Perampanel
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
WARNING
See full prescribing information for complete Boxed Warning.
SERIOUS PSYCHIATRIC AND BEHAVIORAL REACTIONS:
|
Overview
Perampanel is a non-competitive AMPA glutamate receptor antagonist that is FDA approved for the {{{indicationType}}} of partial-onset seizures with or without secondarily generalized seizures in patients with epilepsy aged 12 years and older. There is a Black Box Warning for this drug as shown here. Common adverse reactions include dizziness, somnolence, fatigue, irritability, falls, nausea, weight gain, vertigo, ataxia, gait disturbance, and balance disorder.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Partial-Onset Seizures
- In the Absence of Enzyme-Inducing AEDs
- The recommended starting dosage of FYCOMPA is 2 mg once daily taken orally at bedtime. Increase dosage by 2 mg per day increments no more frequently than every week to a dose of 4 mg to 8 mg once daily taken at bedtime. In elderly patients, dosage increases during titration are recommended no more frequently than every two weeks.
- The recommended dose range is 8 mg to 12 mg once daily. A dose of 12 mg once daily resulted in somewhat greater reductions in seizure rates than the dose of 8 mg once daily, but with a substantial increase in adverse reactions. Individual dosing should be adjusted based on clinical response and tolerability
- In the Presence of Enzyme-Inducing AEDs
- The recommended starting dosage of FYCOMPA in the presence of enzyme-inducing AEDs, including phenytoin, carbamazepine, and oxcarbazepine, is 4 mg and patients should be monitored closely for response. Clinical trials revealed a substantially reduced effect on seizure rates in these patients. The reduction in seizure frequency was somewhat greater at 12 mg than at 8 mg.
- When these enzyme-inducing AEDs are introduced or withdrawn from a patient’s treatment regimen, patient should be closely monitored for clinical response and tolerability. Dose adjustment of FYCOMPA may be necessary.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Perampanel in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Perampanel in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Partial-Onset Seizures
- In the Absence of Enzyme-Inducing AEDs
- The recommended starting dosage of FYCOMPA is 2 mg once daily taken orally at bedtime. Increase dosage by 2 mg per day increments no more frequently than every week to a dose of 4 mg to 8 mg once daily taken at bedtime. In elderly patients, dosage increases during titration are recommended no more frequently than every two weeks.
- The recommended dose range is 8 mg to 12 mg once daily. A dose of 12 mg once daily resulted in somewhat greater reductions in seizure rates than the dose of 8 mg once daily, but with a substantial increase in adverse reactions. Individual dosing should be adjusted based on clinical response and tolerability
- In the Presence of Enzyme-Inducing AEDs
- The recommended starting dosage of FYCOMPA in the presence of enzyme-inducing AEDs, including phenytoin, carbamazepine, and oxcarbazepine, is 4 mg and patients should be monitored closely for response. Clinical trials revealed a substantially reduced effect on seizure rates in these patients. The reduction in seizure frequency was somewhat greater at 12 mg than at 8 mg.
- When these enzyme-inducing AEDs are introduced or withdrawn from a patient’s treatment regimen, patient should be closely monitored for clinical response and tolerability. Dose adjustment of FYCOMPA may be necessary.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Perampanel in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Perampanel in pediatric patients.
Contraindications
- None.
Warnings
|
WARNING
See full prescribing information for complete Boxed Warning.
SERIOUS PSYCHIATRIC AND BEHAVIORAL REACTIONS:
|
Precautions
- Serious Psychiatric and Behavioral Reactions
- In the controlled Phase 3 epilepsy clinical trials, hostility- and aggression-related adverse reactions occurred in 12% and 20% of patients randomized to receive FYCOMPA at doses of 8 mg and 12 mg/day, respectively, compared to 6% of patients in the placebo group. These effects were dose-related and generally appeared within the first 6 weeks of treatment, although new events continued to be observed through more than 37 weeks. FYCOMPA-treated patients experienced more hostility- and aggression - related adverse reactions that were serious, severe, and led to dose reduction, interruption, and discontinuation more frequently than placebo-treated patients.
- In general, in placebo-controlled Phase 3 epilepsy trials, neuropsychiatric events were reported more frequently in patients being treated with FYCOMPA than in patients taking placebo. These events included irritability, aggression, anger, and anxiety which occurred in 2% or greater of perampanel treated patients and twice as frequently as in placebo-treated patients. Other symptoms that were observed with perampanel treatment and more commonly than with placebo, included belligerence, affect lability, agitation, and physical assault. Some of these events were reported as serious and life-threatening. Homicidal ideation and/or threat were exhibited in 0.1% of 4,368 perampanel treated patients in controlled and open label studies, including non-epilepsy studies.
- In the Phase 3 epilepsy trials these events occurred in patients with and without prior psychiatric history, prior aggressive behavior, or concomitant use of medications associated with hostility and aggression. Some patients experienced worsening of their pre-existing psychiatric conditions. Patients with active psychotic disorders and unstable recurrent affective disorders were excluded from the clinical trials. The combination of alcohol and perampanel significantly worsened mood and increased anger. Patients taking FYCOMPA should avoid the use of alcohol.
- In healthy volunteers taking FYCOMPA, observed psychiatric events included paranoia, euphoric mood, agitation, anger, mental status changes, and disorientation/confusional state.
- In the non-epilepsy trials, psychiatric events that occurred in perampanel-treated subjects more often than placebo-treated subjects included disorientation, delusion, and paranoia.
- Patients, their caregivers, and families should be informed that FYCOMPA may increase the risk of psychiatric events. Patients should be monitored during treatment and for at least one month after the last dose of FYCOMPA, and especially when taking higher doses and during the initial few weeks of drug therapy (titration period) or at other times of dose increases. Dose of FYCOMPA should be reduced if these symptoms occur. Permanently discontinue FYCOMPA for persistent severe or worsening psychiatric symptoms or behaviors and refer for psychiatric evaluation.
- Suicidal Behavior and Ideation
- Antiepileptic drugs (AEDs), including FYCOMPA, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
- Pooled analyses of 199 placebo-controlled clinical trials (mono- and adjunctive therapy) of 11 different AEDs showed that patients randomized to one of the AEDs had approximately twice the risk (adjusted Relative Risk 1.8, 95% CI: 1.2, 2.7) of suicidal thinking or behavior compared to patients randomized to placebo. In these trials, which had a median treatment duration of 12 weeks, the estimated incidence of suicidal behavior or ideation among 27,863 AED-treated patients was 0.43%, compared to 0.24% among 16,029 placebo-treated patients, representing an increase of approximately one case of suicidal thinking or behavior for every 530 patients treated. There were four suicides in drug-treated patients in the trials and none in placebo-treated patients, but the number is too small to allow any conclusion about drug effect on suicide.
- The increased risk of suicidal thoughts or behavior with AEDs was observed as early as one week after starting drug treatment with AEDs and persisted for the duration of treatment assessed. Because most trials included in the analysis did not extend beyond 24 weeks, the risk of suicidal thoughts or behavior beyond 24 weeks could not be assessed.
- The risk of suicidal thoughts or behavior was generally consistent among drugs in the data analyzed. The finding of increased risk with AEDs of varying mechanisms of action and across a range of indications suggests that the risk applies to all AEDs used for any indication. The risk did not vary substantially by age (5-100 years) in the clinical trials analyzed.
- Table 1 shows absolute and relative risk by indication for all evaluated AEDs.
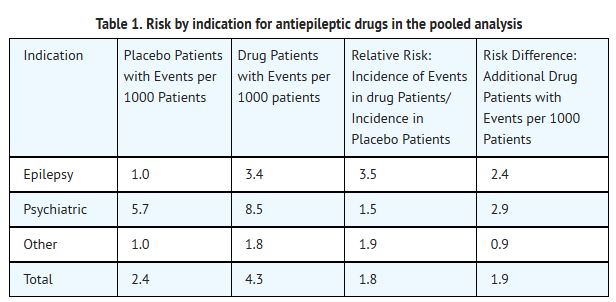
This image is provided by the National Library of Medicine.

- The relative risk for suicidal thoughts or behavior was higher in clinical trials for epilepsy than in clinical trials for psychiatric or other conditions, but the absolute risk differences were similar for the epilepsy and psychiatric indications.
- Anyone considering prescribing FYCOMPA or any other AED must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
- Patients, their caregivers, and families should be informed that AEDs increase the risk of suicidal thoughts and behavior and should be advised of the need to be alert for the emergence or worsening of the signs and symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm. Behaviors of concern should be reported immediately to healthcare providers.
- Neurologic Effects
- Dizziness and Gait Disturbance
- FYCOMPA caused dose-related increases in events related to dizziness and disturbance in gait or coordination. In the controlled Phase 3 epilepsy clinical trials, dizziness and vertigo were reported in 35% and 47% of patients randomized to receive FYCOMPA at doses of 8 mg and 12 mg/day, respectively, compared to 10% of placebo-treated patients. The gait disturbance related events (including ataxia, gait disturbance, balance disorder, and coordination abnormal) were reported in 12% and 16% of patients randomized to receive FYCOMPA at doses of 8 mg and 12 mg/day, respectively, compared to 2% of placebo-treated patients.
- These adverse reactions occurred mostly during the titration phase and led to discontinuation in 3% of perampanel-treated subjects compared to 1% of placebo-treated patients. Elderly patients had an increased risk of these adverse reactions compared to younger adults and adolescents.
- Somnolence and Fatigue
- FYCOMPA caused dose-dependent increases in somnolence and fatigue-related events (including fatigue, asthenia, and lethargy).
- In the controlled Phase 3 epilepsy clinical trials, 16% and 18% of patients randomized to receive FYCOMPA at doses of 8 mg and 12 mg/day, respectively, reported somnolence compared to 7% of placebo patients. In the controlled Phase 3 epilepsy clinical trials, 12% and 15% of patients randomized to receive FYCOMPA at doses of 8 mg and 12 mg/day, respectively, reported fatigue-related events compared to 5% of placebo patients. Somnolence or fatigue-related events led to discontinuation in 2% of perampanel-treated patients and 0.5% of placebo-treated patients. Elderly patients had an increased risk of these adverse reactions compared to younger adults and adolescents.
- Risk Amelioration
- Prescribers should advise patients against engaging in hazardous activities requiring mental alertness, such as operating motor vehicles or dangerous machinery, until the effect of FYCOMPA is known.
- In the controlled Phase 3 epilepsy clinical trials these adverse reactions occurred mostly during the titration phase.
- Falls
- An increased risk of falls, in some cases leading to serious injuries including head injuries and bone fracture, occurred in patients being treated with FYCOMPA (with and without concurrent seizures). In the controlled Phase 3 epilepsy clinical trials, falls were reported in 5% and 10% of patients randomized to receive FYCOMPA at doses of 8 mg and 12 mg/day, respectively, compared to 3% of placebo-treated patients. Falls were reported as serious and led to discontinuation more frequently in FYCOMPA-treated patients than placebo-treated patients. Elderly patients had an increased risk of falls compared to younger adults and adolescents.
- Withdrawal of Antiepileptic Drugs
- There is the potential of increased seizure frequency in patients with seizure disorders when antiepileptic drugs are withdrawn abruptly. FYCOMPA has a half-life of approximately 105 hours so that even after abrupt cessation, blood levels fall gradually. In antiepileptic clinical trials FYCOMPA was withdrawn without down-titration. Although a small number of patients exhibited seizures following discontinuation, the data were not sufficient to allow any recommendations regarding appropriate withdrawal regimens. A gradual withdrawal is generally recommended with antiepileptic drugs, but if withdrawal is a response to adverse events, prompt withdrawal can be considered.
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
- A total of 1,038 patients on perampanel (2, 4, 8, or 12 mg once daily) constituted the safety population in the pooled analysis of Phase 3 placebo controlled studies (Studies 1, 2, and 3) in patients with partial onset seizures. Approximately 51% of patients were female and the mean age was 35 years.
- Adverse Reactions Leading to Discontinuation
- In controlled Phase 3 clinical trials (Studies 1, 2, and 3), the rate of discontinuation as a result of an adverse reaction was 3%, 8% and 19% in patients randomized to receive FYCOMPA at the recommended doses of 4 mg, 8 mg and 12 mg/day, respectively, and 5% in patients randomized to receive placebo [see Clinical Studies (14)]. The adverse events most commonly leading to discontinuation (≥1% in the 8 mg or 12 mg FYCOMPA group and greater than placebo) were dizziness, somnolence, vertigo, aggression, anger, ataxia, blurred vision, irritability, and dysarthria.
- Most Common Adverse Reactions
- Table 2 gives the incidence in the Phase 3 controlled trials (Studies 1, 2, and 3) of the adverse reactions that occurred in ≥2% of patients with partial-onset seizures in any FYCOMPA dose group. Overall, the most frequently reported dose-related adverse reactions in patients receiving FYCOMPA at doses of 8 mg or 12 mg (≥4% and occurring at least 1% higher than the placebo group) included dizziness (36%), somnolence (16%), fatigue (10%), irritability (9%), falls (7%), nausea (7%), ataxia (5%), balance disorder (4%), gait disturbance (4%), vertigo (4%), and weight gain (4%). For almost every adverse reaction, rates were higher on 12 mg and more often led to dose reduction or discontinuation.
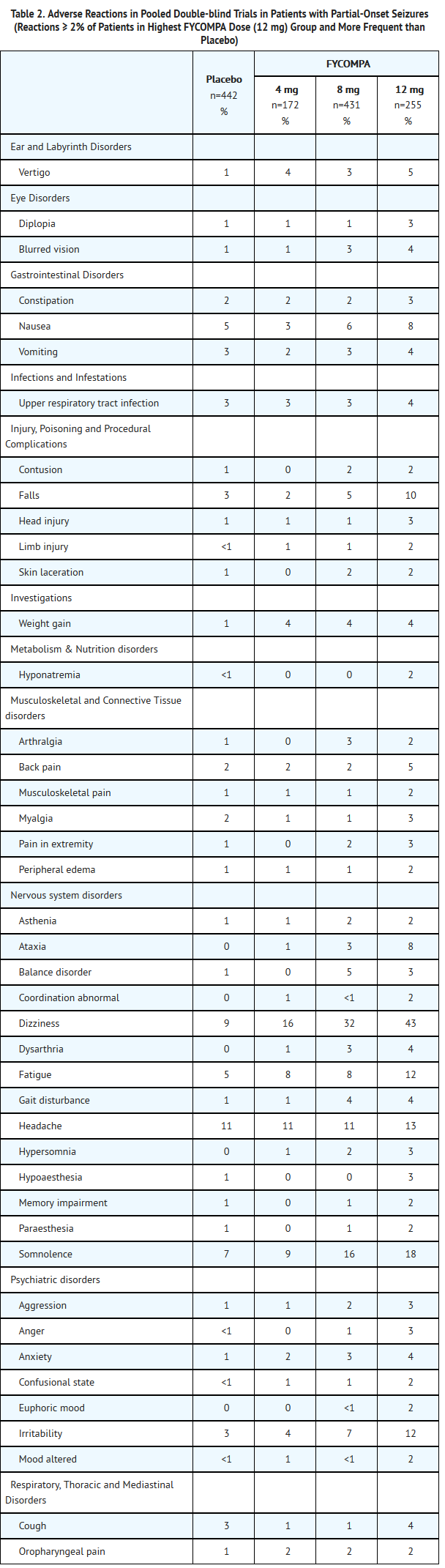
This image is provided by the National Library of Medicine.

- Weight Gain
- Weight gain has been observed with FYCOMPA use in adults.
- In the controlled Phase 3 epilepsy clinical trials, FYCOMPA-treated adults gained an average of 1.1 kg (2.5 lbs) compared to an average of 0.3 kg (0.7 lbs) in placebo-treated adults with a median exposure of 19 weeks. The percentages of adults who gained at least 7% and 15% of their baseline body weight in FYCOMPA-treated patients were 9.1% and 0.9%, respectively, as compared to 4.5% and 0.2% of placebo-treated patients, respectively.
- Clinical monitoring of weight is recommended.
- Comparison of Sex and Race
- No significant sex differences were noted in the incidence of adverse reactions.
- Although there were few non-Caucasian patients, no differences in the incidences of adverse reactions compared to Caucasian patients were observed.
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Perampanel in the drug label.
Drug Interactions
- Contraceptives
- With concomitant use, FYCOMPA at a dose of 12 mg/day reduced levonorgestrel exposure by approximately 40%. Use of FYCOMPA with oral or implant contraceptives containing levonorgestrel may render them less effective. Additional non-hormonal forms of contraception are recommended.
- Cytochrome P450 (CYP) Inducers
- The concomitant use of known CYP enzyme inducers including carbamazepine, phenytoin, or oxcarbazepine with FYCOMPA decreased the plasma levels of perampanel by approximately 50~67%. The starting doses for FYCOMPA should be increased in the presence of enzyme-inducing AEDs.
- When these enzyme-inducing AEDs are introduced or withdrawn from a patient’s treatment regimen, patient should be closely monitored for clinical response and tolerability. Dose adjustment of FYCOMPA may be necessary. As noted, however, the decrease in the therapeutic effect seen in patients on concomitant treatment was not affected by use of higher doses (8 mg to 12 mg).
- Concomitant use of FYCOMPA with other strong CYP3A inducers (e.g., rifampin, St. John’s wort) should be avoided.
- Alcohol and Other CNS Depressants
- The concomitant use of FYCOMPA and CNS depressants including alcohol may increase CNS depression. A pharmacodynamic interaction study in healthy subjects found that the effects of FYCOMPA on complex tasks such as driving ability were additive or supra-additive to the impairment effects of alcohol. Multiple dosing of FYCOMPA 12 mg/day also enhanced the effects of alcohol to interfere with vigilance and alertness, and increased levels of anger, confusion, and depression. These effects may also be seen when FYCOMPA is used in combination with other CNS depressants. Care should be taken when administering FYCOMPA with these agents. Patients should limit activity until they have experience with concomitant use of CNS depressants (e.g., benzodiazepines, narcotics, barbiturates, sedating antihistamines). Advise patients not to drive or operate machinery until they have gained sufficient experience on FYCOMPA to gauge whether it adversely affects these activities.
Use in Specific Populations
Pregnancy
- Pregnancy Category C
- There are no adequate and well-controlled studies in pregnant women. In animal studies, perampanel induced developmental toxicity in pregnant rat and rabbit at clinically relevant doses. FYCOMPA should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Oral administration of perampanel (1, 3, or 10 mg/kg/day) to pregnant rats throughout organogenesis resulted in an increase in visceral abnormalities (diverticulum of the intestine) at all doses tested. In a dose-ranging study at higher oral doses (10, 30, or 60 mg/kg/day), embryo lethality and reduced fetal body weight were observed at the mid and high doses tested. The lowest dose tested (1 mg/kg/day) is similar to a human dose of 8 mg/day based on body surface area (mg/m2).
- Upon oral administration of perampanel (1, 3, or 10 mg/kg/day) to pregnant rabbits throughout organogenesis, embryo lethality was observed at the mid and high doses tested; the no effect dose for embryo-fetal developmental toxicity in rabbit (1 mg/kg/day) is approximately 2 times a human dose of 8 mg/day based on body surface area (mg/m2).
- Oral administration of perampanel (1, 3, or 10 mg/kg/day) to rats throughout gestation and lactation resulted in fetal and pup deaths at the mid and high doses and delayed sexual maturation in males and females at the highest dose tested. No effects were observed on measures of neurobehavioral or reproductive function in the offspring. The no-effect dose for pre- and postnatal developmental toxicity in rat (1 mg/kg/day) is similar to a human dose of 8 mg/day based on body surface area (mg/m2).
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Perampanel in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Perampanel during labor and delivery.
Nursing Mothers
- Perampanel and/or its metabolites are excreted in rat milk, and are detected at concentrations higher than that in maternal plasma. It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when FYCOMPA is administered to a nursing woman.
Pediatric Use
- The safety and efficacy of FYCOMPA for the adjunctive therapy of partial-onset seizures was established by three randomized double blind, placebo-controlled, multicenter studies which included 72 pediatric patients between 12 and 16 years old exposed to perampanel. The safety and effectiveness of FYCOMPA in pediatric patients <12 years old have not been established.
- Juvenile Animal Data
- Oral administration of perampanel (1, 3, 3/10/30 mg/kg/day; high dose increased on postnatal days [PND] 28 and 56) to young rats for 12 weeks starting on PND 7 resulted in reduced body weight, reduced growth, neurobehavioral impairment (water maze performance and auditory startle habituation) at the mid and high doses, and delayed sexual maturation at the high doses. CNS signs (reduced activity, incoordination, excessive grooming/scratching), pup death, decreased hindlimb splay, and decreased hindlimb grip strength were observed at all doses. Effects on pup body weight, pup growth, hindlimb splay, impairment in the water maze performance and auditory startle persisted after dosing was stopped. A no-effect dose for postnatal developmental toxicity was not identified in this study.
- Oral administration of perampanel (1, 5, 5/10 mg/kg/day; high dose increased on PND 56) to juvenile dogs for 33 weeks, starting on PND 42, resulted in CNS signs (incoordination, excessive grooming/licking/scratching, spatial disorientation, and/or ataxic gait) at all doses tested.
Geriatic Use
- Clinical studies of FYCOMPA did not include sufficient numbers of patients aged 65 and over to determine the safety and efficacy of FYCOMPA in the elderly population. Because of increased likelihood for adverse reactions in the elderly, dosing titration should proceed slowly in patients aged 65 years and older.
Gender
There is no FDA guidance on the use of Perampanel with respect to specific gender populations.
Race
There is no FDA guidance on the use of Perampanel with respect to specific racial populations.
Renal Impairment
- Dose adjustment is not required in patients with mild renal impairment. FYCOMPA should be used with caution in patients with moderate renal impairment and slower titration may be considered. Use in patients with severe renal impairment or patients undergoing hemodialysis is not recommended.
Hepatic Impairment
- Use of FYCOMPA in patients with severe hepatic impairment is not recommended and dosage adjustments are recommended in patients with mild or moderate hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Perampanel in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Perampanel in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
There is limited information regarding Monitoring of Perampanel in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Perampanel in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- There is limited clinical experience with FYCOMPA overdose. The highest reported overdose (approximately 264 mg) was intentional. This patient experienced serious adverse reactions of altered mental status, agitation, and aggressive behavior and recovered without sequelae. In general, the adverse reactions associated with overdoses were similar to the reactions at therapeutic doses with dizziness reported most frequently. There were no reported sequelae.
Management
- There is no available specific antidote to the overdose reactions of FYCOMPA. In the event of overdose, standard medical practice for the management of any overdose should be used. An adequate airway, oxygenation, and ventilation should be ensured; monitoring of cardiac rhythm and vital sign measurement is recommended. A certified poison control center should be contacted for updated information on the management of overdose with FYCOMPA. Due to its long half-life, the reactions caused by FYCOMPA could be prolonged.
Chronic Overdose
There is limited information regarding Chronic Overdose of Perampanel in the drug label.
Pharmacology

| |
Perampanel
| |
| Systematic (IUPAC) name | |
| 5'-(2-cyanophenyl)-1'-phenyl-2,3'-bipyridinyl-6'(1'H)-one | |
| Identifiers | |
| CAS number | |
| ATC code | N03 |
| PubChem | |
| Chemical data | |
| Formula | Template:OrganicBox atomTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBox atomTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBoxTemplate:OrganicBox |
| Mol. mass | 349.384 g/mol |
| SMILES | & |
| Synonyms | E2007 |
| Pharmacokinetic data | |
| Bioavailability | 116%[1] |
| Protein binding | 95–96% |
| Metabolism | hepatic, mostly via CYP3A4 and/or CYP3A5 |
| Half life | 105 hrs, 295 hrs (moderate hepatic impairment) |
| Excretion | 70% faeces, 30% urine |
| Therapeutic considerations | |
| Licence data |
, |
| Pregnancy cat. |
C(US) |
| Legal status | |
| Routes | ? |
Mechanism of Action
- Perampanel is a non-competitive antagonist of the ionotropic α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) glutamate receptor on postsynaptic neurons. Glutamate is the primary excitatory neurotransmitter in the central nervous system and is implicated in a number of neurological disorders caused by neuronal over excitation.
- The precise mechanism by which FYCOMPA exerts its antiepileptic effects in humans has not been fully elucidated.
Structure
- FYCOMPA tablets contain perampanel, a non-competitive AMPA receptor antagonist. Perampanel is described chemically as 2-(2-oxo-1-phenyl-5-pyridin-2-yl-1,2-dihydropyridin-3-yl) benzonitrile hydrate (4:3).
- The molecular formula is C23H15N3O • 3/4H2O, and the molecular weight is 362.90 (3/4 hydrate). The chemical structure of perampanel is:
This image is provided by the National Library of Medicine.

- Perampanel is a white to yellowish white powder. It is freely soluble in N-methylpyrrolidone, sparingly soluble in acetonitrile and acetone, slightly soluble in methanol, ethanol and ethyl acetate, very slightly soluble in 1-octanol and diethyl ether and practically insoluble in heptane and water.
- FYCOMPA (perampanel) tablets are round, bi-convex, film coated tablets containing 2 mg, 4 mg, 6 mg, 8 mg, 10 mg or 12 mg of perampanel. Tablets contain the following inactive ingredients: lactose monohydrate, low substituted hydroxypropyl cellulose, povidone, microcrystalline cellulose, magnesium stearate, hypromellose, polyethylene glycol, talc and titanium dioxide. Tablets of different strengths also may contain yellow ferric oxide (10 mg and 2 mg), red ferric oxide (2 mg, 4 mg, 6 mg, 8 mg), black ferric oxide (8 mg) and FD&C blue # 2 indigo carmine aluminum lake (10 mg and 12 mg).
Pharmacodynamics
- Psychomotor Performance
- In a healthy volunteer study to assess the effects of FYCOMPA on psychomotor performance using a standard battery of assessments including simulated driving, single and multiple daily doses of FYCOMPA 4 mg did not impair simple psychomotor tasks, driving performance or sensori-motor coordination. Single and multiple doses of 8 mg and 12 mg impaired psychomotor performance in a dose-related manner. Car handling ability was impaired after dosing of FYCOMPA 12 mg, but postural stability was not significantly impaired. Performance testing returned to baseline within 2 weeks of cessation of FYCOMPA dosing.
- Interactions with Alcohol
- In the above study, when administered to healthy subjects receiving alcohol to achieve a blood concentration of 80-100mg/100mL, FYCOMPA consistently impaired simple psychomotor performance after single doses of 4 to 12 mg, and after 21 days of multiple 12 mg/day doses. The effects of FYCOMPA on complex tasks such as driving ability were additive or supra-additive to the impairment effects of alcohol. FYCOMPA enhanced the effects of alcohol on vigilance and alertness, and increased levels of anger, confusion, and depression.
- Potential to Prolong QT Interval
- In a placebo-controlled thorough QT study perampanel in healthy subjects, there was no evidence that perampanel caused QT interval prolongation of clinical significance at doses of 6 or 12 mg (i.e., the upper bound of the 95% confidence interval for the largest placebo-adjusted baseline-corrected QTc was below 10 msec). The exposures observed with the 12 mg dose in this study will not cover the exposures expected in patients with hepatic impairment taking doses over 6 mg/day. At the maximum recommended dose (12 mg), perampanel did not prolong the QTc interval to any clinically relevant extent.
Pharmacokinetics
- Pharmacokinetics of perampanel are similar in healthy subjects and patients with partial-onset seizures. The half-life of perampanel is about 105 hours, so that steady state is reached in about 2-3 weeks. AUC of perampanel increased in a dose-proportional manner after single-dose administration of 0.2-12 mg and after multiple-dose administration of 1-12 mg once daily.
- Absorption
- Perampanel is rapidly and completely absorbed after oral administration with negligible first-pass metabolism. Median Tmax ranged from 0.5 to 2.5 hours under fasted condition. Food does not affect the extent of absorption (AUC), but slows the rate of absorption. Under fed conditions, Cmax of perampanel was decreased by 28-40% and Tmax was delayed by 2-3 hours compared to that under fasted conditions.
- Distribution
- Data from in vitro studies indicate that, in the concentration range of 20 to 2000 ng/mL, perampanel is approximately 95-96% bound to plasma proteins, mainly bound to albumin and α1-acid glycoprotein. Blood to plasma ratio of perampanel is 0.55-0.59.
- Metabolism
- Perampanel is extensively metabolized via primary oxidation and sequential glucuronidation. Oxidative metabolism is primarily mediated by CYP3A4/5 and to a lesser extent by CYP1A2 and CYP2B6, based on results of in vitro studies using recombinant human CYPs and human liver microsomes. Other CYP enzymes may also be involved.
- Following administration of radiolabeled perampanel, unchanged perampanel accounted for 74-80% of total radioactivity in systemic circulation, whereas only trace amounts of individual perampanel metabolites were detected in plasma.
- Elimination
- Following administration of a radiolabeled perampanel dose to 8 healthy elderly subjects, 22% of administered radioactivity was recovered in the urine and 48% in the feces. In urine and feces, recovered radioactivity was primarily composed of a mixture of oxidative and conjugated metabolites. Population pharmacokinetic analysis of pooled data from 19 Phase 1 studies reported that t1/2 of perampanel was 105 hours on average. Apparent clearance of perampanel in healthy subjects and patients was approximately 12 mL/min.
- Specific Populations
- Hepatic Impairment
- The pharmacokinetics of perampanel following a single 1 mg dose were evaluated in 12 subjects with mild and moderate hepatic impairment (Child-Pugh A and B, respectively) compared with 12 demographically matched healthy subjects. The total (free and protein bound) exposure (AUC0-inf) of perampanel was 50% greater in subjects with mild hepatic impairment and more than doubled (2.55-fold) in subjects with moderate hepatic impairment compared to their healthy controls. The AUC0-inf of free perampanel in subjects with mild and moderate hepatic impairment was 1.8-fold and 3.3-fold, respectively, of those in matched healthy controls. The t1/2 was prolonged in subjects with mild impairment (306 vs. 125 hours) and moderate impairment (295 vs. 139 hours). Perampanel has not been studied in subjects with severe hepatic impairment.
- Renal Impairment
- A dedicated study has not been conducted to evaluate the pharmacokinetics of perampanel in patients with renal impairment. Population pharmacokinetic analysis was performed on pooled data from patients with partial-onset seizures and receiving FYCOMPA up to 12 mg/day in placebo-controlled clinical trials. Results showed that perampanel apparent clearance was decreased by 27% in patients with mild renal impairment (creatinine clearance 50-80 mL/min) compared to patients with normal renal function (creatinine clearance >80 mL/min), with a corresponding 37% increase in AUC. Considering the substantial overlap in the exposure between normal and mildly impaired patients, no dosage adjustment is necessary for patients with mild renal impairment. Perampanel has not been studied in patients with severe renal impairment and patients undergoing hemodialysis.
- Sex
- In a population pharmacokinetic analysis of patients with partial-onset seizures receiving FYCOMPA in placebo-controlled clinical trials, perampanel apparent clearance in females (0.605 L/hr) was 17% lower than in males (0.730 L/hr). No dosage adjustment is necessary based on sex.
- Pediatric Patients
- FYCOMPA has not been studied in patients <12 years old. In a population pharmacokinetic analysis of patients with partial-onset seizures ranging in age from 12 to 74 years receiving FYCOMPA in placebo-controlled trials, apparent clearance of perampanel in adolescents (0.787 L/hr) was slightly, but not significantly, higher than that in adults. Pediatric patients above 12 years old can be dosed similarly to adults.
- Geriatrics
- In a population pharmacokinetic analysis of patients with partial-onset seizures ranging in age from 12 to 74 years receiving FYCOMPA in placebo-controlled trials, no significant effect of age on perampanel apparent clearance was found.
- Race
- In a population pharmacokinetic analysis of patients with partial-onset seizures which included 576 Caucasians, 14 Blacks, 97 non-Chinese Asians, and 62 Chinese receiving FYCOMPA in placebo-controlled trials, no significant effect of race on perampanel apparent clearance was found. No dosage adjustment is necessary.
- Drug Interaction Studies
- In Vitro Assessment of Drug Interactions
- Drug Metabolizing Enzymes
- In human liver microsomes, perampanel at a concentration of 30 μmol/L, about 10 fold the steady state Cmax at a 12 mg dose, had a weak inhibitory effect on CYP2C8, CYP3A4, UGT1A9 and UGT2B7. Perampanel did not inhibit CYP1A2, CYP2A6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, UGT1A1, UGT1A4, and UGT1A6 at a concentration of 30 µmol/L.
- Compared with positive controls (including phenobarbital and rifampin), perampanel was found to weakly induce CYP2B6 (30µmol/L) and CYP3A4/5 (≥ 3µmol/L) in cultured human hepatocytes. Perampanel also induced UGT1A1 (≥ 3µmol/L) and UGT1A4 (30µmol/L). Perampanel did not induce CYP1A2 at concentrations up to 30 µmol/L.
- Transporters
- In vitro studies showed that perampanel is not a substrate or significant inhibitor of the following: organic anion transporting polypeptides 1B1 and 1B3; organic anion transporters 1, 2, 3, and 4; organic cation transporters 1, 2, and 3; efflux transporters P-glycoprotein and Breast Cancer Resistance Protein.
- In Vivo Assessment of Drug Interactions
- Drug Interactions with AEDs
- Effect of concomitant AEDs on FYCOMPA:
- Carbamazepine. As an inducer of CYP enzymes, carbamazepine increases perampanel clearance. Steady state administration of carbamazepine at 300 mg BID in healthy subjects reduced the Cmax and AUC0-inf of a single 2 mg dose of perampanel by 26% and 67% respectively. The t1/2 of perampanel was shortened from 56.8 hours to 25 hours. In clinical studies examining partial-onset seizures, a population pharmacokinetic analysis showed that perampanel AUC was reduced by 67% in patients on carbamazepine compared to the AUC in patients not on enzyme-inducing AEDs.
- Oxcarbazepine. In clinical studies examining partial-onset seizures, a population pharmacokinetic analysis showed that perampanel AUC was reduced by half in patients on oxcarbazepine compared to patients not on enzyme-inducing AEDs.
- Phenytoin. In clinical studies examining partial-onset seizures, a population pharmacokinetic analysis showed that perampanel AUC was reduced by half in patients on phenytoin compared to patients not on enzyme-inducing AEDs.
- Phenobarbital and Primidone: In a population pharmacokinetic analysis of patients with partial-onset seizures in clinical trials (37 patients coadministered phenobarbital and 9 patients coadministered primidone) no significant effect on perampanel AUC was found. A modest effect of phenobarbital and primidone on perampanel concentrations cannot be excluded.
- Topiramate: Population pharmacokinetic analysis of patients with partial-onset seizures in clinical trials showed that perampanel AUC was reduced by approximately 20% in patients on topiramate compared to patients not on enzyme-inducing AEDs.
- Other AEDs: Population pharmacokinetic analysis of patients with partial-onset seizures in clinical trials showed that clobazam, clonazepam, lamotrigine, levetiracetam, valproate, and zonisamide did not have an effect on perampanel clearance.
- Other strong CYP3A inducers (e.g., rifampin, St. John’s wort) may also greatly increase clearance of perampanel and reduce perampanel plasma concentrations.
- Effect of FYCOMPA on concomitant AEDs:
- FYCOMPA up to 12 mg/day did not significantly affect the clearance of clonazepam, levetiracetam, phenobarbital, phenytoin, topiramate, or zonisamide based on a population pharmacokinetic analysis of patients with partial-onset seizures in clinical trials. FYCOMPA had a statistically significant effect on the clearance of carbamazepine, clobazam, lamotrigine, and valproic acid, but the increases in clearance of these drugs were each less than 10% at the highest perampanel dose evaluated (12 mg/day). FYCOMPA coadministration resulted in a 26% decrease in oxcarbazepine clearance and increased its concentrations. The concentrations of 10-monohydroxy metabolite (MHD), the active metabolite of oxcarbazepine, were not measured.
- Drug-drug interaction studies with other drugs
- Effect of other drugs on FYCOMPA
- Ketoconazole. Coadministration of single 1-mg dose of perampanel with 400 mg once daily doses of ketoconazole, a strong CYP3A4 inhibitor, for 8 days in healthy subjects prolonged perampanel t1/2 by 15% (67.8 vs. 58.4 hours) and increased AUC0-inf by 20%.
- Oral contraceptives. Perampanel Cmax and AUC0-72h were not altered when a single 6-mg dose of perampanel was administered to healthy female subjects following a 21-day course of oral contraceptives containing ethinylestradiol 30 µg and levonorgestrel 150 µg.
- Effect of FYCOMPA on other drugs
- Midazolam. Perampanel administered as 6 mg once daily doses for 20 days decreased AUC0-inf and Cmax of midazolam (a CYP3A4 substrate) by 13% and 15%, respectively, in healthy subjects.
- Oral Contraceptives. Coadministration of perampanel 4 mg once daily with an oral contraceptive containing ethinylestradiol 30 µg and levonorgestrel 150 µg for 21 days did not alter Cmax or AUC0-24h of either ethinylestradiol or levonorgestrel in healthy female subjects. In another study, a single dose of the oral contraceptive was administered following 21-day once daily dosing of FYCOMPA 12 mg or 8 mg in healthy females. FYCOMPA at 12 mg did not alter AUC0-24h of ethinylestradiol but decreased its Cmax by 18%, and also decreased Cmax and AUC0-24h of levonorgestrel by 42% and 40%, respectively. FYCOMPA at 8 mg did not have significant effect on Cmax or AUC0-24h of either ethinylestradiol or levonorgestrel, with a small decrease in AUC0-24h of levonorgestrel (9%).
- Levodopa. Perampanel administered as 4 mg once daily doses for 19 days had no effect on Cmax and AUC0-inf of levodopa in healthy subjects.
Nonclinical Toxicology
- Carcinogenesis
- Perampanel was administered orally to mice (1, 3, 10, or 30 mg/kg/day) and rats (10, 30, or 100 mg/kg/day in males; 3, 10, or 30 mg/kg/day in females) for up to 104 weeks. There was no evidence of drug-related tumors in either species. Plasma perampanel exposures (AUC) at the highest doses tested were less than that in humans dosed at 8 mg/day.
- Mutagenesis
- Perampanel was negative in the in vitro Ames and mouse lymphoma tk assays, and in the in vivo rat micronucleus assay.
- Impairment of Fertility
- In male and female rats administered perampanel (oral doses of 1, 10, or 30 mg/kg/day) prior to and throughout mating and continuing in females to gestation day 6, there were no clear effects on fertility. Prolonged and/or irregular estrus cycles were observed at all doses but particularly at the highest dose tested. Plasma perampanel exposures (AUC) at all doses were lower than that in humans dosed at 8 mg/day.
Clinical Studies
- The efficacy of FYCOMPA in partial-onset seizures, with or without secondary generalization, was studied in patients who were not adequately controlled with 1 to 3 concomitant AEDs in 3 randomized, double-blind, placebo-controlled, multicenter trials (Studies 1, 2, and 3) in adult and adolescent patients (aged 12 years and older). All trials had an initial 6-week Baseline Period, during which patients were required to have more than five seizures in order to be randomized. The Baseline Period was followed by a 19-week Treatment Period consisting of a 6-week Titration Phase and a 13-week Maintenance Phase. Patients in these 3 trials had a mean duration of epilepsy of approximately 21 years and a median baseline seizure frequency ranging from 9.3 to 14.3 seizures per 28 days. During the trials, more than 85% of patients were taking 2 to 3 concomitant AEDs with or without concurrent vagal nerve stimulation, and approximately 50% were on at least one AED known to induce CYP3A4, an enzyme critical to the metabolism of FYCOMPA (i.e., carbamazepine, oxcarbazepine, or phenytoin), resulting in a significant reduction in FYCOMPA’s serum concentration.
- Each study evaluated placebo and multiple FYCOMPA dosages (see Figure 1). During the Titration period in all 3 trials, patients on FYCOMPA received an initial 2 mg once daily dose, which was subsequently increased in weekly increments of 2 mg per day to the final target dose. Patients experiencing intolerable adverse reactions were permitted to have their dose reduced to the previously tolerated dose.
- The primary endpoint in Studies 1, 2, and 3 was the percent change in seizure frequency per 28 days during the Treatment Period as compared to the Baseline Period. The criterion for statistical significance was p<0.05. Table 3 shows the results of these studies. A statistically significant decrease in seizure rate was observed at doses of 4 to 12 mg per day. Dose response was apparent at 4 to 8 mg with little additional reduction in frequency at 12 mg per day.
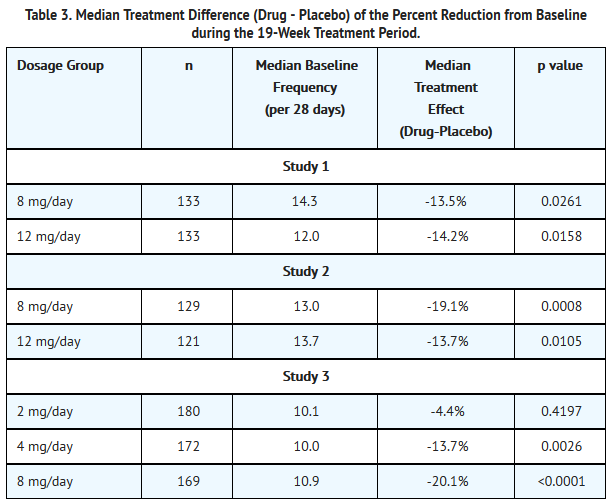
This image is provided by the National Library of Medicine.

- Table 4 presents an analysis combining data from all 3 studies, grouping patients based upon whether or not concomitant AED inducers (carbamazepine, oxcarbazepine, or phenytoin) were used. The analysis revealed a substantially reduced effect in the presence of inducers.
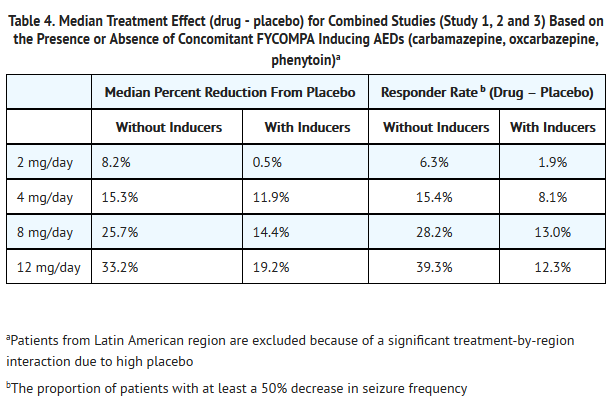
This image is provided by the National Library of Medicine.

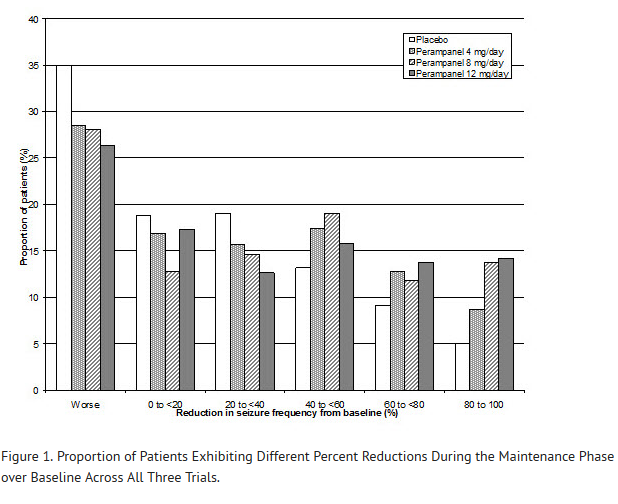
- Figure 1 shows the proportion of patients with different percent reductions during the maintenance phase over baseline across all three trials. Patients in whom the seizure frequency increased are shown at left as “worse.” Patients in whom the seizure frequency decreased are shown in the remaining five categories. Thus, the percentages of patients with a 40 to <60% reduction in seizure frequency were 13.2%, 17.4%, 19.0%, and 15.8% for placebo, 4, 8, and 12 mg, respectively.
This image is provided by the National Library of Medicine.

- The percentages of patients with a 50% or greater reduction in seizure frequency were 19.3%, 28.5%, 35.3%, 35.0% for placebo, 4, 8, and 12 mg, respectively.
How Supplied
- FYCOMPA (perampanel) Tablets 2 mg are orange, round, biconvex, film-coated tablets debossed with "2" on one side and "Є 275" on the other. They are supplied as follows:
- Bottles of 30 NDC 62856-272-30
- Bottles of 90 NDC 62856-272-90
- FYCOMPA (perampanel) Tablets 4 mg are red, round, biconvex, film-coated tablets debossed with "4" on one side and "Є 277" on the other. They are supplied as follows:
- Bottles of 30 NDC 62856-274-30
- Bottles of 90 NDC 62856-274-90
- FYCOMPA (perampanel) Tablets 6 mg are pink, round, biconvex, film-coated tablets debossed with "6" on one side and "Є 294" on the other. They are supplied as follows:
- Bottles of 30 NDC 62856-276-30
- Bottles of 90 NDC 62856-276-90
- FYCOMPA (perampanel) Tablets 8 mg are purple, round, biconvex, film-coated tablets debossed with "8" on one side and "Є 295" on the other. They are supplied as follows:
- Bottles of 30 NDC 62856-278-30
- Bottles of 90 NDC 62856-278-90
- FYCOMPA (perampanel) Tablets 10 mg are green, round, biconvex, film-coated tablets debossed with "10" on one side and "Є 296" on the other. They are supplied as follows:
- Bottles of 30 NDC 62856-280-30
- Bottles of 90 NDC 62856-280-90
- FYCOMPA (perampanel) Tablets 12 mg are blue, round, biconvex, film-coated tablets debossed with "12" on one side and "Є 297" on the other. They are supplied as follows:
- Bottles of 30 NDC 62856-282-30
- Bottles of 90 NDC 62856-282-90
- Storage
- Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F).
Storage
There is limited information regarding Perampanel Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Perampanel |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Perampanel |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
- Inform patients of the availability of a Medication Guide, and instruct them to read the Medication Guide prior to taking FYCOMPA. Instruct patients to take FYCOMPA only as prescribed.
- Serious Psychiatric and Behavioral Reactions
- Counsel patients, families and caregivers of patients of the need to monitor for the emergence of anger, aggression, hostility, unusual changes in mood, personality, or behavior, and other behavioral symptoms. Advise them to report any such symptoms immediately to their health care providers.
- Suicidal Thinking and Behavior
- Counsel patients, their caregivers, and families that AEDs, including FYCOMPA, may increase the risk of suicidal thinking and behavior and advise them of the need to be alert for the emergence or worsening of symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm. Instruct patients, caregivers and families to report behaviors of concern immediately to healthcare providers.
- Neurologic Effects: Dizziness, Gait Disturbance, Somnolence, and Fatigue
- Counsel patients that FYCOMPA may cause dizziness, gait disturbance, somnolence, and fatigue. Advise patients taking FYCOMPA not to drive, operate complex machinery, or engage in other hazardous activities until they have become accustomed to any such effects associated with FYCOMPA.
- Falls
- Counsel patients that FYCOMPA may cause falls and injuries.
- Withdrawal of Antiepileptic Drugs
- Counsel patients that abrupt discontinuation of FYCOMPA may increase seizure frequency.
- Contraceptives
- Counsel patients that FYCOMPA may decrease efficacy of contraceptives containing levonorgestrel.
- Alcohol and Other CNS Depressants
- Counsel patients that FYCOMPA may enhance the impairment effects of alcohol. These effects may also be seen if FYCOMPA is taken with other CNS depressants.
- Missed Doses
- Counsel patients that if they miss a dose, they should resume dosing the following day at their prescribed daily dose. Instruct patients to contact their physician if more than one day of dosing is missed.
- Controlled Substance
- Counsel patients that FYCOMPA is a controlled substance that can be misused and abused.
- Pregnancy Registry
- To provide information regarding the effects of in utero exposure to FYCOMPA, recommend pregnant patients treated with FYCOMPA to enroll in the NAAED Pregnancy Registry. This can be done by calling the toll free number 1-888-233-2334, and must be done by patients themselves. Information on the registry can also be found at the website http://www.aedpregnancyregistry.org.

This image is provided by the National Library of Medicine.

Precautions with Alcohol
- Alcohol-Perampanel interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- FYCOMPA®[2]
Look-Alike Drug Names
There is limited information regarding Perampanel Look-Alike Drug Names in the drug label.
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Yang, X; Wu T-C; Yuxin Men A; Lee J-Y; Bhattaram VA; Mehta MU. "U.S. FDA Clinical Pharmacology Review. Fycompa™ (perampanel)" (PDF): 25.
- ↑ "FYCOMPA perampanel tablet".
{{#subobject:
|Page Name=Perampanel |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel06.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel07.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel08.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel09.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel10.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel11.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel12.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel13.png
}}
{{#subobject:
|Label Page=Perampanel |Label Name=Perampanel14.png
}}