Accessory nerve
Template:Infobox Nerve Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
In anatomy, the accessory nerve is a nerve that controls specific muscles of the neck. As a part of it is traditionally believed to originate in the brain, it is considered a cranial nerve. Based on its location relative to other such nerves, it is designated the eleventh of twelve cranial nerves, and is thus abbreviated CN XI. Although anatomists typically refer to the accessory nerve in singular, there are in reality two accessory nerves, one on each side of the body.
Traditional descriptions of the accessory nerve divide it into two parts: a spinal part and a cranial part.[1] But because the cranial component rapidly joins the vagus nerve and serves the same function as other vagal nerve fibers, modern descriptions often consider the cranial component part of the vagus nerve and not part of the accessory nerve proper.[2] Thus in contemporary discussions of the accessory nerve, the common practice is to dismiss the cranial part altogether, referring to the accessory nerve specifically as the spinal accessory nerve.
The spinal accessory nerve provides motor innervation from the central nervous system to two muscles of the neck: the sternocleidomastoid muscle and the upper part of the trapezius muscle. The sternocleidomastoid muscle tilts and rotates the head, while the trapezius muscle has several actions on the scapula, including shoulder elevation.
Range of motion and strength testing of the neck and shoulders can be measured during a neurological examination to assess function of the spinal accessory nerve. Limited range of motion or poor muscle strength are suggestive of damage to the spinal accessory nerve, which can result from a variety of causes. Injury to the spinal accessory nerve is most commonly caused by medical procedures that involve the head and neck.[3]
Anatomy
Course

Like other cranial nerves, the spinal accessory nerve begins in the central nervous system and exits the cranium through a specialized hole (or foramen). However, unlike all other cranial nerves, the spinal accessory nerve begins outside the skull rather than inside. In particular, in the majority of individuals, the fibers of the spinal accessory nerve originate solely in neurons situated in the upper spinal cord.[4] These fibers coalesce to form spinal rootlets, roots, and finally the spinal accessory nerve itself, which enters the skull through the foramen magnum, the large opening at the base of the skull. The nerve courses along the inner wall of the skull towards the jugular foramen, through which it exits the skull with the glossopharyngeal (CN IX) and vagus nerves (CN X). Owing to its peculiar course, the spinal accessory nerve is notable for being the only cranial nerve to both enter and exit the skull.
Traditionally, the accessory nerve is described as having a small cranial component that descends from the medulla oblongata and briefly connects with the spinal accessory component before branching off of the nerve to join the vagus nerve. A recent study of twelve subjects suggests that in the majority of individuals, this cranial component does not make any distinct connection to the spinal component; the roots of these distinct components were separated by a fibrous sheath in all but one subject.[4]
Once the cranial component has detached from the spinal component, the spinal accessory nerve continues alone and heads posteriorly (backwards) and inferiorly (downwards) upon exiting the skull. It pierces the sternocleidomastoid muscle while sending it motor branches, then continues inferiorly until it reaches the trapezius muscle to provide motor innervation to its upper portion.
Origin
The fibers that form the spinal accessory nerve are formed by lower motor neurons located in the upper segments of the spinal cord. This cluster of neurons, called the spinal accessory nucleus, is located in the lateral horn of the spinal cord. This is in contrast to most other motor neurons, whose cell bodies are found in the spinal cord's anterior horn. The lateral horn of high cervical segments appears to be continuous with the nucleus ambiguus of the medulla oblongata, from which the cranial component of the accessory nerve is derived.
Classification
Among investigators there is disagreement regarding the terminology used to describe the type of information carried by the accessory nerve. As the trapezius and sternocleidomastoid muscles are derived from the branchial arches, some investigators believe the spinal accessory nerve that innervates them must carry branchiomeric (special visceral efferent, SVE) information.[5] This is in line with the observation that the spinal accessory nucleus appears to be continuous with the nucleus ambiguus of the medulla. Others, notably Haines, consider the spinal accessory nerve to carry general somatic efferent (GSE) information.[6] Still others believe it is reasonable to conclude that the spinal accessory nerve contains both SVE and GSE components.[7]
Injury
Injury to the spinal accessory nerve can cause an accessory nerve disorder or spinal accessory nerve palsy, which results in diminished or absent function of the sternocleidomastoid muscle and upper portion of the trapezius muscle. Patients with spinal accessory nerve palsy often exhibit signs of lower motor neuron disease such as diminished muscle mass, fasciculations, and partial paralysis of the sternocleidomastoid and trapezius muscles.
History and etymology
In 1848, Jones Quain described the nerve as the "spinal nerve accessory to the vagus", recognizing that while a minor component of the nerve joins with the larger vagus nerve, the majority of accessory nerve fibers originate in the spinal cord.[8] Quain also suggested spinal accessory nerve as a shortened form of the term; this term, and its more abbreviated variant, accessory nerve, have persisted to modern times. Throughout this interval, the nerve has never had a consistent name among investigators and medical practitioners. Some use accessory nerve and spinal accessory nerve interchangeably; others distinguish between spinal accessory nerve and cranial accessory nerve; still others use accessory nerve to refer to both spinal and cranial components of the nerve.
In Neuroanatomy and the Neurologic Exam, Terence R. Anthoney provides a historical account of the usage of the terms accessory nerve, spinal accessory nerve, and cranial accessory nerve, summarized in the following excerpt:
To summarize, then, the eleventh cranial nerve was called both the "accessory nerve" and the "spinal accessory nerve" as early as 1848—"accessory" referring to its fibers which became accessory to the vagus nerve and "spinal" referring to its largely spinal origin. When it became recognized, as early as 1893, that the "accessory" fibers to the vagus nerve came from the same medullary nuclei as the rest of the vagal efferent fibers, people began to view the "accessory" fibers as part of the vagus nerve proper, leaving the eleventh cranial nerve to originate solely from its spinal nucleus. This shift was reinforced by the neuroclinicians, who could only test the integrity of the spinal portion of the nerve separately anyway. Because of the shift to just a spinal origin for the nerve, the word "accessory" came to be associated with the "true"—i.e., spinal—component of the nerve,no longer being considered in the context of "accessory to the vagus." This association has been reinforced by referring to the spinal nucleus of origin as the "(spinal) accessory nucleus."[9]
Additional images
-
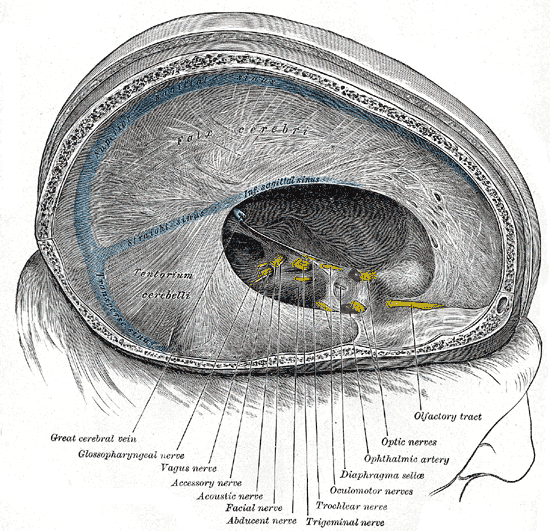
Dura mater and its processes exposed by removing part of the right half of the skull, and the brain.
-
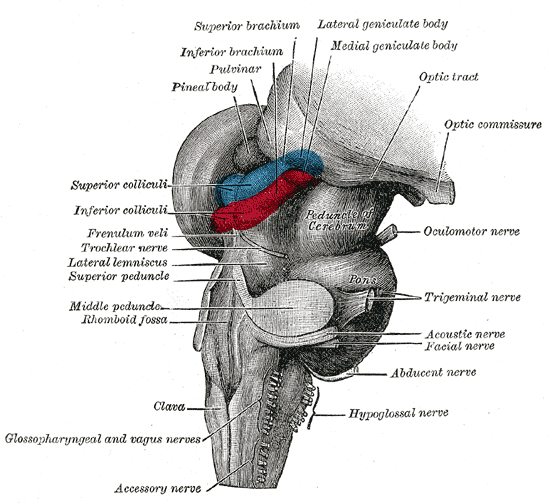
Hind- and mid-brains; postero-lateral view.
-
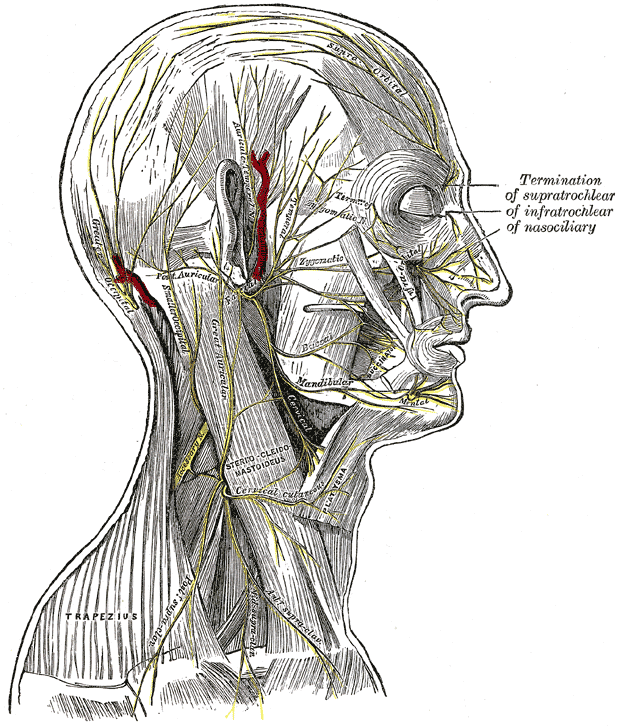
The nerves of the scalp, face, and side of neck.
-
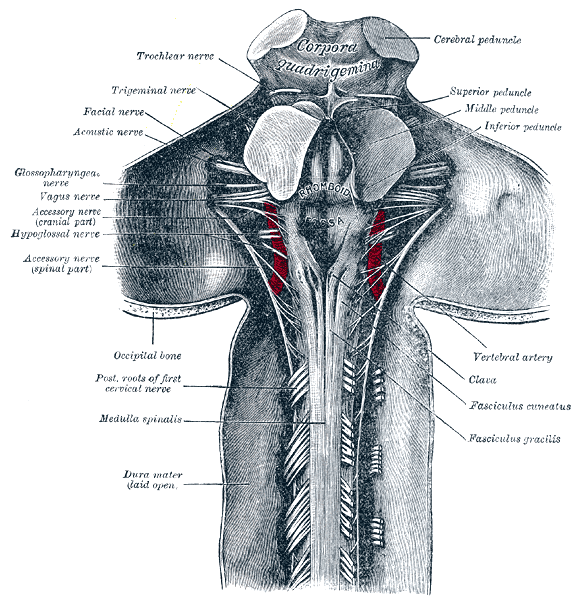
Upper part of medulla spinalis and hind- and mid-brains; posterior aspect, exposed in situ.
-
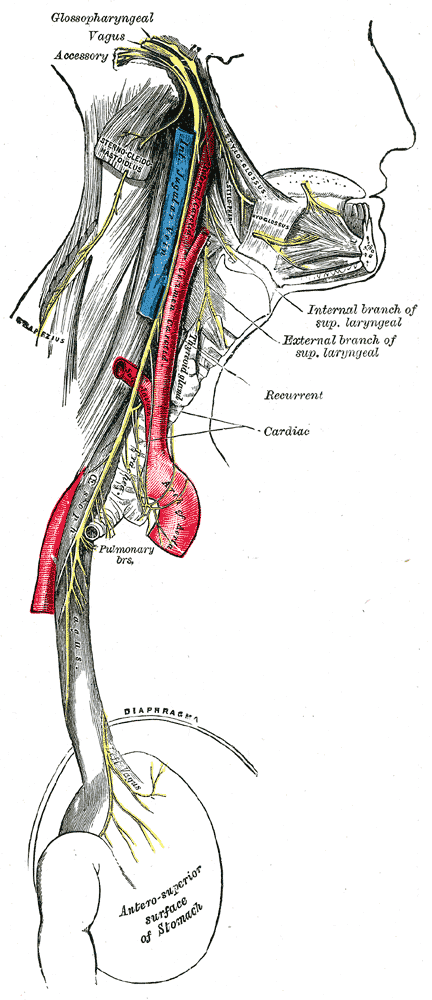
Course and distribution of the glossopharyngeal, vagus, and accessory nerves.
-
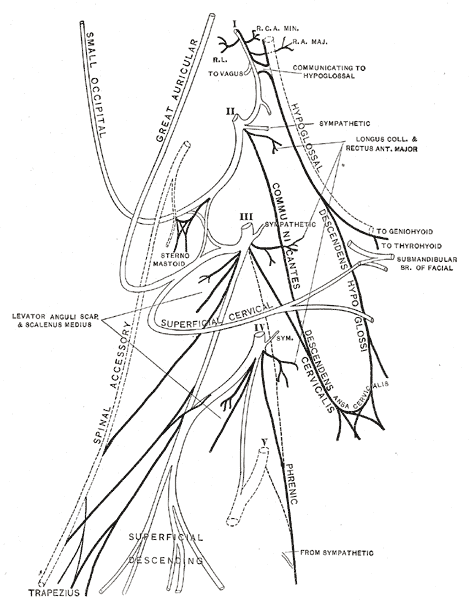
Plan of the cervical plexus.
-

Side of neck, showing chief surface markings.






References
- ↑ "The Accessory Nerve". Gray's Anatomy of the Human Body.
- ↑ "Spinal Accessory Nerve". Structure of the Human body, Loyola University Medical Education Network.
- ↑ London J, London NJ, Kay SP (1996). "Iatrogenic accessory nerve injury". Annals of the Royal College of Surgeons of England. 78 (2): 146–50. PMID 8678450.
- ↑ 4.0 4.1 Ryan S, Blyth P, Duggan N, Wild M, Al-Ali S (2007). "Is the cranial accessory nerve really a portion of the accessory nerve? Anatomy of the cranial nerves in the jugular foramen". Anatomical science international / Japanese Association of Anatomists. 82 (1): 1–7. PMID 17370444.
- ↑ William T. Mosenthal. A Textbook of Neuroanatomy: With Atlas and Dissection Guide. Washington, DC: Taylor & Francis. pp. p. 12. ISBN 1-85070-587-9.
- ↑ Duane E. Haines (2004). Neuroanatomy: an atlas of structures, sections, and systems. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-4677-9.
- ↑ Joshi SS, Joshi SD (2001). "Muscle Dorso-Fascialis — A Case Report". Journal of the Anatomical Society of India. 50 (2): 159–160.
- ↑ Jones Quain (1848). Richard Quain, William Sharpey, ed. Elements of Anatomy. 2 (5th ed. ed.). London: Taylor, Walton, and Maberly. pp. p. 812.
- ↑ Terence R. Anthoney (1993). Neuroanatomy and the Neurologic Exam: A Thesaurus of Synonyms, Similar-Sounding Non-Synonyms, and Terms of Variable Meanings. Boca Raton: CRC-Press. pp. pp. 69-73. ISBN 0-8493-8631-4.
External links
- Template:LoyolaMedEd
- Template:NormanAnatomy
- Template:NormanAnatomy (Template:NormanAnatomyFig)
- Template:SUNYAnatomyLabs
- Template:YaleCranialNerves
de:Nervus accessorius
it:Nervo accessorio
lt:Priedinis nervas
nl:Nervus accessorius
no:Nervus accessorius
tl:Aksesoring litid