Adenomyosis: Difference between revisions
No edit summary |
|||
| (89 intermediate revisions by 6 users not shown) | |||
| Line 1: | Line 1: | ||
'''For patient information, click [[Adenomyosis (patient information)|here]]''' | |||
{{DiseaseDisorder infobox | | {{DiseaseDisorder infobox | | ||
Name = Adenomyosis | | Name = Adenomyosis | | ||
| Line 4: | Line 6: | ||
ICD9 = {{ICD9|617.0}} | | ICD9 = {{ICD9|617.0}} | | ||
ICDO = | | ICDO = | | ||
Image = | | Image = Adenomyosis MRI 105.jpg| | ||
Caption = | | Caption = MRI, T2: Adenomyosis. <br> [http://www.radswiki.net Image courtesy of RadsWiki]| | ||
OMIM = 600458 | | OMIM = 600458 | | ||
MedlinePlus = 001513 | | MedlinePlus = 001513 | | ||
eMedicineSubj = | eMedicineSubj = | | ||
eMedicineTopic = | eMedicineTopic = | | ||
DiseasesDB = | DiseasesDB = | | ||
MeshID = D004715 | | MeshID = D004715 | | ||
}} | }} | ||
{{SI}} | {{SI}} | ||
{{CMG}} | {{CMG}}; '''Associate Editor(s)-In-Chief:''' [[User:Zorkun|Cafer Zorkun M.D. PhD.]][mailto:czorkun@wikidoc.org], [[User:Dina|Dina Elantably, MD]][mailto:dina.antably@gmail.com] | ||
==[[Overview]]== | |||
[[Adenomyosis]] is a medical condition characterized by the presence of ectopic [[endometrium|endometrial tissue]] (the inner lining of the [[uterus]]) within the [[uterus|myometrium]] (the thick, muscular layer of the uterus). The condition is typically found in women between the ages between 35 and 50. Patients with adenomyosis can have painful and/or profuse [[menses]] ([[dysmenorrhea]] & [[menorrhagia]], respectively). | |||
Adenomyosis may involve the uterus focally, creating an [[adenomyoma]], or diffusely. With diffuse involvement, the uterus becomes bulky and heavier. | |||
{{ | ==[[Historical Perspective]]== | ||
*[[Adenomyosis]] was first discovered by '''Carl von Rokitansky''', a German pathologist, in '''1860''' when he found endometrial glands in the myometrium and designated this finding as 'cystosarcoma adenoids uterinum'<ref name="pmid16515887">{{cite journal| author=Benagiano G, Brosens I| title=History of adenomyosis. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 449-63 | pmid=16515887 | doi=10.1016/j.bpobgyn.2006.01.007 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16515887 }} </ref>. <br> | |||
* In '''1892''' the first systematic investigation of [[adenomyosis]] was carried out by ''''Thomas Stephen Cullen'''', a gynecologist. He distinguished 3 types of [[adenomyoma]]: intramural, subperitoneal and submucous [[adenomyoma]]<ref name="pmid16515887">{{cite journal| author=Benagiano G, Brosens I| title=History of adenomyosis. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 449-63 | pmid=16515887 | doi=10.1016/j.bpobgyn.2006.01.007 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16515887 }} </ref>. | |||
*In '''1893''', '''Kelly and Cullen''' described the [[pathogenesis]] of [[adenomyoma]]. The 'gradual ascendancy of Cullen’s mucosal theory' stated that [[endometrium]] invades the inner [[myometrium]] through the presence in it of ‘chinks’, or fissures. | |||
*In '''1892''', '''Cullen''' described that abdominal [[hysterectomy]] is indicated for [[treatment]] as the [[endometrial]] growths are interwoven with the normal muscle of the [[uterus]]. | |||
== | ==[[Classification]]== | ||
*Adenomyosis can be classified according to its [[histopathology]] into 2 groups: | |||
:*'''Diffuse adenomyosis:''' Uniformly enlarged boggy [[uterus]]. | |||
:*'''Focal adenomyosis [[(adenomyoma)]]:''' Grossly it resembles [[fibroid]] but without a surrounding pseudocapsule. | |||
''' | *Other variants of adenomyosis include '''juvenile cystic adenomyosis'''; which is the presence of [[endometrial]] cysts > 1cm in diameter within the [[myometrium]]. It is usually seen in young women <30 years old <ref name="pmid19539912">{{cite journal| author=Takeuchi H, Kitade M, Kikuchi I, Kumakiri J, Kuroda K, Jinushi M| title=Diagnosis, laparoscopic management, and histopathologic findings of juvenile cystic adenomyoma: a review of nine cases. | journal=Fertil Steril | year= 2010 | volume= 94 | issue= 3 | pages= 862-8 | pmid=19539912 | doi=10.1016/j.fertnstert.2009.05.010 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19539912 }} </ref>. | ||
The | ==[[Pathophysiology]]== | ||
*The pathogenesis of [[Adenomyosis]] is poorly understood. There two theories that explain the possible [[pathogenesis]]<ref name="pmid9825847">{{cite journal| author=Ferenczy A| title=Pathophysiology of adenomyosis. | journal=Hum Reprod Update | year= 1998 | volume= 4 | issue= 4 | pages= 312-22 | pmid=9825847 | doi=10.1093/humupd/4.4.312 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=9825847 }} </ref>: | |||
# Endomyometrial invagination of the [[endometrium]]; due to weakness of the uterine [[smooth muscles]]. | |||
# De novo development of adenomyosis from [[mullerian]] rests due to metaplasia. | |||
*The '''basic Fibroblast Growth Factor (bFGF)''' receptor/ligand system has shown to be upregulated in adenomyosis which explain the abnormal [[uterine bleeding]] and [[menorrhagia]]<ref name="pmid11528364">{{cite journal| author=Propst AM, Quade BJ, Gargiulo AR, Nowak RA, Stewart EA| title=Adenomyosis demonstrates increased expression of the basic fibroblast growth factor receptor/ligand system compared with autologous endometrium. | journal=Menopause | year= 2001 | volume= 8 | issue= 5 | pages= 368-71 | pmid=11528364 | doi=10.1097/00042192-200109000-00012 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11528364 }} </ref>. | |||
* [[Estrogen]] and [[progesterone]] hormones play a role in the [[pathogenesis]] of adenomyosis<ref name="pmid15816354">{{cite journal| author=Green AR, Styles JA, Parrott EL, Gray D, Edwards RE, Smith AG | display-authors=etal| title=Neonatal tamoxifen treatment of mice leads to adenomyosis but not uterine cancer. | journal=Exp Toxicol Pathol | year= 2005 | volume= 56 | issue= 4-5 | pages= 255-63 | pmid=15816354 | doi=10.1016/j.etp.2004.10.001 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15816354 }} </ref>. Other hormones such as [[oxytocin]] <ref name="pmid22999795">{{cite journal| author=Guo SW, Mao X, Ma Q, Liu X| title=Dysmenorrhea and its severity are associated with increased uterine contractility and overexpression of oxytocin receptor (OTR) in women with symptomatic adenomyosis. | journal=Fertil Steril | year= 2013 | volume= 99 | issue= 1 | pages= 231-240 | pmid=22999795 | doi=10.1016/j.fertnstert.2012.08.038 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22999795 }} </ref>, [[FSH]]<ref name="pmid11750866">{{cite journal| author=Stewart EA| title=Gonadotropins and the uterus: is there a gonad-independent pathway? | journal=J Soc Gynecol Investig | year= 2001 | volume= 8 | issue= 6 | pages= 319-26 | pmid=11750866 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11750866 }} </ref>, and [[prolactin]]<ref name="pmid1853904">{{cite journal| author=Mori T, Singtripop T, Kawashima S| title=Animal model of uterine adenomyosis: is prolactin a potent inducer of adenomyosis in mice? | journal=Am J Obstet Gynecol | year= 1991 | volume= 165 | issue= 1 | pages= 232-4 | pmid=1853904 | doi=10.1016/0002-9378(91)90258-s | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1853904 }} </ref> also contribute to the pathogenesis of the disease. | |||
*On gross [[pathology]], there is a globular enlargement of the [[myometrium]] of the [[uterus]] showing cysts filled with hemolysed [[red blood cells]] and [[sideroblasts]]<ref name="pmid16563870">{{cite journal| author=Bergeron C, Amant F, Ferenczy A| title=Pathology and physiopathology of adenomyosis. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 511-21 | pmid=16563870 | doi=10.1016/j.bpobgyn.2006.01.016 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16563870 }} </ref>. | |||
*On microscopic histopathological analysis, there are [[endometrial]] glands, and stroma surrounded by hypertrophic smooth muscle bundles haphazardly scattered within the [[myometrium]]<ref name="pmid16563870">{{cite journal| author=Bergeron C, Amant F, Ferenczy A| title=Pathology and physiopathology of adenomyosis. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 511-21 | pmid=16563870 | doi=10.1016/j.bpobgyn.2006.01.016 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16563870 }} </ref>. | |||
{{#ev:youtube|nOCtpIwCZ-Y}} | |||
==[[Causes]]== | |||
The cause of adenomyosis is unknown, although it has been associated with any sort of uterine trauma that may break the barrier between the endometrium and myometrium, such as: | |||
* [[Caesarean section]] | |||
* [[Tubal ligation]] | |||
* [[Abortion]] | |||
* [[Pregnancy]] | |||
==[[Differentiating adenomyosis from other Diseases]]== | |||
For further information about the differential diagnosis, click [[Adenomyosis differential diagnosis|here]]. | |||
==[[Epidemiology and Demographics]]== | |||
* It is generally estimated that [[adenomyosis]] is present in 20-35% of women<ref name="pmid16563868">{{cite journal| author=Vercellini P, Viganò P, Somigliana E, Daguati R, Abbiati A, Fedele L| title=Adenomyosis: epidemiological factors. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 465-77 | pmid=16563868 | doi=10.1016/j.bpobgyn.2006.01.017 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16563868 }} </ref>. | |||
* The [[incidence]] and [[prevalence]] of adenomyosis are, however, difficult to be accurately estimated and biased by studying only women undergoing [[hysterectomy]], so the total population of women having the disease is not known<ref name="pmid27810281">{{cite journal| author=Abbott JA| title=Adenomyosis and Abnormal Uterine Bleeding (AUB-A)-Pathogenesis, diagnosis, and management. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2017 | volume= 40 | issue= | pages= 68-81 | pmid=27810281 | doi=10.1016/j.bpobgyn.2016.09.006 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27810281 }} </ref>. | |||
===Age=== | |||
*[[Adenomyosis]] is more commonly observed among women aged 40-50 years in those undergoing [[hysterectomy]] for diagnosis<ref name="pmid16563870">{{cite journal| author=Bergeron C, Amant F, Ferenczy A| title=Pathology and physiopathology of adenomyosis. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 511-21 | pmid=16563870 | doi=10.1016/j.bpobgyn.2006.01.016 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16563870 }} </ref>. | |||
*[[Adenomyosis]] is less commonly diagnosed in adolescents who undergo pelvic imaging by [[transvaginal ultrasound]] or [[MRI]] rather than a [[hysterectomy]] for [[diagnosis]]<ref name="pmid16782099">{{cite journal| author=Parker JD, Leondires M, Sinaii N, Premkumar A, Nieman LK, Stratton P| title=Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis. | journal=Fertil Steril | year= 2006 | volume= 86 | issue= 3 | pages= 711-5 | pmid=16782099 | doi=10.1016/j.fertnstert.2006.01.030 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16782099 }} </ref>. | |||
===Race=== | |||
*There is no racial predilection for adenomyosis. | |||
* Almost all cases of adenomyosis present in multiparous women, however there is no clear causal relationship between multiparty and the development of the disease<ref name="pmid16563870">{{cite journal| author=Bergeron C, Amant F, Ferenczy A| title=Pathology and physiopathology of adenomyosis. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2006 | volume= 20 | issue= 4 | pages= 511-21 | pmid=16563870 | doi=10.1016/j.bpobgyn.2006.01.016 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16563870 }} </ref> | |||
== | ==[[Risk Factors]]== | ||
*Similar to the [[epidemiology]], the risk factors of [[adenomyosis]] are unknown and difficult to be accurately determined as [[diagnosis]] is based on examining [[pathological]] specimens only in women undergoing [[hysterectomy]]<ref name="pmid27810281">{{cite journal| author=Abbott JA| title=Adenomyosis and Abnormal Uterine Bleeding (AUB-A)-Pathogenesis, diagnosis, and management. | journal=Best Pract Res Clin Obstet Gynaecol | year= 2017 | volume= 40 | issue= | pages= 68-81 | pmid=27810281 | doi=10.1016/j.bpobgyn.2016.09.006 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27810281 }} </ref>. | |||
* [[Adenomyosis]] often coexists with other pelvic diseases namely [[endometriosis]] and [[leiomyoma]], so it is unknown whether it exhibits specific risk factors<ref name="pmid16782099">{{cite journal| author=Parker JD, Leondires M, Sinaii N, Premkumar A, Nieman LK, Stratton P| title=Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis. | journal=Fertil Steril | year= 2006 | volume= 86 | issue= 3 | pages= 711-5 | pmid=16782099 | doi=10.1016/j.fertnstert.2006.01.030 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16782099 }} </ref>. | |||
* Prior [[uterine]] surgery has been shown to be a possible risk factor for the development of [[adenomyosis]]<ref name="pmid15516398">{{cite journal| author=Panganamamula UR, Harmanli OH, Isik-Akbay EF, Grotegut CA, Dandolu V, Gaughan JP| title=Is prior uterine surgery a risk factor for adenomyosis? | journal=Obstet Gynecol | year= 2004 | volume= 104 | issue= 5 Pt 1 | pages= 1034-8 | pmid=15516398 | doi=10.1097/01.AOG.0000143264.59822.73 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15516398 }} </ref>. | |||
==[[Adenomyosis natural history, complications and prognosis|Natural History, Complications and Prognosis]]== | |||
*Early clinical features of adenomyosis include [[dysmenorrhea]], heavy [[menstrual bleeding]], and [[chronic pelvic pain]]. | |||
*Some reported [[complications]] of adenomyosis are [[preterm]] birth and [[miscarriage]] in young women diagnosed by pelvic imaging<ref name="pmid31318420">{{cite journal| author=Horton J, Sterrenburg M, Lane S, Maheshwari A, Li TC, Cheong Y| title=Reproductive, obstetric, and perinatal outcomes of women with adenomyosis and endometriosis: a systematic review and meta-analysis. | journal=Hum Reprod Update | year= 2019 | volume= 25 | issue= 5 | pages= 592-632 | pmid=31318420 | doi=10.1093/humupd/dmz012 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=31318420 }} </ref>. The relationship of adenomyosis to [[infertility]] is controversial<ref name="pmid22442261">{{cite journal| author=Maheshwari A, Gurunath S, Fatima F, Bhattacharya S| title=Adenomyosis and subfertility: a systematic review of prevalence, diagnosis, treatment and fertility outcomes. | journal=Hum Reprod Update | year= 2012 | volume= 18 | issue= 4 | pages= 374-92 | pmid=22442261 | doi=10.1093/humupd/dms006 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22442261 }} </ref>. | |||
*[[Prognosis]] is generally good as [[surgical treatment]] by [[hysterectomy]] is often curable unless there is another associated [[uterine]] pathology that requires further attention. There is no increased risk for secondary development of [[endometrial carcinoma]]. | |||
==[[Diagnosis]]== | |||
[[Adenomyosis]] is a [[histopathological]] [[diagnosis]] that is made after [[hysterectomy]]. The preoperative [[diagnosis]] is suggested by pelvic [[imaging]] such as [[transvaginal ultrasound]] and [[MRI]] along with the classical presentation of heavy [[menstrual bleeding]], [[dysmenorrhea]], and [[uniformly enlarged globular uterus]]. | |||
===[[Symptoms]]=== | |||
*[[Symptoms]] of [[adenomyosis]] may include the following<ref name="pmid4608783">{{cite journal| author=McElin TW, Bird CC| title=Adenomyosis of the uterus. | journal=Obstet Gynecol Annu | year= 1974 | volume= 3 | issue= 0 | pages= 425-41 | pmid=4608783 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=4608783 }} </ref>: | |||
:*Heavy [[menstrual bleeding]] | |||
:*[[Dysmenorrhea]] | |||
:*Chronic [[pelvic pain]] | |||
===[[Physical Examination]]=== | |||
*Bimanual [[pelvic examination]] may be remarkable for<ref name="pmid4608783">{{cite journal| author=McElin TW, Bird CC| title=Adenomyosis of the uterus. | journal=Obstet Gynecol Annu | year= 1974 | volume= 3 | issue= 0 | pages= 425-41 | pmid=4608783 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=4608783 }} </ref>: | |||
:*Diffusely enlarged [[uterus]] (Boggy soft uterus) | |||
:*[[Uterus]] is mobile (not fixed as in endometriosis) | |||
:*Uterine [[tenderness]] may be noted. | |||
== | === [[Pelvic Imaging]] === | ||
The [[uterus]] may be imaged using [[ultrasound]] (US) or [[magnetic resonance imaging]] (MRI). Transvaginal ultrasound is the most cost-effective and most available. Either modality will show an enlarged uterus. On ultrasound, the uterus will have a heterogeneous texture, without the focal well-defined masses that characterize [[leiomyoma|uterine fibroids]]. | |||
====[[Ultrasonography]]==== | |||
*Typical appearances of [[adenomyosis]] at [[transvaginal ultrasound]] include poorly marginated [[hypoechoic]] and [[heterogeneous]] areas within the [[myometrium]], [[myometrial]] cysts, and a globular or enlarged [[uterus]] with asymmetry. | |||
[http://www.radswiki.net Image courtesy of RadsWiki] | |||
<gallery perRow="3"> | <gallery perRow="3"> | ||
Image:Adenomyosis ultrasound 101.jpg|US: Adenomyosis | |||
Image:Adenomyosis ultrasound 102.jpg|US: Adenomyosis | |||
Image:Adenomyosis ultrasound 103.jpg|US: Adenomyosis | |||
</gallery> | |||
====[[Computed Tomography]]==== | |||
[http://www.radswiki.net Images courtesy of RadsWiki] | |||
<gallery perRow="3"> | |||
Image:Adenomyosis CT 108.jpg|CT: Adenomyosis | |||
Image:Adenomyosis CT 109.jpg|CT: Adenomyosis | |||
</gallery> | |||
====[[Magnetic Resonance Imaging]]==== | |||
* [[MRI]] provides better diagnostic capability due to the increased spatial and contrast [[resolution]], and to not be limited by the presence of bowel gas or calcified [[uterine]] fibroids (as is [[ultrasound]]). In particular, [[MRI]] is better able to differentiate [[adenomyosis]] from multiple small [[leiomyoma|uterine fibroids]]. | |||
* [[MRI]] can be used to classify [[adenomyosis]] based on the depth of penetration of the ectopic [[endometrium]] into the [[myometrium]]. | |||
*[[Adenomyosis]] appears as either diffuse or focal thickening (greater than 12 mm )of the [[junctional zone]] forming an ill-defined area of low signal intensity, occasionally with embedded bright foci on [[T2-weighted]] images. | |||
*[[Histologically]], areas of low signal intensity correspond to [[smooth muscle]] [[hyperplasia]], and bright foci on [[T2-weighted]] images correspond to islands of ectopic [[endometrial]] tissue and cystic dilatation of [[glands]]. | |||
[http://www.radswiki.net Images courtesy of RadsWiki] | |||
<gallery perRow="2"> | |||
Image:Adenomyosis MRI 104.jpg|T2: Adenomyosis | |||
Image:Adenomyosis MRI 105.jpg|T2: Adenomyosis | |||
Image:Adenomyosis MRI 106.jpg|T2: Adenomyosis | |||
Image:Adenomyosis MRI 107.jpg|T1 fat sat contrast: Adenomyosis | |||
</gallery> | </gallery> | ||
| Line 71: | Line 146: | ||
<br clear="left"/> | <br clear="left"/> | ||
==Treatment== | == [[Treatment]] == | ||
=== [[Surgery]] === | |||
*[[Surgery]] is the mainstay of therapy for [[adenomyosis]]<ref name="pmid30918629">{{cite journal| author=Vannuccini S, Petraglia F| title=Recent advances in understanding and managing adenomyosis. | journal=F1000Res | year= 2019 | volume= 8 | issue= | pages= | pmid=30918629 | doi=10.12688/f1000research.17242.1 | pmc=6419978 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=30918629 }} </ref>. | |||
*[[Hysterectomy]] with preservation of the [[ovaries]] is the most common approach to the [[treatment]] of [[adenomyosis]], and it is done via [[abdominal]], [[transvaginal]], [[laparoscopic]] approach, or [[robotic surgery]]. <ref name="pmid30918629">{{cite journal| author=Vannuccini S, Petraglia F| title=Recent advances in understanding and managing adenomyosis. | journal=F1000Res | year= 2019 | volume= 8 | issue= | pages= | pmid=30918629 | doi=10.12688/f1000research.17242.1 | pmc=6419978 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=30918629 }} </ref>. | |||
*Unlike [[Leiomyoma]], there is no plane of cleavage to excise [[adenomyomas]] and preserve the [[uterus]]. [[Uterus]] sparing resection is an investigational approach especially for young women seeking future [[pregnancy]]<ref name="pmid9825848">{{cite journal| author=Wood C| title=Surgical and medical treatment of adenomyosis. | journal=Hum Reprod Update | year= 1998 | volume= 4 | issue= 4 | pages= 323-36 | pmid=9825848 | doi=10.1093/humupd/4.4.323 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=9825848 }} </ref>. | |||
== | |||
=== [[Medical Therapy]] === | |||
*[[ | *[[Medical]] [[treatment]] for [[dysmenorrhea]] and [[menorrhagia]] can be prescribed as a temporary alternative for young women in the child-bearing period. | ||
*[[ | *[[Hormonal]] therapy to control the symptoms includes [[levonorgestrel]]-releasing [[IUD]] (most preferred method), [[combined oral contraceptive pills]], [[GnRH]] analogs, and oral [[GnRH]] antagonists<ref name="pmid31971678">{{cite journal| author=Schlaff WD, Ackerman RT, Al-Hendy A, Archer DF, Barnhart KT, Bradley LD | display-authors=etal| title=Elagolix for Heavy Menstrual Bleeding in Women with Uterine Fibroids. | journal=N Engl J Med | year= 2020 | volume= 382 | issue= 4 | pages= 328-340 | pmid=31971678 | doi=10.1056/NEJMoa1904351 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=31971678 }} </ref>. | ||
*[[Levonorgestrel]]-[[IUD]] has a direct action on the [[uterus]]. It alleviates [[dysmenorrhea]] and [[menorrhagia]]<ref name="pmid17707716">{{cite journal| author=Bragheto AM, Caserta N, Bahamondes L, Petta CA| title=Effectiveness of the levonorgestrel-releasing intrauterine system in the treatment of adenomyosis diagnosed and monitored by magnetic resonance imaging. | journal=Contraception | year= 2007 | volume= 76 | issue= 3 | pages= 195-9 | pmid=17707716 | doi=10.1016/j.contraception.2007.05.091 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=17707716 }} </ref>. | |||
*Once the [[hormonal]] [[therapy]] is stopped to conceive, [[symptoms]] recur within six months. | |||
=== [[Uterine artery embolization]] === | |||
*In women who decline [[hysterectomy]] or have [[contraindications]] for [[hysterectomy]] or women who failed [[hormonal]] [[therapy]], [[uterine artery embolization]] can be an alternative to control [[dysmenorrhea]] and heavy [[menstrual bleeding]].<ref name="pmid27806072">{{cite journal| author=Zhou J, He L, Liu P, Duan H, Zhang H, Li W | display-authors=etal| title=Outcomes in Adenomyosis Treated with Uterine Artery Embolization Are Associated with Lesion Vascularity: A Long-Term Follow-Up Study of 252 Cases. | journal=PLoS One | year= 2016 | volume= 11 | issue= 11 | pages= e0165610 | pmid=27806072 | doi=10.1371/journal.pone.0165610 | pmc=5091759 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27806072 }} </ref>. | |||
* The outcomes of the [[procedure]] are significantly correlated with the lesion [[vascularity]].<ref name="pmid27806072">{{cite journal| author=Zhou J, He L, Liu P, Duan H, Zhang H, Li W | display-authors=etal| title=Outcomes in Adenomyosis Treated with Uterine Artery Embolization Are Associated with Lesion Vascularity: A Long-Term Follow-Up Study of 252 Cases. | journal=PLoS One | year= 2016 | volume= 11 | issue= 11 | pages= e0165610 | pmid=27806072 | doi=10.1371/journal.pone.0165610 | pmc=5091759 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27806072 }} </ref>. | |||
== | ==[[References]]== | ||
{{Reflist|2}} | |||
== | ==[[Additional Resources]]== | ||
{{refbegin|2}} | |||
* Atri M, Reinhold C, Mehio AR. Adenomyosis: US features with histologic correlation in an in-vitro study. Radiology. Jun 2000;215(3):783-90. | |||
* Batzer FR, Hansen L. Bizarre sonographic appearance of an adenomyoma and its presentation. J Ultrasound Med. Aug 1996;15(8):599-602. | |||
* Bazot M, Daraï E. [Evaluation of pelvic endometriosis: the role of MRI.]. J Radiol. Nov 2008;89(11 Pt 1):1695-6. | |||
* Byun JY, Kim SE, Choi BG, et al. Diffuse and focal adenomyosis: MR imaging findings. Radiographics. Oct 1999;19 Spec No:S161-70. | |||
* Chiang CH, Chang MY, Hsu JJ. Tumor vascular pattern and blood flow impedance in the differential diagnosis of leiomyoma and adenomyosis by color Doppler sonography. J Assist Reprod Genet. May 1999;16(5):268-75. | |||
* Guilbeault H, Wilson SR, Lickrish GM. Massive uterine enlargement with necrosis: an unusual manifestation of adenomyosis. J Ultrasound Med. Apr 1994;13(4):326-8. | |||
* Haimovici JB, Tempany CM. MR of the female pelvis: benign disease. Appl Radiol. Jun 1994;7:21. | |||
* Huang HY. Medical treatment of endometriosis. Chang Gung Med J. Sep-Oct 2008;31(5):431-40. | |||
* Iribarne C, Plaza J, De la Fuente P, et al. Intramyometrial cystic adenomyosis. J Clin Ultrasound. Jun 1994;22(5):348-50. | |||
* Jarlot C, Anglade E, Paillocher N, Moreau D, Catala L, Aubé C. [MR imaging features of deep pelvic endometriosis: correlation with laparoscopy.]. J Radiol. Nov 2008;89(11 Pt 1):1745-54. | |||
* Kang S, Turner DA, Foster GS, et al. Adenomyosis: specificity of 5 mm as the maximum normal uterine junctional zone thickness in MR images. AJR Am J Roentgenol. May 1996;166(5):1145-50. | |||
* Kim MD, Lee HS, Lee MH, Kim HJ, Cho JH, Cha SH. Long-term results of symptomatic fibroids treated with uterine artery embolization: In conjunction with MR evaluation. Eur J Radiol. Dec 10 2008; | |||
* Ostrzenski A. Extensive iatrogenic adenomyosis after laparoscopic myomectomy. Fertil Steril. Jan 1998;69(1):143-5. | |||
* Piketty M, Chopin N, Dousset B, Millischer-Bellaische AE, Roseau G, Leconte M, et al. Preoperative work-up for patients with deeply infiltrating endometriosis: transvaginal ultrasonography must definitely be the first-line imaging examination. Hum Reprod. Dec 17 2008; | |||
* Piketty M, Chopin N, Dousset B, Millischer-Bellaische AE, Roseau G, Leconte M, et al. Preoperative work-up for patients with deeply infiltrating endometriosis: transvaginal ultrasonography must definitely be the first-line imaging examination. Hum Reprod. Dec 17 2008; | |||
* Reinhold C, Atri M, Mehio A, et al. Diffuse uterine adenomyosis: morphologic criteria and diagnostic accuracy of endovaginal sonography. Radiology. Dec 1995;197(3):609-14. | |||
* Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics. Oct 1999;19 Spec No:S147-60. | |||
* Tamai K, Koyama T, Umeoka S, et al. Spectrum of MR features in adenomyosis. Best Pract Res Clin Obstet Gynaecol. Aug 2006;20(4):583-602. | |||
* Tamai K, Togashi K, Ito T, et al. MR imaging findings of adenomyosis: correlation with histopathologic features and diagnostic pitfalls. Radiographics. Jan-Feb 2005;25(1):21-40. | |||
* Utsunomiya D, Notsute S, Hayashida Y, et al. Endometrial carcinoma in adenomyosis: assessment of myometrial invasion on T2-weighted spin-echo and gadolinium-enhanced T1-weighted images. AJR Am J Roentgenol. Feb 2004;182(2):399-404. | |||
{{refend}} | |||
{{Diseases of the pelvis, genitals and breasts}} | {{Diseases of the pelvis, genitals and breasts}} | ||
[[nl:Adenomyose]] | [[nl:Adenomyose]] | ||
| Line 104: | Line 197: | ||
{{WikiDoc Help Menu}} | {{WikiDoc Help Menu}} | ||
{{WikiDoc Sources}} | {{WikiDoc Sources}} | ||
[[Category:Overview complete]] | |||
[[Category:Disease]] | |||
[[Category:Gynecology]] | |||
Latest revision as of 20:25, 25 May 2021
For patient information, click here
Template:DiseaseDisorder infobox
|
WikiDoc Resources for Adenomyosis |
|
Articles |
|---|
|
Most recent articles on Adenomyosis Most cited articles on Adenomyosis |
|
Media |
|
Powerpoint slides on Adenomyosis |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Adenomyosis at Clinical Trials.gov Clinical Trials on Adenomyosis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Adenomyosis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Adenomyosis Discussion groups on Adenomyosis Patient Handouts on Adenomyosis Directions to Hospitals Treating Adenomyosis Risk calculators and risk factors for Adenomyosis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Adenomyosis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun M.D. PhD.[2], Dina Elantably, MD[3]
Overview
Adenomyosis is a medical condition characterized by the presence of ectopic endometrial tissue (the inner lining of the uterus) within the myometrium (the thick, muscular layer of the uterus). The condition is typically found in women between the ages between 35 and 50. Patients with adenomyosis can have painful and/or profuse menses (dysmenorrhea & menorrhagia, respectively). Adenomyosis may involve the uterus focally, creating an adenomyoma, or diffusely. With diffuse involvement, the uterus becomes bulky and heavier.
Historical Perspective
- Adenomyosis was first discovered by Carl von Rokitansky, a German pathologist, in 1860 when he found endometrial glands in the myometrium and designated this finding as 'cystosarcoma adenoids uterinum'[1].
- In 1892 the first systematic investigation of adenomyosis was carried out by 'Thomas Stephen Cullen', a gynecologist. He distinguished 3 types of adenomyoma: intramural, subperitoneal and submucous adenomyoma[1].
- In 1893, Kelly and Cullen described the pathogenesis of adenomyoma. The 'gradual ascendancy of Cullen’s mucosal theory' stated that endometrium invades the inner myometrium through the presence in it of ‘chinks’, or fissures.
- In 1892, Cullen described that abdominal hysterectomy is indicated for treatment as the endometrial growths are interwoven with the normal muscle of the uterus.
Classification
- Adenomyosis can be classified according to its histopathology into 2 groups:
- Diffuse adenomyosis: Uniformly enlarged boggy uterus.
- Focal adenomyosis (adenomyoma): Grossly it resembles fibroid but without a surrounding pseudocapsule.
- Other variants of adenomyosis include juvenile cystic adenomyosis; which is the presence of endometrial cysts > 1cm in diameter within the myometrium. It is usually seen in young women <30 years old [2].
Pathophysiology
- The pathogenesis of Adenomyosis is poorly understood. There two theories that explain the possible pathogenesis[3]:
- Endomyometrial invagination of the endometrium; due to weakness of the uterine smooth muscles.
- De novo development of adenomyosis from mullerian rests due to metaplasia.
- The basic Fibroblast Growth Factor (bFGF) receptor/ligand system has shown to be upregulated in adenomyosis which explain the abnormal uterine bleeding and menorrhagia[4].
- Estrogen and progesterone hormones play a role in the pathogenesis of adenomyosis[5]. Other hormones such as oxytocin [6], FSH[7], and prolactin[8] also contribute to the pathogenesis of the disease.
- On gross pathology, there is a globular enlargement of the myometrium of the uterus showing cysts filled with hemolysed red blood cells and sideroblasts[9].
- On microscopic histopathological analysis, there are endometrial glands, and stroma surrounded by hypertrophic smooth muscle bundles haphazardly scattered within the myometrium[9].
{{#ev:youtube|nOCtpIwCZ-Y}}
Causes
The cause of adenomyosis is unknown, although it has been associated with any sort of uterine trauma that may break the barrier between the endometrium and myometrium, such as:
Differentiating adenomyosis from other Diseases
For further information about the differential diagnosis, click here.
Epidemiology and Demographics
- It is generally estimated that adenomyosis is present in 20-35% of women[10].
- The incidence and prevalence of adenomyosis are, however, difficult to be accurately estimated and biased by studying only women undergoing hysterectomy, so the total population of women having the disease is not known[11].
Age
- Adenomyosis is more commonly observed among women aged 40-50 years in those undergoing hysterectomy for diagnosis[9].
- Adenomyosis is less commonly diagnosed in adolescents who undergo pelvic imaging by transvaginal ultrasound or MRI rather than a hysterectomy for diagnosis[12].
Race
- There is no racial predilection for adenomyosis.
- Almost all cases of adenomyosis present in multiparous women, however there is no clear causal relationship between multiparty and the development of the disease[9]
Risk Factors
- Similar to the epidemiology, the risk factors of adenomyosis are unknown and difficult to be accurately determined as diagnosis is based on examining pathological specimens only in women undergoing hysterectomy[11].
- Adenomyosis often coexists with other pelvic diseases namely endometriosis and leiomyoma, so it is unknown whether it exhibits specific risk factors[12].
- Prior uterine surgery has been shown to be a possible risk factor for the development of adenomyosis[13].
Natural History, Complications and Prognosis
- Early clinical features of adenomyosis include dysmenorrhea, heavy menstrual bleeding, and chronic pelvic pain.
- Some reported complications of adenomyosis are preterm birth and miscarriage in young women diagnosed by pelvic imaging[14]. The relationship of adenomyosis to infertility is controversial[15].
- Prognosis is generally good as surgical treatment by hysterectomy is often curable unless there is another associated uterine pathology that requires further attention. There is no increased risk for secondary development of endometrial carcinoma.
Diagnosis
Adenomyosis is a histopathological diagnosis that is made after hysterectomy. The preoperative diagnosis is suggested by pelvic imaging such as transvaginal ultrasound and MRI along with the classical presentation of heavy menstrual bleeding, dysmenorrhea, and uniformly enlarged globular uterus.
Symptoms
- Symptoms of adenomyosis may include the following[16]:
- Heavy menstrual bleeding
- Dysmenorrhea
- Chronic pelvic pain
Physical Examination
- Bimanual pelvic examination may be remarkable for[16]:
- Diffusely enlarged uterus (Boggy soft uterus)
- Uterus is mobile (not fixed as in endometriosis)
- Uterine tenderness may be noted.
Pelvic Imaging
The uterus may be imaged using ultrasound (US) or magnetic resonance imaging (MRI). Transvaginal ultrasound is the most cost-effective and most available. Either modality will show an enlarged uterus. On ultrasound, the uterus will have a heterogeneous texture, without the focal well-defined masses that characterize uterine fibroids.
Ultrasonography
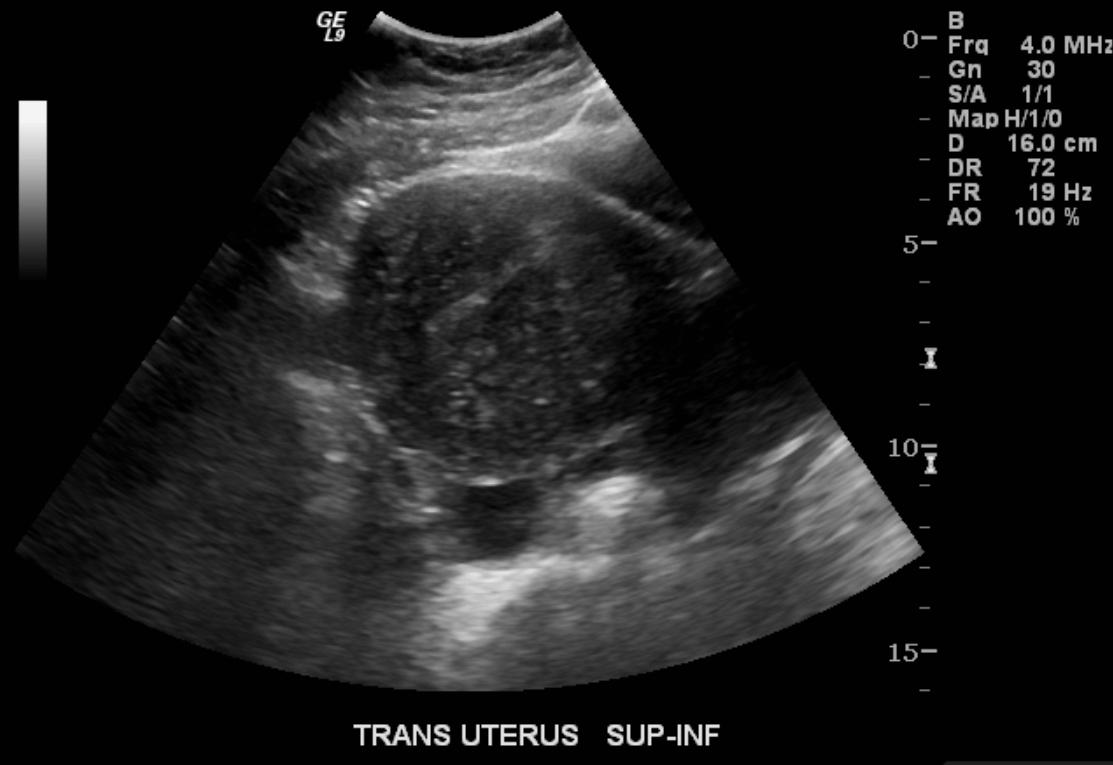
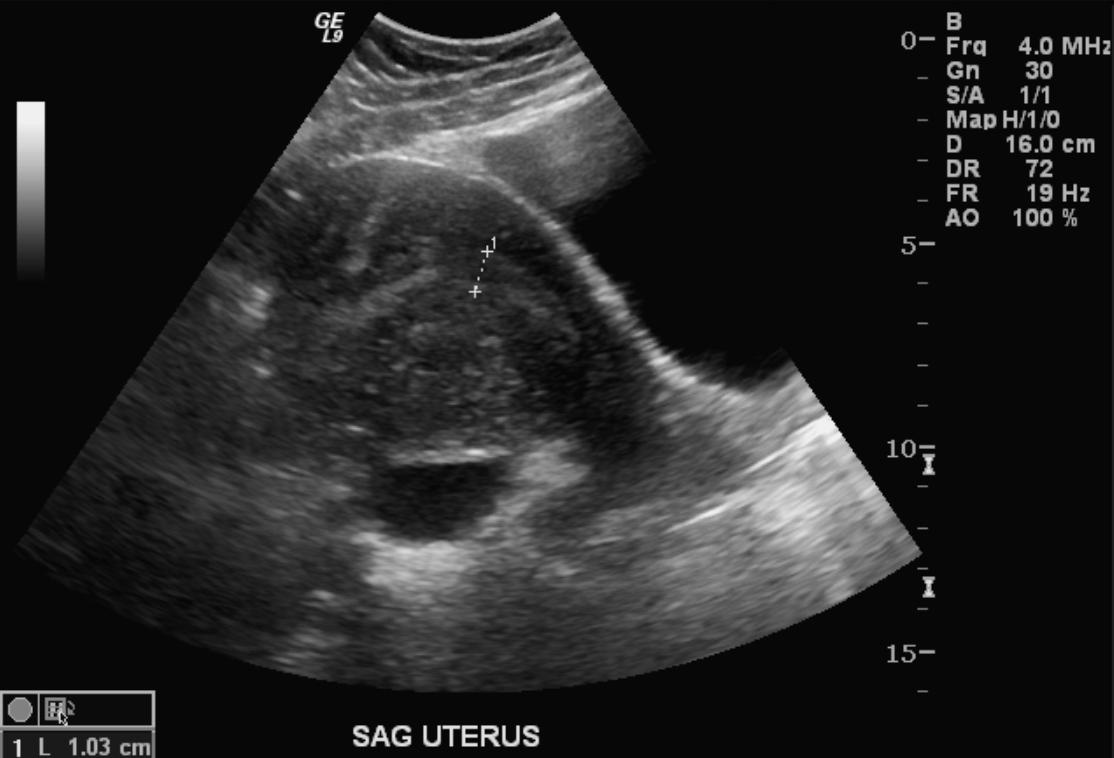
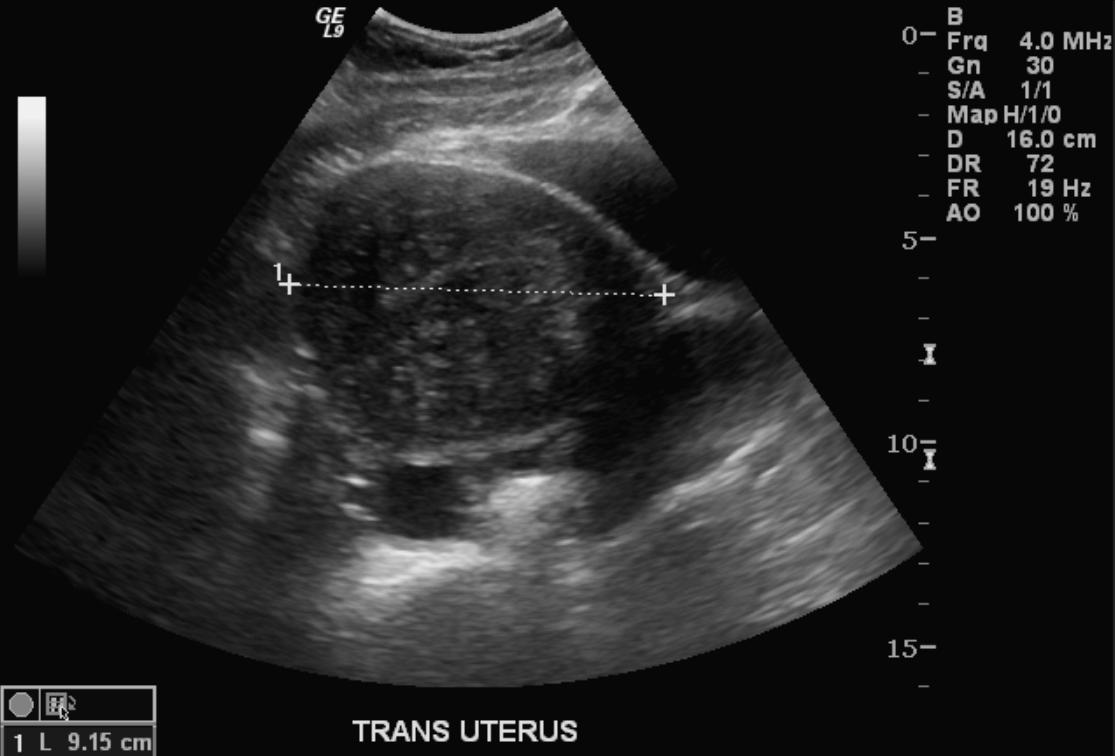
- Typical appearances of adenomyosis at transvaginal ultrasound include poorly marginated hypoechoic and heterogeneous areas within the myometrium, myometrial cysts, and a globular or enlarged uterus with asymmetry.
-
US: Adenomyosis
-
US: Adenomyosis
-
US: Adenomyosis



Computed Tomography
-

CT: Adenomyosis
-

CT: Adenomyosis


Magnetic Resonance Imaging
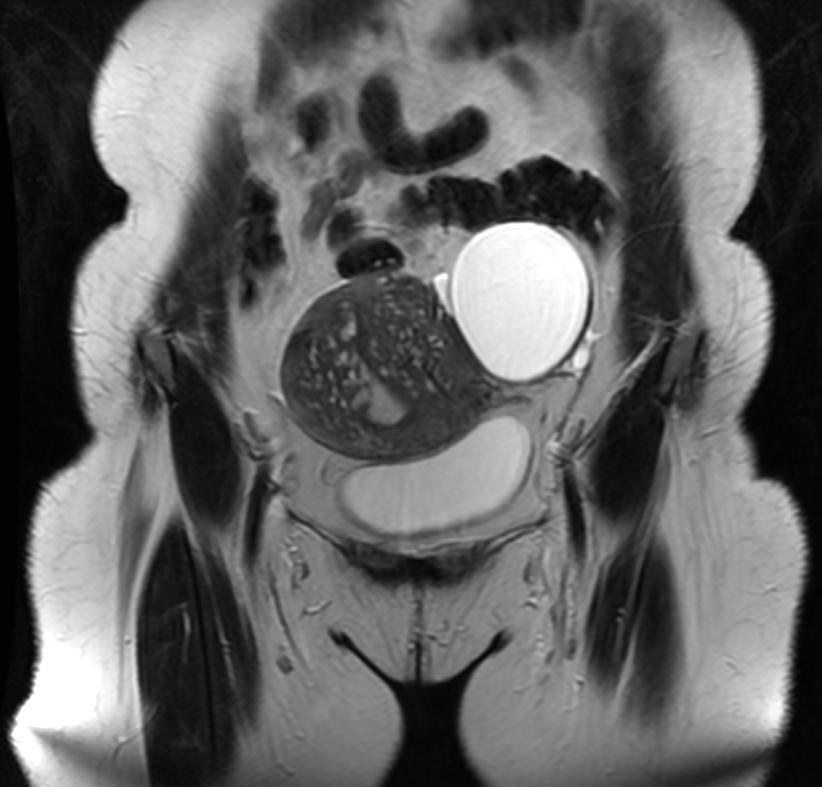
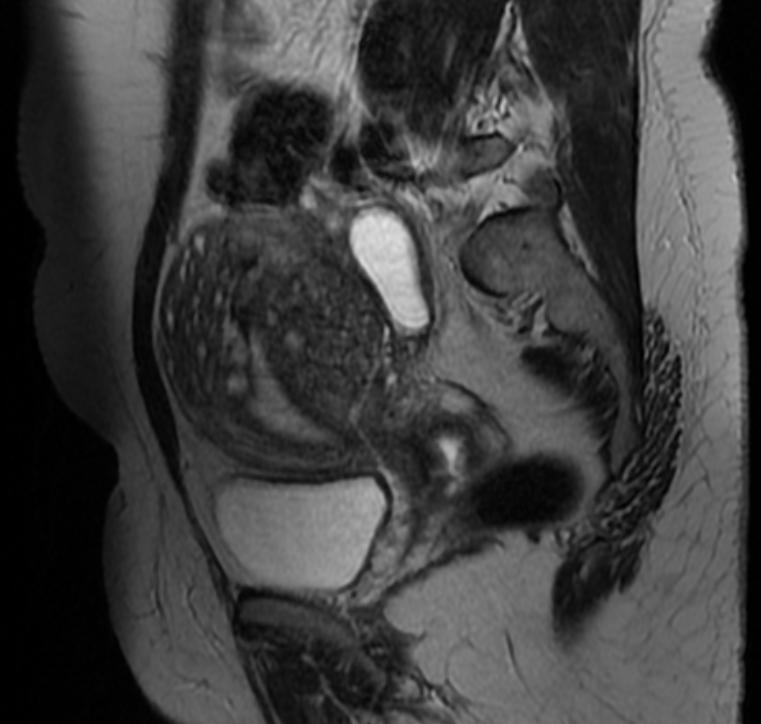
- MRI provides better diagnostic capability due to the increased spatial and contrast resolution, and to not be limited by the presence of bowel gas or calcified uterine fibroids (as is ultrasound). In particular, MRI is better able to differentiate adenomyosis from multiple small uterine fibroids.
- MRI can be used to classify adenomyosis based on the depth of penetration of the ectopic endometrium into the myometrium.
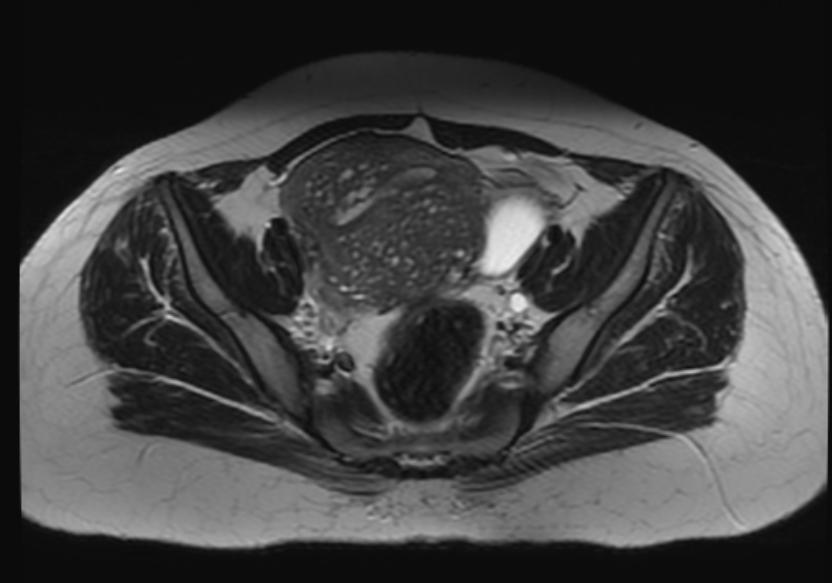
- Adenomyosis appears as either diffuse or focal thickening (greater than 12 mm )of the junctional zone forming an ill-defined area of low signal intensity, occasionally with embedded bright foci on T2-weighted images.
- Histologically, areas of low signal intensity correspond to smooth muscle hyperplasia, and bright foci on T2-weighted images correspond to islands of ectopic endometrial tissue and cystic dilatation of glands.
-
T2: Adenomyosis
-
T2: Adenomyosis
-
T2: Adenomyosis
-
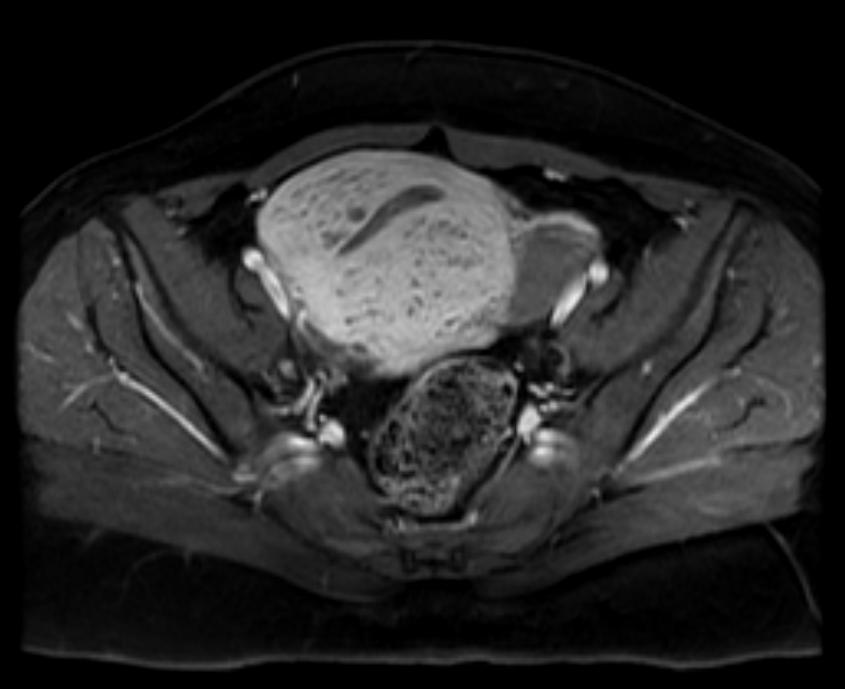
T1 fat sat contrast: Adenomyosis






Treatment
Surgery
- Surgery is the mainstay of therapy for adenomyosis[17].
- Hysterectomy with preservation of the ovaries is the most common approach to the treatment of adenomyosis, and it is done via abdominal, transvaginal, laparoscopic approach, or robotic surgery. [17].
- Unlike Leiomyoma, there is no plane of cleavage to excise adenomyomas and preserve the uterus. Uterus sparing resection is an investigational approach especially for young women seeking future pregnancy[18].
Medical Therapy
- Medical treatment for dysmenorrhea and menorrhagia can be prescribed as a temporary alternative for young women in the child-bearing period.
- Hormonal therapy to control the symptoms includes levonorgestrel-releasing IUD (most preferred method), combined oral contraceptive pills, GnRH analogs, and oral GnRH antagonists[19].
- Levonorgestrel-IUD has a direct action on the uterus. It alleviates dysmenorrhea and menorrhagia[20].
- Once the hormonal therapy is stopped to conceive, symptoms recur within six months.
Uterine artery embolization
- In women who decline hysterectomy or have contraindications for hysterectomy or women who failed hormonal therapy, uterine artery embolization can be an alternative to control dysmenorrhea and heavy menstrual bleeding.[21].
- The outcomes of the procedure are significantly correlated with the lesion vascularity.[21].
References
- ↑ 1.0 1.1 Benagiano G, Brosens I (2006). "History of adenomyosis". Best Pract Res Clin Obstet Gynaecol. 20 (4): 449–63. doi:10.1016/j.bpobgyn.2006.01.007. PMID 16515887.
- ↑ Takeuchi H, Kitade M, Kikuchi I, Kumakiri J, Kuroda K, Jinushi M (2010). "Diagnosis, laparoscopic management, and histopathologic findings of juvenile cystic adenomyoma: a review of nine cases". Fertil Steril. 94 (3): 862–8. doi:10.1016/j.fertnstert.2009.05.010. PMID 19539912.
- ↑ Ferenczy A (1998). "Pathophysiology of adenomyosis". Hum Reprod Update. 4 (4): 312–22. doi:10.1093/humupd/4.4.312. PMID 9825847.
- ↑ Propst AM, Quade BJ, Gargiulo AR, Nowak RA, Stewart EA (2001). "Adenomyosis demonstrates increased expression of the basic fibroblast growth factor receptor/ligand system compared with autologous endometrium". Menopause. 8 (5): 368–71. doi:10.1097/00042192-200109000-00012. PMID 11528364.
- ↑ Green AR, Styles JA, Parrott EL, Gray D, Edwards RE, Smith AG; et al. (2005). "Neonatal tamoxifen treatment of mice leads to adenomyosis but not uterine cancer". Exp Toxicol Pathol. 56 (4–5): 255–63. doi:10.1016/j.etp.2004.10.001. PMID 15816354.
- ↑ Guo SW, Mao X, Ma Q, Liu X (2013). "Dysmenorrhea and its severity are associated with increased uterine contractility and overexpression of oxytocin receptor (OTR) in women with symptomatic adenomyosis". Fertil Steril. 99 (1): 231–240. doi:10.1016/j.fertnstert.2012.08.038. PMID 22999795.
- ↑ Stewart EA (2001). "Gonadotropins and the uterus: is there a gonad-independent pathway?". J Soc Gynecol Investig. 8 (6): 319–26. PMID 11750866.
- ↑ Mori T, Singtripop T, Kawashima S (1991). "Animal model of uterine adenomyosis: is prolactin a potent inducer of adenomyosis in mice?". Am J Obstet Gynecol. 165 (1): 232–4. doi:10.1016/0002-9378(91)90258-s. PMID 1853904.
- ↑ 9.0 9.1 9.2 9.3 Bergeron C, Amant F, Ferenczy A (2006). "Pathology and physiopathology of adenomyosis". Best Pract Res Clin Obstet Gynaecol. 20 (4): 511–21. doi:10.1016/j.bpobgyn.2006.01.016. PMID 16563870.
- ↑ Vercellini P, Viganò P, Somigliana E, Daguati R, Abbiati A, Fedele L (2006). "Adenomyosis: epidemiological factors". Best Pract Res Clin Obstet Gynaecol. 20 (4): 465–77. doi:10.1016/j.bpobgyn.2006.01.017. PMID 16563868.
- ↑ 11.0 11.1 Abbott JA (2017). "Adenomyosis and Abnormal Uterine Bleeding (AUB-A)-Pathogenesis, diagnosis, and management". Best Pract Res Clin Obstet Gynaecol. 40: 68–81. doi:10.1016/j.bpobgyn.2016.09.006. PMID 27810281.
- ↑ 12.0 12.1 Parker JD, Leondires M, Sinaii N, Premkumar A, Nieman LK, Stratton P (2006). "Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis". Fertil Steril. 86 (3): 711–5. doi:10.1016/j.fertnstert.2006.01.030. PMID 16782099.
- ↑ Panganamamula UR, Harmanli OH, Isik-Akbay EF, Grotegut CA, Dandolu V, Gaughan JP (2004). "Is prior uterine surgery a risk factor for adenomyosis?". Obstet Gynecol. 104 (5 Pt 1): 1034–8. doi:10.1097/01.AOG.0000143264.59822.73. PMID 15516398.
- ↑ Horton J, Sterrenburg M, Lane S, Maheshwari A, Li TC, Cheong Y (2019). "Reproductive, obstetric, and perinatal outcomes of women with adenomyosis and endometriosis: a systematic review and meta-analysis". Hum Reprod Update. 25 (5): 592–632. doi:10.1093/humupd/dmz012. PMID 31318420.
- ↑ Maheshwari A, Gurunath S, Fatima F, Bhattacharya S (2012). "Adenomyosis and subfertility: a systematic review of prevalence, diagnosis, treatment and fertility outcomes". Hum Reprod Update. 18 (4): 374–92. doi:10.1093/humupd/dms006. PMID 22442261.
- ↑ 16.0 16.1 McElin TW, Bird CC (1974). "Adenomyosis of the uterus". Obstet Gynecol Annu. 3 (0): 425–41. PMID 4608783.
- ↑ 17.0 17.1 Vannuccini S, Petraglia F (2019). "Recent advances in understanding and managing adenomyosis". F1000Res. 8. doi:10.12688/f1000research.17242.1. PMC 6419978. PMID 30918629.
- ↑ Wood C (1998). "Surgical and medical treatment of adenomyosis". Hum Reprod Update. 4 (4): 323–36. doi:10.1093/humupd/4.4.323. PMID 9825848.
- ↑ Schlaff WD, Ackerman RT, Al-Hendy A, Archer DF, Barnhart KT, Bradley LD; et al. (2020). "Elagolix for Heavy Menstrual Bleeding in Women with Uterine Fibroids". N Engl J Med. 382 (4): 328–340. doi:10.1056/NEJMoa1904351. PMID 31971678.
- ↑ Bragheto AM, Caserta N, Bahamondes L, Petta CA (2007). "Effectiveness of the levonorgestrel-releasing intrauterine system in the treatment of adenomyosis diagnosed and monitored by magnetic resonance imaging". Contraception. 76 (3): 195–9. doi:10.1016/j.contraception.2007.05.091. PMID 17707716.
- ↑ 21.0 21.1 Zhou J, He L, Liu P, Duan H, Zhang H, Li W; et al. (2016). "Outcomes in Adenomyosis Treated with Uterine Artery Embolization Are Associated with Lesion Vascularity: A Long-Term Follow-Up Study of 252 Cases". PLoS One. 11 (11): e0165610. doi:10.1371/journal.pone.0165610. PMC 5091759. PMID 27806072.
Additional Resources
- Atri M, Reinhold C, Mehio AR. Adenomyosis: US features with histologic correlation in an in-vitro study. Radiology. Jun 2000;215(3):783-90.
- Batzer FR, Hansen L. Bizarre sonographic appearance of an adenomyoma and its presentation. J Ultrasound Med. Aug 1996;15(8):599-602.
- Bazot M, Daraï E. [Evaluation of pelvic endometriosis: the role of MRI.]. J Radiol. Nov 2008;89(11 Pt 1):1695-6.
- Byun JY, Kim SE, Choi BG, et al. Diffuse and focal adenomyosis: MR imaging findings. Radiographics. Oct 1999;19 Spec No:S161-70.
- Chiang CH, Chang MY, Hsu JJ. Tumor vascular pattern and blood flow impedance in the differential diagnosis of leiomyoma and adenomyosis by color Doppler sonography. J Assist Reprod Genet. May 1999;16(5):268-75.
- Guilbeault H, Wilson SR, Lickrish GM. Massive uterine enlargement with necrosis: an unusual manifestation of adenomyosis. J Ultrasound Med. Apr 1994;13(4):326-8.
- Haimovici JB, Tempany CM. MR of the female pelvis: benign disease. Appl Radiol. Jun 1994;7:21.
- Huang HY. Medical treatment of endometriosis. Chang Gung Med J. Sep-Oct 2008;31(5):431-40.
- Iribarne C, Plaza J, De la Fuente P, et al. Intramyometrial cystic adenomyosis. J Clin Ultrasound. Jun 1994;22(5):348-50.
- Jarlot C, Anglade E, Paillocher N, Moreau D, Catala L, Aubé C. [MR imaging features of deep pelvic endometriosis: correlation with laparoscopy.]. J Radiol. Nov 2008;89(11 Pt 1):1745-54.
- Kang S, Turner DA, Foster GS, et al. Adenomyosis: specificity of 5 mm as the maximum normal uterine junctional zone thickness in MR images. AJR Am J Roentgenol. May 1996;166(5):1145-50.
- Kim MD, Lee HS, Lee MH, Kim HJ, Cho JH, Cha SH. Long-term results of symptomatic fibroids treated with uterine artery embolization: In conjunction with MR evaluation. Eur J Radiol. Dec 10 2008;
- Ostrzenski A. Extensive iatrogenic adenomyosis after laparoscopic myomectomy. Fertil Steril. Jan 1998;69(1):143-5.
- Piketty M, Chopin N, Dousset B, Millischer-Bellaische AE, Roseau G, Leconte M, et al. Preoperative work-up for patients with deeply infiltrating endometriosis: transvaginal ultrasonography must definitely be the first-line imaging examination. Hum Reprod. Dec 17 2008;
- Piketty M, Chopin N, Dousset B, Millischer-Bellaische AE, Roseau G, Leconte M, et al. Preoperative work-up for patients with deeply infiltrating endometriosis: transvaginal ultrasonography must definitely be the first-line imaging examination. Hum Reprod. Dec 17 2008;
- Reinhold C, Atri M, Mehio A, et al. Diffuse uterine adenomyosis: morphologic criteria and diagnostic accuracy of endovaginal sonography. Radiology. Dec 1995;197(3):609-14.
- Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics. Oct 1999;19 Spec No:S147-60.
- Tamai K, Koyama T, Umeoka S, et al. Spectrum of MR features in adenomyosis. Best Pract Res Clin Obstet Gynaecol. Aug 2006;20(4):583-602.
- Tamai K, Togashi K, Ito T, et al. MR imaging findings of adenomyosis: correlation with histopathologic features and diagnostic pitfalls. Radiographics. Jan-Feb 2005;25(1):21-40.
- Utsunomiya D, Notsute S, Hayashida Y, et al. Endometrial carcinoma in adenomyosis: assessment of myometrial invasion on T2-weighted spin-echo and gadolinium-enhanced T1-weighted images. AJR Am J Roentgenol. Feb 2004;182(2):399-404.
Template:Diseases of the pelvis, genitals and breasts