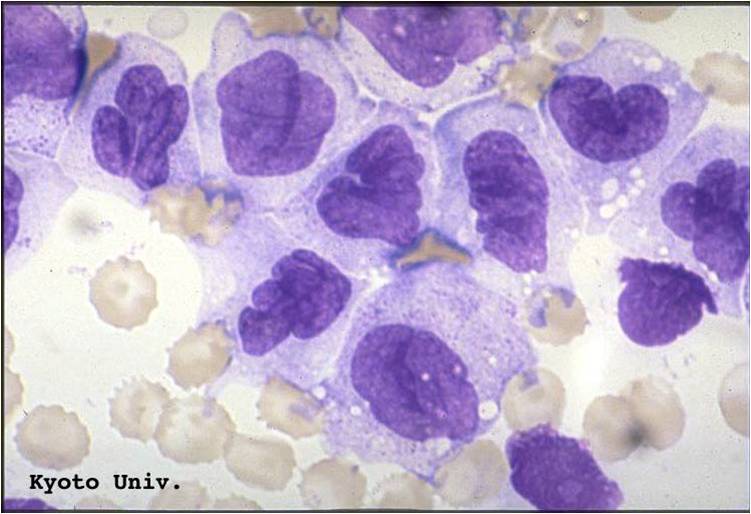
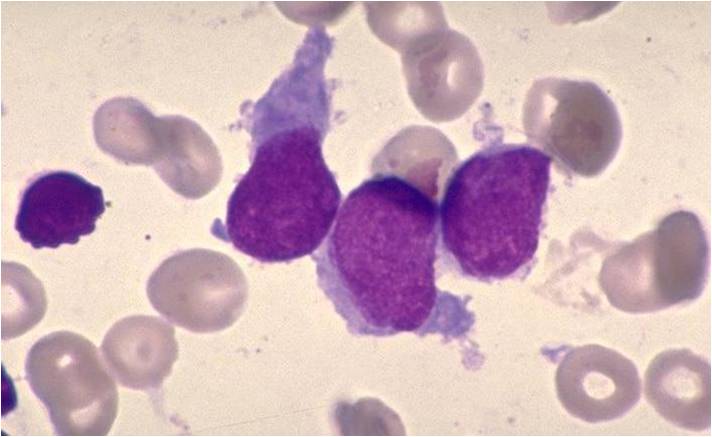
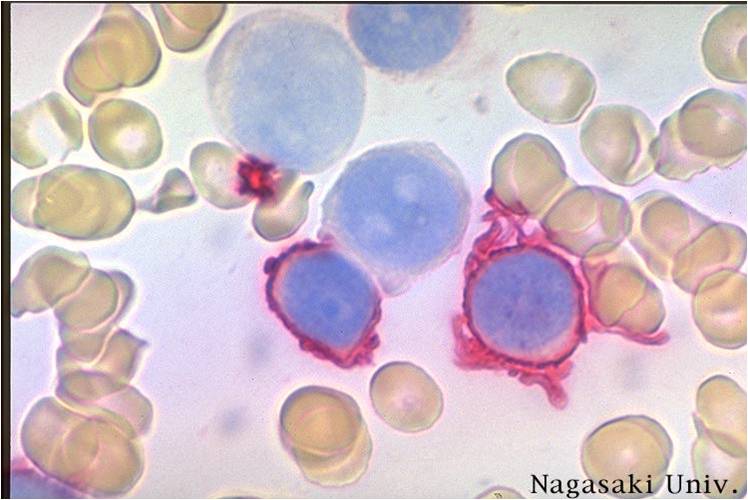
Pathology
![AML - Auer Rods, DIC[40]](/index.php/File:AML.jpg)
![AML (with Auer Rods)[41]](/index.php/File:AML_(with_Auer_Rods).jpg)
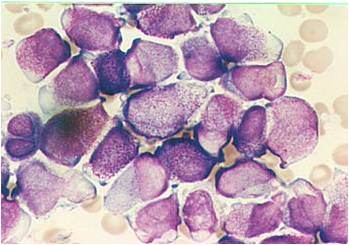
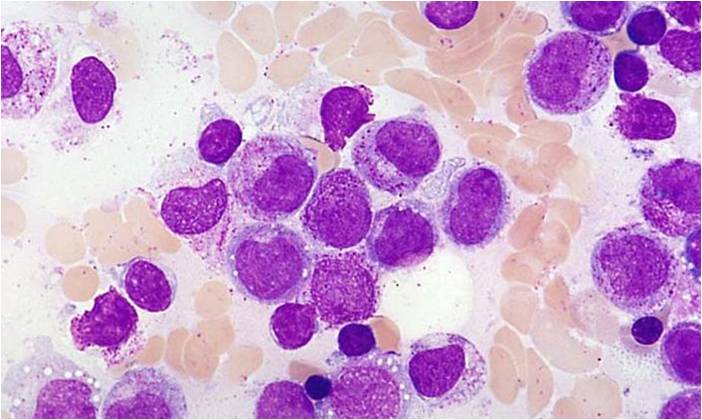
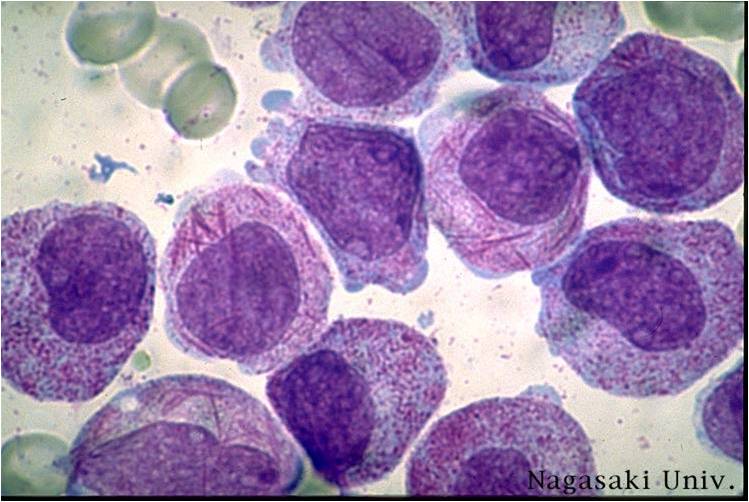
(Images shown below are courtesy of Melih Aktan MD., Istanbul Medical Faculty - Turkey, and Kyoto University - Japan)
-
AML-M0
-
AML-M1


-
AML-M1 peroxidase
-
AML-M1


-
AML-M1
-
AML-M1


-
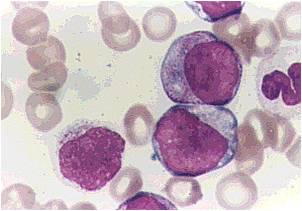
AML-M2
-
AML-M2


-
AML-M2
-
AML-M2


-
AML-M3
-
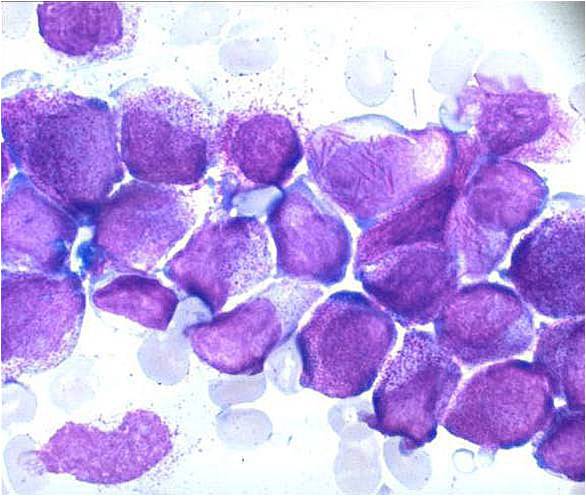
AML-M3


-
AML-M3
-
AML-M3


-
AML-M3 Auer bodies
-
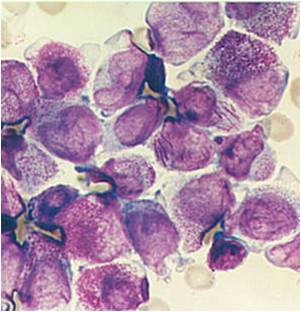
AML-M3 Auer bodies


-
AML-M3 variation
-
AML-M4


-
AML-M5a
-
AML-M5a


-
AML-M5a (alpha naphtyle acetat)
-
AML-M5b


-
AML-M5b
-
AML-M7
-
AML-M7



Classification
The two most commonly used classification schemata for AML, as of 2006, are the older French-American-British (FAB) system and the newer World Health Organization (WHO) system.
French-American-British classification
The French-American-British (FAB) classification system divided AML into 8 subtypes, M0 through to M7, based on the type of cell from which the leukemia developed and its degree of maturity. This is done by examining the appearance of the malignant cells under light microscopy and/or by using cytogenetics to characterize any underlying chromosomal abnormalities. The subtypes have varying prognoses and responses to therapy. Although the WHO classification (see below) may be more useful, the FAB system is still widely used as of mid-2006.
The eight FAB subtypes are:[42]
- M0 (undifferentiated AML)
- M1 (myeloblastic, without maturation)
- M2 (myeloblastic, with maturation)
- M3 (promyelocytic), or acute promyelocytic leukemia (APL)
- M4 (myelomonocytic)
- M4eo (myelomonocytic together with bone marrow eosinophilia)
- M5 monoblastic leukemia (M5a) or monocytic leukemia (M5b)
- M6 (erythrocytic), or erythroleukemia
- M7 (megakaryoblastic)
World Health Organization classification
The World Health Organization (WHO) classification of acute myeloid leukemia attempts to be more clinically useful and to produce more meaningful prognostic information than the FAB criteria. Each of the WHO categories contains numerous descriptive sub-categories of interest to the hematopathologist and oncologist; however, most of the clinically significant information in the WHO schema is communicated via categorization into one of the five subtypes listed below.
The WHO subtypes of AML are:[43]
- AML with characteristic genetic abnormalities, which includes AML with translocations between chromosome 8 and 21 [t(8;21)], inversions in chromosome 16 [inv(16)], or translocations between chromosome 15 and 17 [t(15;17)]. Patients with AML in this category generally have a high rate of remission and a better prognosis compared to other types of AML.
- AML with multilineage dysplasia. This category includes patients who have had a prior myelodysplastic syndrome (MDS) or myeloproliferative disease (MPD) that transforms into AML. This category of AML occurs most often in elderly patients and often has a worse prognosis.
- AML and MDS, therapy-related. This category includes patients who have had prior chemotherapy and/or radiation and subsequently develop AML or MDS. These leukemias may be characterized by specific chromosomal abnormalities, and often carry a worse prognosis.
- AML not otherwise categorized. Includes subtypes of AML that do not fall into the above categories.
- Acute leukemias of ambiguous lineage. Acute leukemias of ambiguous lineage (also known as mixed phenotype or biphenotypic acute leukemia) occur when the leukemic cells can not be classified as either myeloid or lymphoid cells, or where both types of cells are present.
Prognosis

Acute myeloid leukemia is a curable disease; the chance of cure for a specific patient depends on a number of prognostic factors.[44]
Cytogenetics and prognosis in AML
The single most important prognostic factor in AML is cytogenetics, or the chromosomal structure of the leukemic cell. Certain cytogenetic abnormalities are associated with very good outcomes (for example, the (15;17) translocation in acute promyelocytic leukemia). About half of AML patients have "normal" cytogenetics; they fall into an intermediate risk group. A number of other cytogenetic abnormalities are known to associate with a poor prognosis and a high risk of relapse after treatment.[45][46][47]
The first publication to address cytogenetics and prognosis was the MRC trial of 1998:[48]
| Risk Category | Abnormality | 5-year survival | Relapse rate |
|---|---|---|---|
| Favorable | t(8;21), t(15;17), inv(16) | 70% | 33% |
| Intermediate | Normal, +8, +21, +22, del(7q), del(9q), Abnormal 11q23, all other structural or numerical changes | 48% | 50% |
| Adverse | -5, -7, del(5q), Abnormal 3q, Complex cytogenetics | 15% | 78% |
Later, the Southwest Oncology Group and Eastern Cooperative Oncology Group,[49] and later still, Cancer and Leukemia Group B published other, mostly overlapping lists of cytogenetics prognostication in leukemia[50]
Antecedent MDS and prognosis
AML which arises from a pre-existing myelodysplastic syndrome or myeloproliferative disease (so-called secondary AML) has a worse prognosis, as does treatment-related AML arising after chemotherapy for another previous malignancy. Both of these entities are associated with a high rate of unfavorable cytogenetic abnormalities.[51][52][53]
Other prognostic markers
In some studies, age >60 years and elevated lactate dehydrogenase level were also associated with poorer outcomes.[54] As with most forms of cancer, performance status (i.e. the general physical condition and activity level of the patient) plays a major role in prognosis as well.
FLT3 internal tandem duplications (ITDs) have been shown to confer a poorer prognosis in AML.[55] Treating these patients with more aggressive therapy, such as stem-cell transplantation in first remission, has not been shown to enhance long-term survival, so this prognostic feature is of uncertain clinical significance at this point.[56]
Researchers are investigating the clinical significance of c-KIT mutations[57] in AML. These are prevalent, and clinically relevant because of the availability of tyrosine kinase inhibitors, such as sunitinib and imatinib that can block the activity of c-KIT pharmacologically.
Other genes being investigated as prognostic factors or therapeutic targets include CEBPA, BAALC, ERG, and NPM1.
Overall expectation of cure
Cure rates in clinical trials have ranged from 20–45%;[58][59] however, it should be noted that clinical trials often include only younger patients and those able to tolerate aggressive therapies. The overall cure rate for all patients with AML (including the elderly and those unable to tolerate aggressive therapy) is likely lower. Cure rates for promyelocytic leukemia can be as high as 98%.[60]
Treatment
Treatment of AML consists primarily of chemotherapy, and is divided into two phases: induction and postremission (or consolidation) therapy. The goal of induction therapy is to achieve a complete remission by reducing the amount of leukemic cells to an undetectable level; the goal of consolidation therapy is to eliminate any residual undetectable disease and achieve a cure.
In addition, specific treatment plans may be used, depending on the type of leukemia that has been diagnosed. Whatever the plan, it is important for the patient to understand the treatment that is being given and the decision-making process behind the choice.
Acute Myelogenous Leukemia (AML)
It is most common for adults; more men than women are affected. Many different chemotherapeutic plans are available for the treatment of AML. Overall, the strategy is to control bone marrow and systemic (whole-body) disease while offering specific treatment for the central nervous system (CNS), if involved. In general, most oncologists rely on combinations of drugs for the initial, induction phase of chemotherapy. Such combination chemotherapy usually offers the benefits of early remission (lessening of the disease) and a lower risk of disease resistance. Consolidation or "maintenance" treatments may be given to prevent disease recurrence once remission has been achieved. Consolidation treatment often entails a repetition of induction chemotherapy or the intensification chemotherapy with added drugs. By contrast, maintenance treatment involves drug doses that are lower than those administered during the induction phase.
Initial treatment of AML
Initial treatment of AML usually begins with induction chemotherapy using a combination of drugs such as daunorubicin (DNR), cytarabine (ara-C), idarubicin, thioguanine, etoposide, or mitoxantrone, anabolic steroids.
Follow-up treatment
Follow-up therapy for such patients may involve:
- supportive care, such as intravenous nutrition and treatment with oral antibiotics (e.g., ofloxacin, rifampin), especially in patients who have prolonged granulocytopenia; that is too few mature granulocytes (neutrophils), the bacteria-destroying white blood cells that contain small particles, or granules (< 100 granulocytes per cubic millimeter for 2 weeks)
- injection with colony-stimulating factors such as granulocyte colony-stimulating factor (G-CSF), which may help to shorten the period of granulocytopenia that results from induction therapy
- transfusions with red blood cells and platelets
Patients with newly diagnosed disease also may be considered for stem cell transplantation (SCT), either from the bone marrow or other sources. Allogeneic bone marrow transplant (alloBMT) is reserved primarily for patients under 55 years of age who have a compatible family donor. Approximately half of newly diagnosed AML patients are in this age group, with 75% achieving a complete remission (CR) after induction and consolidation therapy. Allogeneic bone marrow transplant is available for about 15% of all patients with AML. Unfortunately, it is estimated that only 7% of all AML patients will be cured using this procedure.
People who receive stem cell transplantation (SCT, alloBMT) require protective isolation in the hospital, including filtered air, sterile food, and sterilization of the microorganisms in the gut, until their total white blood cell (WBC) count is above 500.
Treatment of central nervous system leukemia, if present, may involve injection of chemotherapeutic drugs (e.g., cytarabine or ara-C, methotrexate) into the areas around the brain and spinal cord.
Induction
As of 2006, all FAB subtypes except M3 are usually given induction chemotherapy with cytarabine (ara-C) and an anthracycline (such as daunorubicin or idarubicin).[61] Other alternatives, including high-dose ara-C alone, may also be used.[62][63] Because of the toxic effects of therapy, including myelosuppression and an increased risk of infection, induction chemotherapy may not offered to the very elderly. Induction chemotherapy usually requires a hospitalization of about 1 month to receive the chemotherapy and recover from its side effects.
Induction chemotherapy is known as "7 and 3" because the cytarabine is given as a continuous IV infusion for seven consecutive days, while the anthracycline is given for three consecutive days as an IV push. Up to 70% of patients will achieve a remission with this protocol.[64]
The M3 subtype of AML, also known as acute promyelocytic leukemia, is almost universally treated with the drug ATRA (all-trans-retinoic acid) in addition to induction chemotherapy.[65][66][67] Care must be taken to prevent disseminated intravascular coagulation (DIC), complicating the treatment of APL when the promyelocytes release the contents of their granules into the peripheral circulation. APL is eminently curable with well-documented treatment protocols.
The goal of the induction phase is to reach a complete remission. Complete remission does not mean that the disease has been cured; rather, it signifies that no disease can be detected with available diagnostic methods (i.e., <5% leukemic cells remain in the bone marrow).[61] Complete remission is obtained in about 50%–75% of newly diagnosed adults, although this may vary based on the prognostic factors described above.[68]
The durability of remission depends on the prognostic features of the original leukemia. In general, all remissions will fail without consolidation (post-remission) chemotherapy, and consolidation has become an important component of treatment.[69]
Consolidation
Even after complete remission is achieved, leukemic cells likely remain in numbers too small to be detected with current diagnostic techniques. If no further postremission or consolidation therapy is given, almost all patients will eventually relapse.[70] Therefore, more therapy is necessary to eliminate non-detectable disease and prevent relapse — that is, to achieve a cure.
The specific type of postremission therapy is individualized based on a patient's prognostic factors (see above) and general health. For good-prognosis leukemias (i.e. inv(16), t(8;21), and t(15;17)), patients will typically undergo an additional 3–5 courses of intensive chemotherapy, known as consolidation chemotherapy.[71][72] For patients at high risk of relapse (e.g. those with high-risk cytogenetics, underlying MDS, or therapy-related AML), allogeneic stem cell transplantation is usually recommended if the patient is able to tolerate a transplant and has a suitable donor. The best postremission therapy for intermediate-risk AML (normal cytogenetics or cytogenetic changes not falling into good-risk or high-risk groups) is less clear and depends on the specific situation, including the age and overall health of the patient, the patient's personal values, and whether a suitable stem cell donor is available.[72]
If, however, the AML patient has resistant disease (about 15%) or relapses (about 70%), second remissions sometimes are achieved by treating them with:
- conventional induction chemotherapy
- high-dose ara-C (HDAC), with/without other drugs
- etoposide or other single chemotherapeutic agents
Elderly AML patients have special treatment concerns. They may be less able to tolerate the septicemia (blood poisoning) associated with granulocytopenia, and they often have higher rates of myelodysplastic ('preleukemia') syndrome (MDS). Individuals who are over age 75 or who have significant medical conditions can be treated effectively with low-dose ara-C. High-dose post-induction chemotherapy is unlikely to be tolerated by elderly patients.
Until recently, the treatment plans and responses of children with AML did not differ much from those of adults. Yet new, more intensive induction and consolidation treatments have resulted in higher remission rates and prolonged survivals. Many induction trials have produced good results using combinations of cytarabine (ara-C) plus an anthracycline (e.g., daunorubicin, doxorubicin). In children under 3 years of age, the anthracycline used for induction should be chosen with care, since doxorubicin produces more toxicity and related deaths than daunorubicin.
Consolidation therapy is complex, but it should include at least two courses of high-dose ara-C (HDAC). Children who have hyperleukocytosis (too many white blood cells), especially monocytic M5 leukemia, have a poor prognosis.
Relapsed AML
Despite aggressive therapy, however, only 20%–30% of patients enjoy long-term disease-free survival. For patients with relapsed AML, the only proven potentially curative therapy is a stem cell transplant, if one has not already been performed.[73][74][75] In 2000, Mylotarg (gemtuzumab zogamicin) was approved in the United States for patients aged more than 60 years with relapsed AML who are not candidates for high-dose chemotherapy.[76]
Patients with relapsed AML who are not candidates for stem cell transplantion, or who have relapsed after a stem cell transplant, should be strongly considered for enrollment in a clinical trial, as conventional treatment options are limited. Agents under investigation include cytotoxic drugs such as clofarabine as well as targeted therapies such as farnesyl transferase inhibitors, decitabine, and inhibitors of MDR1 (multidrug-resistance protein). Since treatment options for relapsed AML are so limited, another option which may be offered is palliative care.
For relapsed acute promyelocytic leukemia (APL), arsenic trioxide has been tested in trials and approved by the Food and Drug Administration. Like ATRA, arsenic trioxide does not work with other subtypes of AML.[77]
See also
Further reading
- Martin Abeloff (2004). Clinical Oncology (3rd. edition ed.). St. Louis, Mo.: Elsevier Churchill Livingstone. ISBN 0-443-06629-9. Unknown parameter
|coauthors=ignored (help) - Ronald Hoffman (2005). Hematology: Basic Principles and Practice (4th. edition ed.). St. Louis, Mo.: Elsevier Churchill Livingstone. ISBN 0-443-06629-9. Unknown parameter
|coauthors=ignored (help)
References
- ↑ 1.0 1.1 1.2 Jemal A, Thomas A, Murray T, Thun M. Cancer statistics 2002. CA Cancer J Clin 52:23, 2002. PMID 11814064
- ↑ Hoffman, Ronald; et al. (2005). Hematology: Basic Principles and Practice (4th. ed. ed.). St. Louis, Mo.: Elsevier Churchill Livingstone. pp. p. 1071. ISBN 0-443-06629-9.
- ↑ Bennett JH. Two cases of hypertrophy of the spleen and liver, in which death took place from suppuration of blood. Edinburgh Med Surg J. (1845)64:413.
- ↑ Virchow R: Die Leukämie. In Virchow R (ed): Gesammelte Abhandlungen zur Wissenschaftlichen Medizin. Frankfurt, Meidinger, 1856, p 190.
- ↑ Ebstein W. Ueber die acute Leukämie und Pseudoleukämie. Deutsch Arch Klin Med. (1889)44:343.
- ↑ Mosler F. Klinische Symptome und Therapie der medullären Leukämie. Berl Klin Wochenschr. (1876)13:702.
- ↑ Naegeli O. Über rothes Knochenmark und Myeloblasten. Deutsch Med Wochenschr. (1900) 26:287.
- ↑ Zhen-yi, Wang (2003). "Ham-Wasserman Lecture: Treatment of Acute Leukemia by Inducing Differentiation and Apoptosis". Hematology. PMID 14633774.
- ↑ 9.0 9.1 9.2 9.3 Hoffman, Ronald et al. (2005), pp. 1074–75.
- ↑ Abeloff, Martin; et al. (2004). Clinical Oncology (3rd. edition ed.). St. Louis, Mo.: Elsevier Churchill Livingstone. pp. p. 2834. ISBN 0-443-06629-9.
- ↑ Sanz G, Sanz M, Vallespí T, Cañizo M, Torrabadella M, García S, Irriguible D, San Miguel J (1989). "Two regression models and a scoring system for predicting survival and planning treatment in myelodysplastic syndromes: a multivariate analysis of prognostic factors in 370 patients". Blood. 74 (1): 395–408. PMID 2752119.
- ↑ Le Beau M, Albain K, Larson R, Vardiman J, Davis E, Blough R, Golomb H, Rowley J (1986). "Clinical and cytogenetic correlations in 63 patients with therapy-related myelodysplastic syndromes and acute nonlymphocytic leukemia: further evidence for characteristic abnormalities of chromosomes no. 5 and 7". J Clin Oncol. 4 (3): 325–45. PMID 3950675.
- ↑ Thirman M, Gill H, Burnett R, Mbangkollo D, McCabe N, Kobayashi H, Ziemin-van der Poel S, Kaneko Y, Morgan R, Sandberg A (1993). "Rearrangement of the MLL gene in acute lymphoblastic and acute myeloid leukemias with 11q23 chromosomal translocations". N Engl J Med. 329 (13): 909–14. PMID 8361504.
- ↑ Bizzozero O, Johnson K, Ciocco A (1966). "Radiation-related leukemia in Hiroshima and Nagasaki, 1946–1964. I. Distribution, incidence and appearance time". N Engl J Med. 274 (20): 1095–101. PMID 5932020.
- ↑ Yoshinaga S, Mabuchi K, Sigurdson A, Doody M, Ron E (2004). "Cancer risks among radiologists and radiologic technologists: review of epidemiologic studies". Radiology. 233 (2): 313–21. PMID 15375227.
- ↑ Austin H, Delzell E, Cole P (1988). "Benzene and leukemia. A review of the literature and a risk assessment". Am J Epidemiol. 127 (3): 419–39. PMID 3277397.
- ↑ Linet, MS. The Leukemias: Epidemiologic Aspects. Oxford University Press, New York 1985.
- ↑ Evans D, Steward J (1972). "Down's syndrome and leukaemia". Lancet. 2 (7790): 1322. PMID 4117858.
- ↑ Leone G, Mele L, Pulsoni A, et al: The incidence of secondary leukemias. Haematologica 84:937, 1999. PMID 10509043
- ↑ Greenlee RT, Hill-Harmon MB, Murray T, et al: Cancer statistics, 2001 erratum appears in CA Cancer J Clin 2001 Mar-Apr;51(2):144. CA Cancer J Clin 2001;51:15–36. PMID 11577478
- ↑ Linet MS: The leukemias: Epidemiologic aspects. In Lilienfeld AM (ed): Monographs in Epidemiology and Biostatistics. New York, Oxford University Press, 1985, p I.
- ↑ Aoki K, Kurihars M, Hayakawa N, et al: Death Rates for Malignant Neoplasms for Selected Sites by Sex and Five-Year Age Group in 33 Countries 1953–57 to 1983–87. Nagoya, Japan, University of Nagoya Press, International Union Against Cancer, 1992.
- ↑ Bhatia S, Neglia JP: Epidemiology of childhood acute myelogenous leukemia. J Pediatr Hematol Oncol 17:94, 1995. PMID 7749772
- ↑ Taylor GM, Birch JM: The hereditary basis of human leukemia. In Henderson ES, Lister TA, Greaves MF (eds): Leukemia, 6th ed. Philadelphia, WB Saunders, 1996, p 210.
- ↑ Horwitz M, Goode EL, Jarvik GP: Anticipation in familial leukemia. Am J Hum Genet 59:990, 1996. PMID 8900225
- ↑ Crittenden LB: An interpretation of familial aggregation based on multiple genetic and environmental factors. Ann N Y Acad Sci 91:764, 1978. PMID 13696504
- ↑ Horowitz M: The genetics of familial leukemia. Leukemia 11:1345, 1997
- ↑ Gunz FW, Veale AM: Leukemia in close relatives: Accident or predisposition. J Natl Cancer Inst 42:517, 1969. PMID 4180615
- ↑ Fialkow PJ: Clonal origin of human tumors. Biochim Biophys Acta 1976;458:283–321. PMID 1067873
- ↑ Fialkow PJ, Janssen JW, Bartram CR: Clonal remissions in acute nonlymphocytic leukemia: Evidence for a multistep pathogenesis of the malignancy. Blood 1991;77:1415–1517. PMID 2009365
- ↑ Bonnet D, Dick JE: Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med 1997;3:730–737. PMID 9212098
- ↑ Abeloff, Martin et al. (2004), pp. 2831–32.
- ↑ Greer, John P., et al. Wintrobe's Clinical Hematology, 11th ed. Philadelphia: Lippincott, Williams, and Wilkins, 2004. p. 2045–2062
- ↑ Melnick A, Licht JD. Deconstructing a disease: RARα its fusion partners, and their roles in the pathogenesis of acute promyelocytic leukemia. Blood 1999;93:3167–3215. PMID 10233871
- ↑ Abeloff, Martin et al. (2004), p. 2828.
- ↑ Abeloff, Martin et al. (2004), p. 2834.
- ↑ Abeloff, Martin et al. (2004), p. 2835.
- ↑ Harris N, Jaffe E, Diebold J, Flandrin G, Muller-Hermelink H, Vardiman J, Lister T, Bloomfield C (1999). "The World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues. Report of the Clinical Advisory Committee meeting, Airlie House, Virginia, November, 1997". Ann Oncol. 10 (12): 1419–32. PMID 10643532.
- ↑ Grimwade D, Howe K, Langabeer S, Davies L, Oliver F, Walker H, Swirsky D, Wheatley K, Goldstone A, Burnett A, Solomon E (1996). "Establishing the presence of the t(15;17) in suspected acute promyelocytic leukaemia: cytogenetic, molecular and PML immunofluorescence assessment of patients entered into the M.R.C. ATRA trial. M.R.C. Adult Leukaemia Working Party". Br J Haematol. 94 (3): 557–73. PMID 8790159.
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ Bennett J, Catovsky D, Daniel M, Flandrin G, Galton D, Gralnick H, Sultan C (1976). "Proposals for the classification of the acute leukaemias. French-American-British (FAB) co-operative group". Br J Haematol. 33 (4): 451–8. PMID 188440.
- ↑ Vardiman J, Harris N, Brunning R (2002). "The World Health Organization (WHO) classification of the myeloid neoplasms". Blood. 100 (7): 2292–302. PMID 12239137. Full text.
- ↑ Estey E (2001). "Prognostic factors in acute myelogenous leukemia". Leukemia. 15 (4): 670–2. PMID 11368376.
- ↑ Wheatley K, Burnett A, Goldstone A, Gray R, Hann I, Harrison C, Rees J, Stevens R, Walker H (1999). "A simple, robust, validated and highly predictive index for the determination of risk-directed therapy in acute myeloid leukaemia derived from the MRC AML 10 trial. United Kingdom Medical Research Council's Adult and Childhood Leukaemia Working Parties". Br J Haematol. 107 (1): 69–79. PMID 10520026.
- ↑ Slovak M, Kopecky K, Cassileth P, Harrington D, Theil K, Mohamed A, Paietta E, Willman C, Head D, Rowe J, Forman S, Appelbaum F (2000). "Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group Study". Blood. 96 (13): 4075–83. PMID 11110676.
- ↑ Byrd J, Mrózek K, Dodge R, Carroll A, Edwards C, Arthur D, Pettenati M, Patil S, Rao K, Watson M, Koduru P, Moore J, Stone R, Mayer R, Feldman E, Davey F, Schiffer C, Larson R, Bloomfield C (2002). "Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461)". Blood. 100 (13): 4325–36. PMID 12393746.
- ↑ Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G, Rees J, Hann I, Stevens R, Burnett A, Goldstone A. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood. 1998 Oct 1;92(7):2322–33.
- ↑ Slovak ML; Kopecky KJ; Cassileth PA; Harrington DH; Theil KS; Mohamed A; Paietta E; Willman CL; Head DR; Rowe JM; Forman SJ; Appelbaum FR Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group Study. Blood 2000 Dec 15;96(13):4075–83.
- ↑ Byrd J, Mrózek K, Dodge R, Carroll A, Edwards C, Arthur D, Pettenati M, Patil S, Rao K, Watson M, Koduru P, Moore J, Stone R, Mayer R, Feldman E, Davey F, Schiffer C, Larson R, Bloomfield C (2002). "Pretreatment cytogenetic abnormalities are predictive of induction success, cumulative incidence of relapse, and overall survival in adult patients with de novo acute myeloid leukemia: results from Cancer and Leukemia Group B (CALGB 8461)". Blood. 100 (13): 4325–36. PMID 12393746.
- ↑ Thirman M, Larson R (1996). "Therapy-related myeloid leukemia". Hematol Oncol Clin North Am. 10 (2): 293–320. PMID 8707757.
- ↑ Rowley J, Golomb H, Vardiman J (1981). "Nonrandom chromosome abnormalities in acute leukemia and dysmyelopoietic syndromes in patients with previously treated malignant disease". Blood. 58 (4): 759–67. PMID 7272506.
- ↑ Pedersen-Bjergaard J, Andersen M, Christiansen D, Nerlov C (2002). "Genetic pathways in therapy-related myelodysplasia and acute myeloid leukemia". Blood. 99 (6): 1909–12. PMID 11877259.
- ↑ Haferlach T, Schoch C, Löffler H, Gassmann W, Kern W, Schnittger S, Fonatsch C, Ludwig W, Wuchter C, Schlegelberger B, Staib P, Reichle A, Kubica U, Eimermacher H, Balleisen L, Grüneisen A, Haase D, Aul C, Karow J, Lengfelder E, Wörmann B, Heinecke A, Sauerland M, Büchner T, Hiddemann W (2003). "Morphologic dysplasia in de novo acute myeloid leukemia (AML) is related to unfavorable cytogenetics but has no independent prognostic relevance under the conditions of intensive induction therapy: results of a multiparameter analysis from the German AML Cooperative Group studies". J Clin Oncol. 21 (2): 256–65. PMID 12525517.
- ↑ Schnittger S, Schoch C, Dugas M, Kern W, Staib P, Wuchter C, Löffler H, Sauerland C, Serve H, Büchner T, Haferlach T, Hiddemann W (2002). "Analysis of FLT3 length mutations in 1003 patients with acute myeloid leukemia: correlation to cytogenetics, FAB subtype, and prognosis in the AMLCG study and usefulness as a marker for the detection of minimal residual disease". Blood. 100 (1): 59–66. PMID 12070009.
- ↑ Gale R, Hills R, Kottaridis P, Srirangan S, Wheatley K, Burnett A, Linch D (2005). "No evidence that FLT3 status should be considered as an indicator for transplantation in acute myeloid leukemia (AML): an analysis of 1135 patients, excluding acute promyelocytic leukemia, from the UK MRC AML10 and 12 trials". Blood. 106 (10): 3658–65. PMID 16076872.
- ↑ Paschka P, Marcucci G, Ruppert A, Mrózek K, Chen H, Kittles R, Vukosavljevic T, Perrotti D, Vardiman J, Carroll A, Kolitz J, Larson R, Bloomfield C (2006). "Adverse prognostic significance of KIT mutations in adult acute myeloid leukemia with inv(16) and t(8;21): a Cancer and Leukemia Group B Study". J Clin Oncol. 24 (24): 3904–11. PMID 16921041.
- ↑ Cassileth P, Harrington D, Appelbaum F, Lazarus H, Rowe J, Paietta E, Willman C, Hurd D, Bennett J, Blume K, Head D, Wiernik P (1998). "Chemotherapy compared with autologous or allogeneic bone marrow transplantation in the management of acute myeloid leukemia in first remission". N Engl J Med. 339 (23): 1649–56. PMID 9834301.
- ↑ Matthews J, Bishop J, Young G, Juneja S, Lowenthal R, Garson O, Cobcroft R, Dodds A, Enno A, Gillett E, Hermann R, Joshua D, Ma D, Szer J, Taylor K, Wolf M, Bradstock K (2001). "Patterns of failure with increasing intensification of induction chemotherapy for acute myeloid leukaemia". Br J Haematol. 113 (3): 727–36. PMID 11380464.
- ↑ Sanz M, Lo Coco F, Martín G, Avvisati G, Rayón C, Barbui T, Díaz-Mediavilla J, Fioritoni G, González J, Liso V, Esteve J, Ferrara F, Bolufer P, Bernasconi C, Gonzalez M, Rodeghiero F, Colomer D, Petti M, Ribera J, Mandelli F (2000). "Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups". Blood. 96 (4): 1247–53. PMID 10942364.
- ↑ 61.0 61.1 Abeloff, Martin et al. (2004), pp. 2835–39.
- ↑ Weick JK, Kopecky KJ, Appelbaum FR, et al: A randomized investigation of high-dose versus standard-dose cytosine arabinoside with daunorubicin in patients with previously untreated acute myeloid leukemia: A Southwest Oncology Group Study. Blood 1996;88:2841–2851. PMID 8874180
- ↑ Bishop JF, Matthews JP, Young GA, et al: A randomized study of high-dose cytarabine in induction in acute myeloid leukemia. Blood 1996;87:1710–1717. PMID 8634416
- ↑ Bishop J (1997). "The treatment of adult acute myeloid leukemia". Semin Oncol. 24 (1): 57–69. PMID 9045305.
- ↑ Huang ME, Ye YC, Chen SR, et al: Use of all-trans retinoic acid in the treatment of acute promyelocytic leukemia. Blood 1988;72:567–572. PMID 3165295
- ↑ Tallman MS, Anderson JW, Schiffer CA, et al: All-trans-retinoic acid in acute promyelocytic leukemia. N Engl J Med 1997;337:1021–1028. PMID 9321529
- ↑ Fenaux P, Chastang C, Chevret S, et al: A randomized comparison of all transretinoic acid (ATRA) followed by chemotherapy and ATRA plus chemotherapy and the role of maintenance therapy in newly diagnosed acute promyelocytic leukemia. The European APL Group. Blood 1999;94:1192–1200. PMID 10438706
- ↑ Estey E (2002). "Treatment of acute myelogenous leukemia". Oncology (Williston Park). 16 (3): 343–52, 355–6, discussion 357, 362, 365–6. PMID 15046392.
- ↑ Cassileth P, Harrington D, Hines J, Oken M, Mazza J, McGlave P, Bennett J, O'Connell M (1988). "Maintenance chemotherapy prolongs remission duration in adult acute nonlymphocytic leukemia". J Clin Oncol. 6 (4): 583–7. PMID 3282032.
- ↑ Cassileth PA, Hines JD, Oken MM, et al: Maintenance chemotherapy prolongs remission duration in adult acute nonlymphocytic leukemia. J Clin Oncol 1988;6(4):583–587. PMID 3282032
- ↑ Mayer RJ, Davis RB, Schiffer CA, et al: Intensive post-remission chemotherapy in adults with acute myeloid leukemia. N Engl J Med 1994;331:896–903. PMID 8078551
- ↑ 72.0 72.1 O'Donnell MR, Appelbaum FR, Baer MR, et al: NCCN practice guidelines for acute myelogenous leukemia. Oncology NCCN Proc 2000;14:53–61. PMID 11195419
- ↑ Abeloff, Martin et al. (2004), pp. 2840–41.
- ↑ Appelbaum FR: Who should be transplanted for AML? editorial. Leukemia 2001;15:680–682. PMID 11368380
- ↑ Appelbaum FR: Hematopoietic cell transplantation beyond first remission keynote Address. Leukemia 2002;16:157–159. PMID 11840278
- ↑ Sievers EL, Larson RA, Stadmauer EA, et al: Efficacy and safety of gemtuzumab ozogamicin in patients with CD33-positive acute myeloid leukemia in first relapse. J Clin Oncol 2001;19:3244–3254. PMID 11432892
- ↑ Soignet SL, Frankel SR, Douer D, et al: United States multicenter study of arsenic trioxide in relapsed acute promyelocytic leukemia. J Clin Oncol 2001;19:3852–3860. PMID 11559723
External links
- Atlas of Hematology
- American Cancer Society page on Acute Myeloid Leukemia
- Association of Cancer Online Resource (ACOR) Leukemia Links
- Leukemia & Lymphoma Society page on Acute Myeloid Leukemia
- Childhood Acute Myeloid Leukemia
- National Marrow Donor Program
- Blood & Marrow Transplant Information Network
- National Cancer Institute (NCI) PDQ statement on AML for health professionals
ar:ابيضاض الدم النقوي الحاد de:Akute myeloische Leukämie he:לוקמיה מיאלואידית חריפה sr:Акутна мијелоцитна леукемија sv:Akut myeloisk leukemi