Thymus
|
WikiDoc Resources for Thymus |
|
Articles |
|---|
|
Media |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Thymus at Clinical Trials.gov Clinical Trials on Thymus at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Thymus
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Directions to Hospitals Treating Thymus Risk calculators and risk factors for Thymus
|
|
Healthcare Provider Resources |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
In human anatomy, the thymus is an organ located in the upper anterior portion of the chest cavity just behind the sternum. Hormones produced by this organ stimulate the production of certain infection-fighting cells. It is of central importance in the maturation of T cells.
History
Due to the large numbers of apoptotic lymphocytes, the thymus was originally dismissed as a "lymphocyte graveyard", without functional importance. The importance of the thymus in the immune system was discovered in 1961 by Jacques Miller, by surgically removing the thymus from three day old mice, and observing the subsequent deficiency in a lymphocyte population, subsequently named T cells after the organ of their origin. [1] Recently advances in immunology have allowed the fine dissection of the function of the thymus in T cell maturation.
Development
Embryology
The two main components of the thymus, the lymphoid thymocytes and the thymic epithelial cells, have distinct developmental origins. The thymic epithelium is the first to develop, and appears in the form of two flask-shape endodermal diverticula, which arise, one on either side, from the third branchial pouch (pharyngeal pouch), and extend lateralward and backward into the surrounding mesoderm and neural crest-derived mesenchyme in front of the ventral aorta.
Here they meet and become joined to one another by connective tissue, but there is never any fusion of the thymus tissue proper. The pharyngeal opening of each diverticulum is soon obliterated, but the neck of the flask persists for some time as a cellular cord. By further proliferation of the cells lining the flask, buds of cells are formed, which become surrounded and isolated by the invading mesoderm. Additional portions of thymus tissue are sometimes developed from the fourth branchial pouches. [2]
During the late stages of the development of the thymic epithelium, hematopoietic lymphoid cells from bone-marrow precursors immigrate into the thymus and are aggregated to form lymphoid follicles.
The thymus continues to grow between birth and puberty and then begins to atrophy, a process directed by the high levels of circulating sex hormones. Proportional to thymic size, thymic activity (T cell output) is most active before puberty. Upon atrophy, the size and activity are dramatically reduced, and the organ is primarily replaced with fat (a phenomenon known as "involution"). The atrophy is due to the increased circulating level of sex hormones, and chemical or physical castration of an adult results in the thymus increasing in size and activity. [3] Patients with the autoimmune disease Myasthenia gravis commonly (70%) are found to have thymic hyperplasia or malignancy.[4] The reason or order of these cirumstances has yet to be determined by medical scientists.
| Age | Grams |
| birth | about 15 grams; |
| puberty | about 35 grams |
| twenty-five years | 25 grams |
| sixty years | less than 15 grams |
| seventy years | about 0 grams |
Anatomy
The thymus is of a pinkish-gray color, soft, and lobulated on its surfaces. At birth it is about 5 cm in length, 4 cm in breadth, and about 6 mm in thickness. The organ enlarges during childhood, and atrophies at puberty.
The thymus will, if examined when its growth is most active, be found to consist of two lateral lobes placed in close contact along the middle line, situated partly in the thorax, partly in the neck, and extending from the fourth costal cartilage upward, as high as the lower border of the thyroid gland.
It is covered by the sternum, and by the origins of the sternohyoidei and sternothyreoidei.
Below, it rests upon the pericardium, being separated from the aortic arch and great vessels by a layer of fascia.
In the neck, it lies on the front and sides of the trachea, behind the sternohyoidei and sternothyreoidei.
The two lobes generally differ in size; they are occasionally united, so as to form a single mass, and sometimes separated by an intermediate lobe.
Structure


Each lateral lobe is composed of numerous lobules held together by delicate areolar tissue; the entire organ being enclosed in an investing capsule[5] of a similar but denser structure. The primary lobules vary in size from that of a pin's head to that of a small pea, and are made up of a number of small nodules or follicles.
The follicles are irregular in shape and are more or less fused together, especially toward the interior of the organ. Each follicle is from 1 to 2 mm in diameter and consists of a medullary and a cortical portion[6], and these differ in many essential particulars from each other.
Cortex
The cortical portion is mainly composed of lymphoid cells, supported by a network of finely-branched epithelial reticular cells, which is continuous with a similar network in the medullary portion. This network forms an adventitia to the blood vessels.
The cortex is the location of the earliest events in thymocyte development, where T cell receptor gene rearrangement and positive selection takes place.
Medulla
In the medullary portion, the reticulum is coarser than in the cortex, the lymphoid cells are relatively fewer in number, and there are found peculiar nest-like bodies, the concentric corpuscles of Hassall.[7] These concentric corpuscles are composed of a central mass, consisting of one or more granular cells, and of a capsule formed of epithelioid cells. They are the remains of the epithelial tubes, which grow out from the third branchial pouches of the embryo to form the thymus. Each follicle is surrounded by a vascular plexus, from which vessels pass into the interior, and radiate from the periphery toward the center, forming a second zone just within the margin of the medullary portion. In the center of the medullary portion there are very few vessels, and they are of minute size.
The medulla is the location of the latter events in thymocyte development. Thymocytes that reach the medulla have already successfully undergone T cell receptor gene rearrangement and positive selection, and have been exposed to a limited degree of negative selection. The medulla is specialised to allow thymocytes to undergo additional rounds of negative selection to remove auto-reactive T cells from the mature repertoire. The gene AIRE is expressed in the medulla, and drives the transcription of organ-specific genes such as insulin to allow maturing thymocytes to be exposed to a more complex set of self-antigens than is present in the cortex.
Vasculature
The arteries supplying the thymus are derived from the internal mammary, and from the superior thyroid and inferior thyroids.
The veins end in the left innominate vein, and in the thyroid veins.
The nerves are exceedingly minute; they are derived from the vagi and sympathetic nervous system. Branches from the descendens hypoglossi and phrenic reach the investing capsule, but do not penetrate into the substance of the organ.
Function
In the two thymic lobes, lymphocyte precursors from the bone-marrow become thymocytes, and subsequently mature into T cells. Once mature, T cells emigrate from the thymus and constitute the peripheral T cell repertoire responsible for directing many facets of the adaptive immune system. Loss of the thymus at an early age through genetic mutation or surgical removal results in severe immunodeficiency and a high susceptibility to infection. [8].
However up to January 2001, it was thought that whilst the thymus gland is important to the immune system in the developing foetus, the gland becomes redundant after birth, and so can be surgically excised without harm to the patient.[9]
The ability of T cells to recognize foreign antigens is mediated by the T cell receptor. The T cell receptor undergoes genetic rearrangement during thymocyte maturation, resulting in each T cell bearing a unique T cell receptor, specific to a limited set of peptide:MHC combinations. The random nature of the genetic rearrangement results in a requirement of central tolerance mechanisms to remove or inactivate those T cells which bear a T cell receptor with the ability to recognise self-peptides.
Phases of thymocyte maturation
The generation of T cells expressing distinct T cell receptors occurs within the thymus, and can be conceptually divided into three phases:
- A rare population of hematopoietic progenitors enters the thymus from the blood, and expands by cell division to generate a large population of immature thymocytes[10].
- Immature thymocytes each make distinct T cell receptors by a process of gene rearrangement. This process is error-prone, and some thymocytes fail to make functional T cell receptors, whereas other thymocytes make T cell receptors that are autoreactive. [11]. Growth factors include thymopoietin and thymosin.
- Immature thymocytes undergo a process of selection, based on the specificity of their T cell receptors. This involves selection of T cells that are functional (positive selection), and elimination of T cells that are autoreactive (negative selection).
| type: | functional (positive selection) | autoreactive (negative selection) |
| location: | cortex | medulla |
 |
In order to be positively-selected, thymocytes will have to interact with several cell surface molecules, MHC/HLA, to ensure reactivity and specificity[12]. Positive selection eliminates (apoptosis) weak binding cells and only takes high medium binding cells. (Binding refers to the ability of the T-cell receptors to bind to either MHC class I/II or peptide molecules.) |
Negative selection is not 100% complete. Some autoreactive T cells escape thymic censorship, and are released into the circulation. Additional mechanisms of tolerance active in the periphery exist to silence these cells such as anergy, deletion, and regulatory T cells. If these central tolerance mechanisms also fail, autoimmunity may arise. |
Cells that pass both levels of selection are released into the bloodstream to perform vital immune functions.
Cancer
Two primary forms of tumours originate in the thymus.
Tumours originating from the thymic epithelial cells are called thymomas, and are found in about 25-50% of patients with myasthenia gravis. Symptoms are sometimes confused with bronchitis or a strong cough because the tumor presses on the cough nerve. All thymomas are potentially cancerous, but they can vary a great deal. Some grow very slowly. Others grow rapidly and can spread to surrounding tissues. Treatment of thymomas often requires surgery to remove the entire thymus.
Tumours originating from the thymocytes are called thymic lymphomas.
X-ray
Patient #1: Radiograph demonstrates a normal thymus

Patient #2: Radiograph demonstrates the wave sign of a normal thymus

Other animals and second thymus
The thymus is also present in most vertebrates, with similar structure and function as the human thymus. Some animals have multiple secondary (smaller) thymi in the neck, this phenomenon has been reported for mice [13] and also occurs in 5 out of 6 human fetuses.[14] As in humans, the Guinea pig's thymus naturally atrophies as the animal reaches adulthood, but in the hairless "Skinny pig" breed (which arose from a spontaneous laboratory mutation) it often possesses no thymic tissue whatsoever, and the organ cavity is replaced with cystic spaces.
When animal thymic tissue is sold in a butcher shop or at a meat counter, thymus is known as sweetbread.
References
- ↑ Miller JF. Events that led to the discovery of T-cell development and function--a personal recollection. Tissue Antigens. 2004 Jun;63(6):509-17. full text
- ↑ Template:EmbryologySwiss
- ↑ Sutherland JS. Activation of thymic regeneration in mice and humans following androgen blockade. J Immunol 2005 15;175(4):2741-53
- ↑ Kumar, Parveen, Michael Clark (2002). Clinical Medicine 5th edn. Saunders. p. 1222. ISBN 0-702-02606-9.
- ↑ Histology image: 07403loa – Histology Learning System at Boston University
- ↑ Histology image: 07401loa – Histology Learning System at Boston University
- ↑ Histology at University of Southern California lymp/c_61
- ↑ Miller JF. The discovery of thymus function and of thymus-derived lymphocytes. Immunol Rev 185:7-14, 2002. full text
- ↑ Thymus glands
- ↑ Schwarz BA, Bhandoola A. Trafficking from the bone marrow to the thymus: a prerequisite for thymopoiesis. Immunol Rev 209:47, 2006. full text
- ↑ Sleckman BP, Lymphocyte antigen receptor gene assembly: multiple layers of regulation. Immunol Res 32:153-8, 2005. full text
- ↑ Baldwin TA, Hogquist KA, Jameson SC, The fourth way? Harnessing aggressive tendencies in the thymus. “J Immunol.” 173:6515-20, 2004. http://www.jimmunol.org/cgi/content/full/173/11/6515]
- ↑ Terszowski G et al. (2006) Evidence for a Functional Second Thymus in Mice. Science. 2 March 2006. PMID 16513945
- ↑ Surprise organ discovered in mice, Nature News, 2 March 2006
External links
Additional images
-
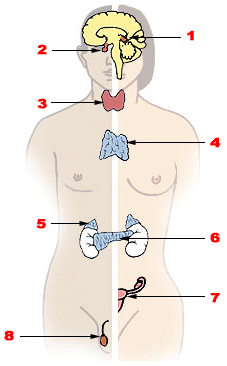
Endocrine system (thymus is #4)
-
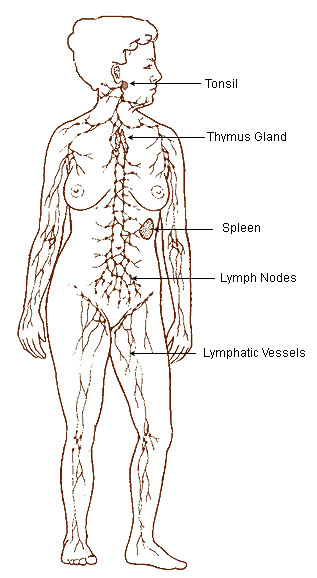
Lymphatic system
-
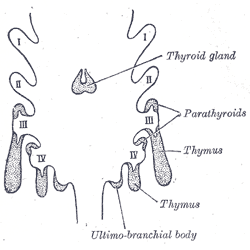
Scheme showing development of branchial epithelial bodies. I, II, III, IV. Branchial pouches.



Template:Lymphatic system Template:Grays
ar:غدة زعترية bg:Тимус ca:Tim da:Brissel de:Thymus et:Tüümus it:Timo (anatomia) he:בלוטת התימוס la:Thymus (membrum) lt:Užkrūčio liauka mk:Градна жлезда nl:Thymus (orgaan) no:Brisselen sk:Detská žľaza sr:Тимус fi:Kateenkorva sv:Bräss