Splenic infarction CT
|
Splenic infarction Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Splenic infarction CT On the Web |
|
American Roentgen Ray Society Images of Splenic infarction CT |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
CT
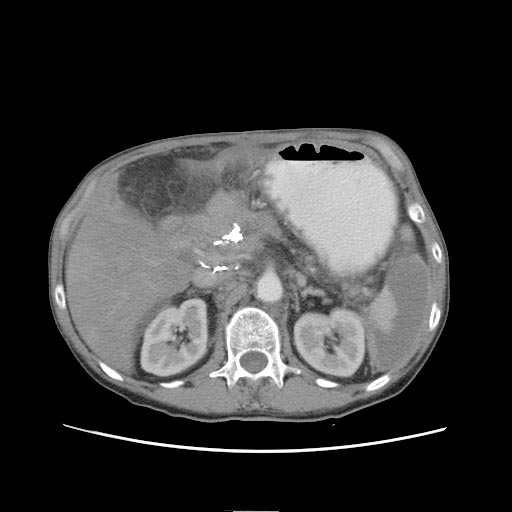
Computerized tomography scan is the current diagnostic modality of choice. Prior to the CT era, diagnosis of splenic infarct was made most commonly at laparotomy for intra-abdominal catastrophe or on postmortem examination. An abdominal CT scan is the most commonly used modality to confirm the diagnosis,although abdominal ultrasound can also contribute.[1][2][3] In CT; focal infarcts appear as wedge-shaped areas of decreased attenuation that extend to the surface of the spleen. Global infarction can manifest as diffuse areas of decreased attenuation in the spleen and can mimic splenic abscess or tumor. In some cases of global infarction, the splenic periphery remains enhanced due to perfusion from capsular vessels.
Patient #1 Note peripheral enhancement due to perfusion from capsular vessels
-

CT: Splenic infarction
-

CT: Splenic infarction
-

CT: Splenic infarction



Patient #2 Note peripheral enhancement due to perfusion from capsular vessels
-

CT: Splenic infarction
-

CT: Splenic infarction
-
CT: Splenic infarction



- Contrast studies clearly depict the classic segmental wedge-shaped, low-attenuation defect. Less frequently, the entire spleen may be infarcted, leaving only a rim of contrast-enhancing capsule.
- Other modes of diagnosis include radioisotope scans and ultrasound evaluation of the spleen.
References
- ↑ Görg C, Seifart U, Görg K (2004). "Acute, complete splenic infarction in cancer patient is associated with a fatal outcome". Abdom Imaging. 29 (2): 224–7. doi:10.1007/s00261-003-0108-9. PMID 15290950.
- ↑ O'Keefe JH, Holmes DR, Schaff HV, Sheedy PF, Edwards WD (1986). "Thromboembolic splenic infarction". Mayo Clin. Proc. 61 (12): 967–72. PMID 3773568. Unknown parameter
|month=ignored (help) - ↑ Frippiat F, Donckier J, Vandenbossche P, Stoffel M, Boland B, Lambert M (1996). "Splenic infarction: report of three cases of atherosclerotic embolization originating in the aorta and retrospective study of 64 cases". Acta Clin Belg. 51 (6): 395–402. PMID 8997756.