Meningitis pathophysiology: Difference between revisions
No edit summary |
No edit summary |
||
| Line 86: | Line 86: | ||
[[Category:Needs overview]] | [[Category:Needs overview]] | ||
[[Category:Primary care]] | |||
[[Category:Disease]] | [[Category:Disease]] | ||
[[Category:Infectious disease]] | [[Category:Infectious disease]] | ||
[[Category:Neurology]] | [[Category:Neurology]] | ||
[[Category:Emergency medicine]] | [[Category:Emergency medicine]] | ||
[[Category:Diseases involving the fasciae]] | |||
[[Category:Inflammations]] | |||
[[Category:Neurological disorders]] | [[Category:Neurological disorders]] | ||
Revision as of 15:34, 14 February 2013
|
Meningitis Main Page |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Pathophysiology
The clinical picture of meningitis largely arises from the host response to the inciting organism in the CSF.
- It seems that the subcapsular components (the cell wall and lipopolysaccharide) of bacteria are more important in determining inflammation than the surface components (pili and polysaccharide capsule).
- The primary site of breakdown of the blood-brain barrier is the cerebral microvascular endothelium.
- Electron microscope (EM) studies have shown complete separation of the intercellular tight junctions
- It appears that there is a final common pathway, mediated by TNF-alpha, IL-1 and IL-6, that results in meningeal inflammation and loss of the blood-brain barrier.
- One of the major roles of these cytokines is to facilitate the migration of neutrophils across the vascular endothelium into the CSF.
- A key initial step in this process is obviously adhesion of the PMN to the endothelial surface.
- This is mediated by the expression of specific transmembrane glycoproteins expressed on the endothelial surface that interact with specific counterparts on the neutrophils.
- These adhesion molecules fall into three large categories: the immunoglobin superfamily (including the antigen-specific T and B cell receptors, ICAM-1 and ICAM-2), the integrin family (beta-1, beta-2, and beta-3) and the selectin family (including ELAM-1).
- The interaction of beta-2 integrin (CD18) and ICAM-1 is largely responsible for PMN diapedesis.
- Additionally, patients get cerebral edema that is mediated by an increase in capillary permeability, the inflammatory response from the neutrophils, and CSF outflow resistance.
- The above pathophysiologic processes are not only important in producing the symptoms associated with meningitis, but the understanding of the underlying disease process is necessary to guide therapy (see below).
Mechanism
- In order to gain access to the CNS, the pathogen needs to colonize mucosal epithelium, invade and survive in the intravascular space, cross the blood-brain barrier and survive in the CSF.
- Colonization of the nasopharynx is usually asymptomatic, and during peak seasons, approximately 20% of the population are colonized with N. meningitidis.
Gross Pathology
Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-

Meningitis: Gross, purulent leptomeningitis due to pneumococcus infection, an excellent example.
-
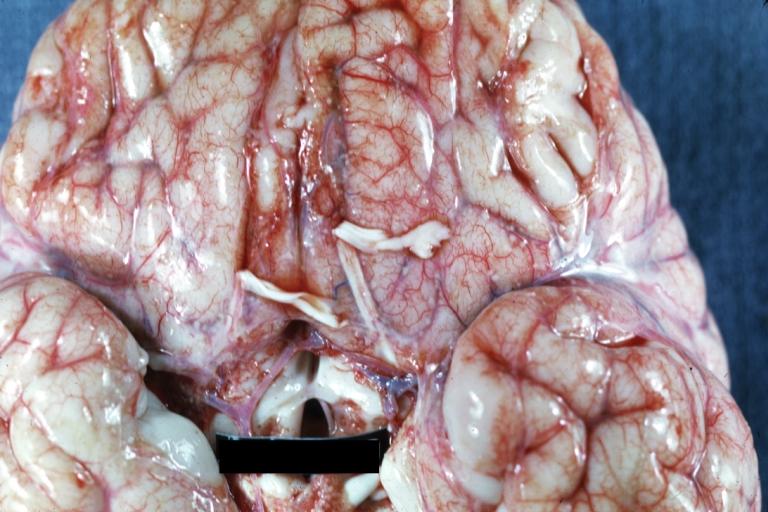
Bacterial Meningitis: Gross, basilar view


-
Bacterial Meningitis: Gross close-up
-
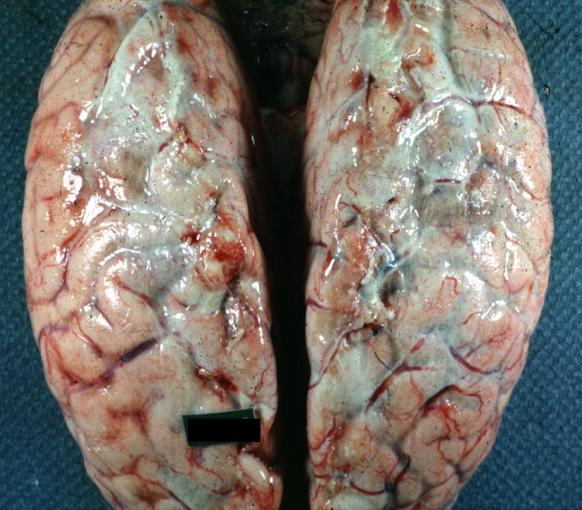
Meningitis: Gross base of frontal lobes well shown meningitis burn case with Pseudomonas sepsis


-
Meningitis: Gross natural color excellent demonstration of greenish pus in subarachnoid space
-
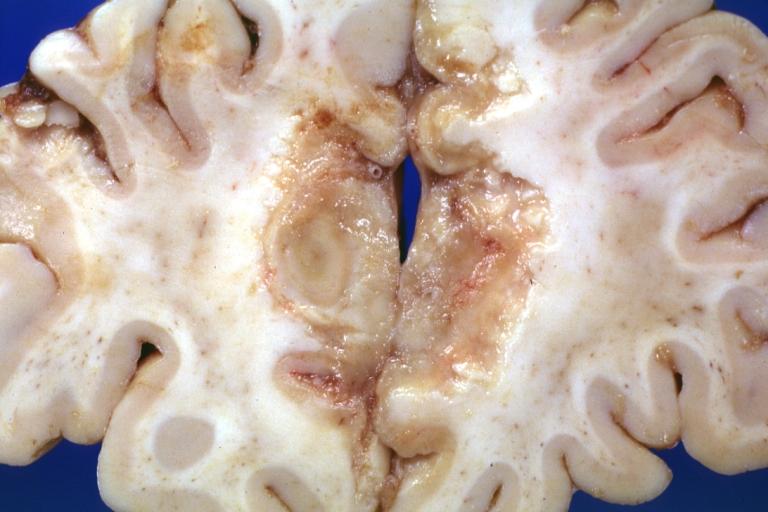
Tuberculous Meningitis: Gross fixed tissue close-up of large areas of necrosis in frontal parasagittal cortex secondary to tuberculous vasculitis. An excellent example


-
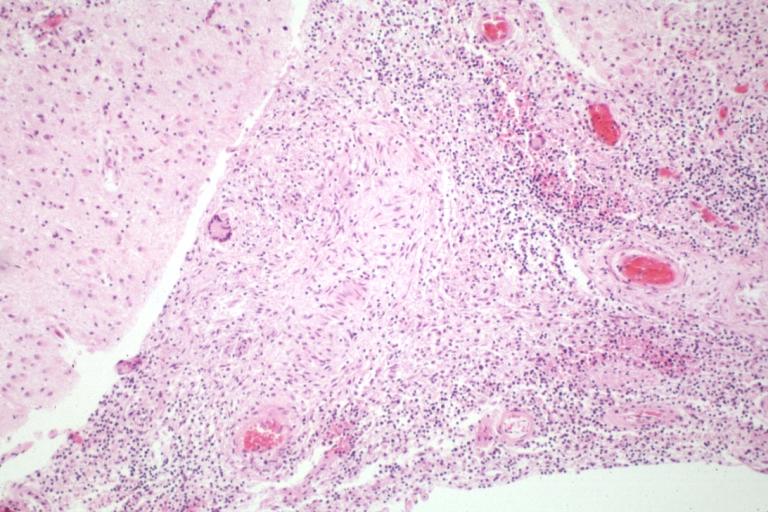
Tuberculous Meningitis: Micro low mag H&E. An excellent example with giant cells.
-
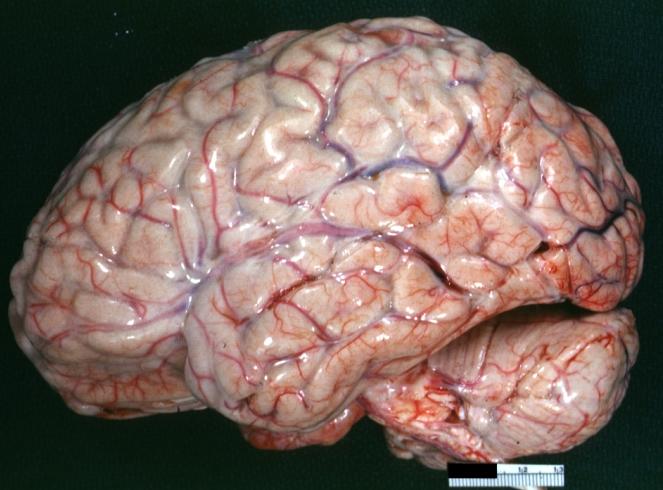
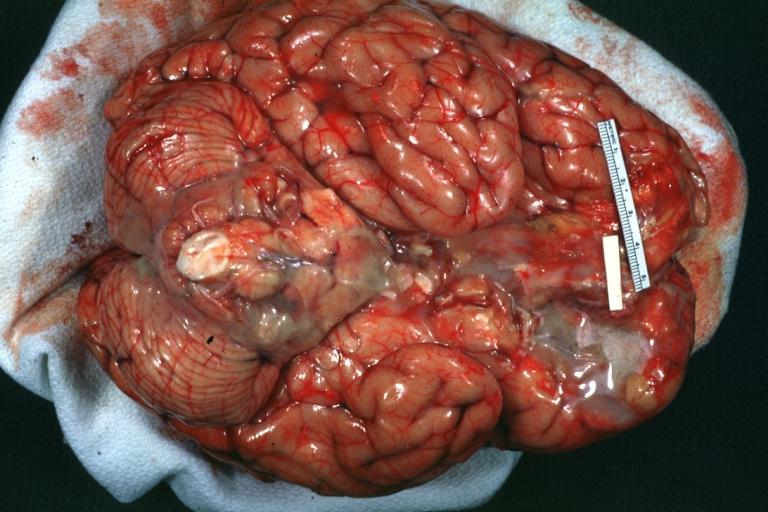
Purulent Meningitis: Gross natural color excellent photo lateral aspect of brain with easily seen purulent exudate due to Pneumococcus infection.


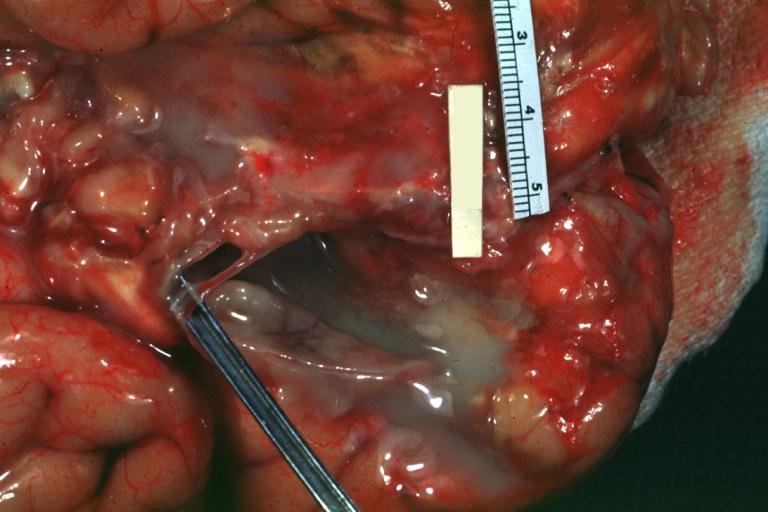
-

Purulent Meningitis: Gross natural color close-up view outstanding example of purulent exudate adjacent to blood vessels
-

Purulent Meningitis: Gross natural color Staphylococcal meningitis.


-
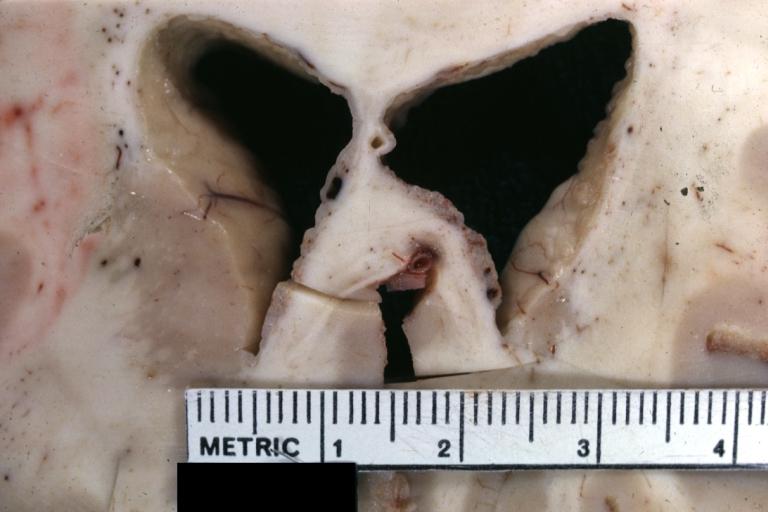
Ependymitis Granular Neoplastic: Gross fixed tissue close-up view and a spectacular one of this lesion case also has carcinomatous meningitis primary is lung oat cell.
-

Purulent Meningitis: Gross natural color brain in situ with removed calvarium very good illustration of exudate in meninges over convexities pneumococcus.


Microscopic Pathology
{{#ev:youtube|L9jpjxTSLws}}